📋 Key Information Summary
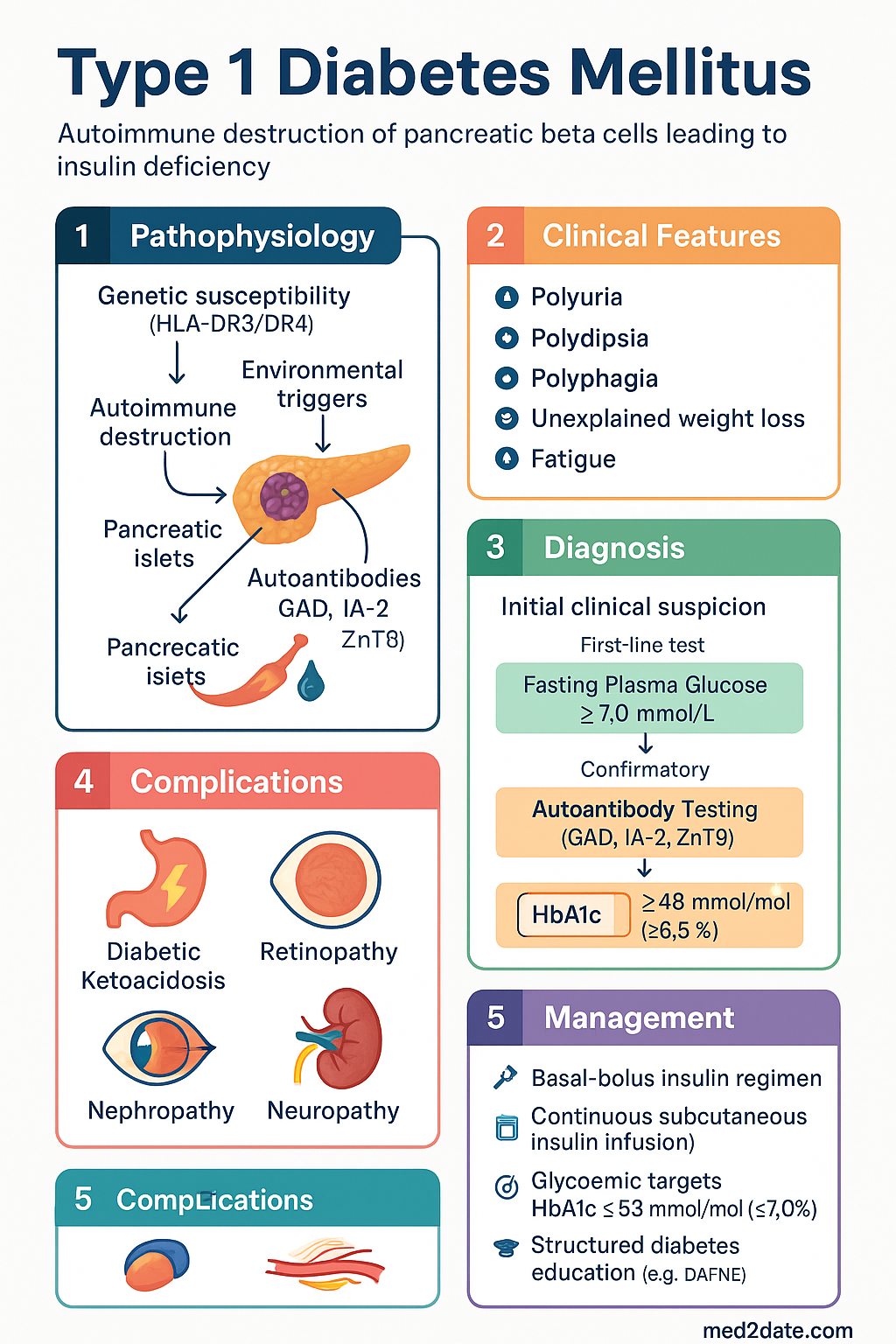
- Type 1 Diabetes Mellitus (T1DM) is an autoimmune condition leading to absolute insulin deficiency, requiring lifelong exogenous insulin.
- Diagnosis is typically made in childhood/young adulthood but can occur at any age. Presentation is often acute with hyperglycaemia and possible diabetic ketoacidosis (DKA).
- In Australia, incidence is rising, particularly in children aged 0–14 years. Genetic susceptibility (HLA-DR3/DR4) and environmental triggers are implicated.
- Diagnostic criteria include hyperglycaemia (random ≥11.1 mmol/L, fasting ≥7.0 mmol/L, or HbA1c ≥6.5%) with symptoms, and positive autoantibodies (GAD, IA-2, ZnT8).
- Management requires a basal-bolus insulin regimen or continuous subcutaneous insulin infusion (insulin pump) to mimic physiological insulin secretion.
- Glycaemic targets for most adults: HbA1c ≤53 mmol/mol (≤7.0%), pre-meimal BGL 5–7 mmol/L, and post-meal BGL 5–10 mmol/L, individualised to avoid hypoglycaemia.
- Diabetes-related complications (microvascular: retinopathy, nephropathy, neuropathy; macrovascular: CVD) are delayed by intensive glycaemic control and management of cardiovascular risk factors.
- Structured diabetes education (e.g., DAFNE, OzDAFNE) is a cornerstone of care to empower patients in carbohydrate counting and insulin dose adjustment.
- Hypoglycaemia is the major acute complication of insulin therapy. Severe hypoglycaemia requires glucagon (parenteral or intranasal) for management.
- Annual screening for complications is mandatory, including retinal photography, urine albumin-to-creatinine ratio, foot examination, and cardiovascular risk assessment.
- Aboriginal and Torres Strait Islander peoples have a higher prevalence of diabetes complications. Culturally safe care, access to services, and addressing social determinants are critical.
🎧 Audio Brief
Introduction & Australian Epidemiology
Type 1 Diabetes Mellitus (T1DM) is a chronic autoimmune disorder characterised by T-cell mediated destruction of pancreatic beta cells, resulting in absolute insulin deficiency. Without exogenous insulin, individuals with T1DM develop life-threatening hyperglycaemia and ketoacidosis. In Australia, T1DM accounts for approximately 10–15% of all diabetes cases, but it is the most common form of diabetes in children and adolescents.
Australia has one of the highest incidences of childhood T1DM globally. According to the Australian Institute of Health and Welfare (AIHW), the incidence in children aged 0–14 years has increased by approximately 3.0% per year over recent decades. The condition has a significant genetic component, with over 50% of the risk attributed to HLA region genes on chromosome 6p21 (particularly HLA-DR3 and HLA-DR4 haplotypes). However, environmental factors such as viral infections, early infant diet, and gut microbiome alterations are also thought to contribute to triggering the autoimmune process.
The management of T1DM in Australia is guided by the National Evidence-Based Clinical Care Guidelines for Type 1 Diabetes in Children, Adolescents and Adults, the Royal Australian College of General Practitioners (RACGP) General Practice Management of Type 2 Diabetes (with principles applicable to T1DM), and local state/territory health service protocols. The primary goal is to achieve glycaemic targets as close to normal as safely possible to prevent acute complications and delay the onset of long-term microvascular and macrovascular complications.
Pathophysiology & Genetics
T1DM results from the autoimmune destruction of insulin-producing beta cells within the pancreatic islets of Langerhans. This process is mediated by autoreactive T-lymphocytes (both CD4+ and CD8+ T-cells) and is associated with the production of circulating autoantibodies.
Genetic Susceptibility
The strongest genetic risk comes from the HLA class II genes on chromosome 6p21, which account for approximately 40–50% of the genetic risk. Key high-risk haplotypes include:
- HLA-DR3-DQ2 (DRB1*03:01–DQA1*05:01–DQB1*02:01)
- HLA-DR4-DQ8 (DRB1*04:01–DQA1*03:01–DQB1*03:02)
The heterozygous DR3/DR4 genotype carries the highest risk. Non-HLA genes also contribute, including the insulin gene (INS) variable number tandem repeat (VNTR) on chromosome 11p15, PTPN22, CTLA4, and IL2RA.
Autoimmune Process
The autoimmune attack is thought to be triggered in genetically susceptible individuals by an environmental factor (e.g., enteroviral infection, particularly Coxsackie B virus, or dietary factors). This leads to insulitis (inflammation of the islets) and a gradual decline in beta-cell mass. Clinical diabetes manifests when approximately 80–90% of beta-cell function is lost. The presence of autoantibodies—glutamic acid decarboxylase (GAD65), insulinoma-associated antigen-2 (IA-2), zinc transporter 8 (ZnT8), and insulin autoantibodies (IAA)—serves as markers of this ongoing autoimmune process and is crucial for diagnosis and classification.
Clinical Features & Diagnosis
Presentation
The classic presentation, often in children and adolescents, is acute to sub-acute, developing over days to weeks. Key features include the "polys" and weight loss:
- Polyuria: Osmotic diuresis from glucosuria.
- Polydipsia: Compensatory thirst due to dehydration.
- Polyphagia: Hunger from cellular starvation, often with paradoxical weight loss.
- Unexplained weight loss: Due to catabolism of fat and muscle.
- Fatigue and lethargy.
In a significant proportion of children, the initial presentation is with diabetic ketoacidosis (DKA) (see Complications section). In adults, the onset may be more gradual, sometimes termed Latent Autoimmune Diabetes in Adults (LADA).
Diagnostic Criteria
Diagnosis is based on the presence of hyperglycaemia with clinical features, and does not always require autoantibody confirmation if the presentation is unequivocal. Diagnostic criteria (any one of the following):
| Test | Diagnostic Threshold | Notes |
|---|---|---|
| Fasting Plasma Glucose | ≥ 7.0 mmol/L | No caloric intake for ≥8 hours. |
| 2-hour Plasma Glucose (OGTT) | ≥ 11.1 mmol/L | 75g oral glucose load. |
| Random Plasma Glucose | ≥ 11.1 mmol/L | Classic hyperglycaemic symptoms or hyperglycaemic crisis must be present. |
| Glycated Haemoglobin (HbA1c) | ≥ 48 mmol/mol (≥6.5%) | NGSP/DCCT standardised. Use with caution in children, pregnancy, or conditions affecting RBC turnover. |
Autoantibody Testing: In ambiguous cases (e.g., type 2 phenotype in a young adult), testing for GAD65, IA-2, and ZnT8 autoantibodies is recommended to confirm autoimmune aetiology and distinguish from type 2 diabetes or monogenic diabetes.
Insulin Regimens & Targets
All individuals with T1DM require a physiologic insulin replacement regimen. The choice of regimen depends on patient preference, lifestyle, age, and hypoglycaemia risk.
Insulin Types & Pharmacokinetics
Regimen Types
Glycaemic Targets
Targets must be individualised to avoid severe hypoglycaemia, considering hypoglycaemia awareness, duration of diabetes, and comorbidities.
| Parameter | Target (Adults) | Target (Children/Adolescents) |
|---|---|---|
| HbA1c | ≤ 53 mmol/mol (≤7.0%) for most; 48 mmol/mol (≤6.5%) if safely achievable. | < 58 mmol/mol (<7.5%) for most, individualised. |
| Pre-meal BGL | 5.0–7.0 mmol/L | 4.0–8.0 mmol/L |
| Post-meal BGL (1-2 hrs) | 5.0–10.0 mmol/L | 5.0–10.0 mmol/L |
| Time in Range (CGM, 3.9-10 mmol/L) | >70% | >50–70% |
| Time Below Range (<3.9 mmol/L) | <4% | <4% |
Complications & Monitoring
Acute Complications
Chronic Microvascular Complications
Risk is directly related to duration of diabetes and degree of glycaemic control. Intensive management reduces risk. Annual screening is mandatory.
| Complication | Screening Test & Frequency | MBS Item | Management Notes |
|---|---|---|---|
| Retinopathy | Retinal photography (dilated pupils) every 2 years (low risk), annually (high risk). | 10850, 10851 | Refer to ophthalmology for any referable retinopathy. Optimal BGL & BP control. |
| Nephropathy | Annual urine Albumin-to-Creatinine Ratio (uACR) & eGFR. | 66830, 66833 | ACEi/ARB for albuminuria (UACR >2.5 mg/mmol men, >3.5 mg/mmol women). SGLT2i may be used in T1DM with CKD under specialist guidance. |
| Neuropathy | Annual clinical foot exam: 10g monofilament, 128 Hz tuning fork (vibration), ankle reflexes, pin-prick sensation. | N/A (clinical exam) | Multifactorial risk reduction. Pregabalin or duloxetine for painful neuropathy. |
Cardiovascular Risk Management
T1DM confers a high absolute risk of CVD. Management focuses on all modifiable risk factors.
- Blood Pressure: Target <130/80 mmHg. First-line: ACE inhibitor or ARB.
- Lipids: High-intensity statin (e.g., Atorvastatin 40–80 mg) recommended for most adults with T1DM aged >40, or earlier if additional risk factors.
- Smoking Cessation: Absolute priority.
Investigations
Beyond diagnostic testing, ongoing monitoring is essential.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Type 1 Diabetes in Aboriginal and Torres Strait Islander peoples requires a culturally safe and holistic approach, acknowledging the higher burden of complications and the impact of systemic disadvantage.
📚 References
- 1. Craig ME, Jefferies C, Dabelea D, Balde N, Seth A, Donaghue KC. ISPAD Clinical Practice Consensus Guidelines 2022: Diabetes education in children and adolescents. Pediatric Diabetes. 2022;23(8):1229-1242.
- 2. Royal Australian College of General Practitioners (RACGP). General practice management of type 2 diabetes: 2024–2025. Melbourne: RACGP; 2024.
- 3. National Diabetes Services Scheme (NDSS). Continuous Glucose Monitoring (CGM) Initiative. Australian Government Department of Health and Aged Care. Accessed 2024.
- 4. Diabetes Australia. Position Statement: Continuous Glucose Monitoring. Canberra: Diabetes Australia; 2023.
- 5. The Royal Australasian College of Physicians (RACP). National Evidence-Based Clinical Care Guidelines for Type 1 Diabetes in Children, Adolescents and Adults. Australian Government Department of Health and Ageing, 2011.
- 6. American Diabetes Association Professional Practice Committee. Standards of Care in Diabetes—2024. Diabetes Care. 2024;47(Supplement 1):S1–S321.
- 7. Australian Institute of Health and Welfare (AIHW). Diabetes: Australian facts. Canberra: AIHW; 2023.
- 8. Joint British Diabetes Societies (JBDS) for Inpatient Care. Management of Diabetic Ketoacidosis in Adults. 2023 Update.
- 9. National Aboriginal Community Controlled Health Organisation (NACCHO). NACCHO Aboriginal and Torres Strait Islander Diabetes Framework. Canberra: NACCHO; 2023.
- 10. DAFNE Study Group. Training in flexible, intensive insulin management to enable dietary freedom in people with type 1 diabetes: dose adjustment for normal eating (DAFNE) randomised controlled trial. BMJ. 2002;325(7367):746.