📋 Key Information Summary
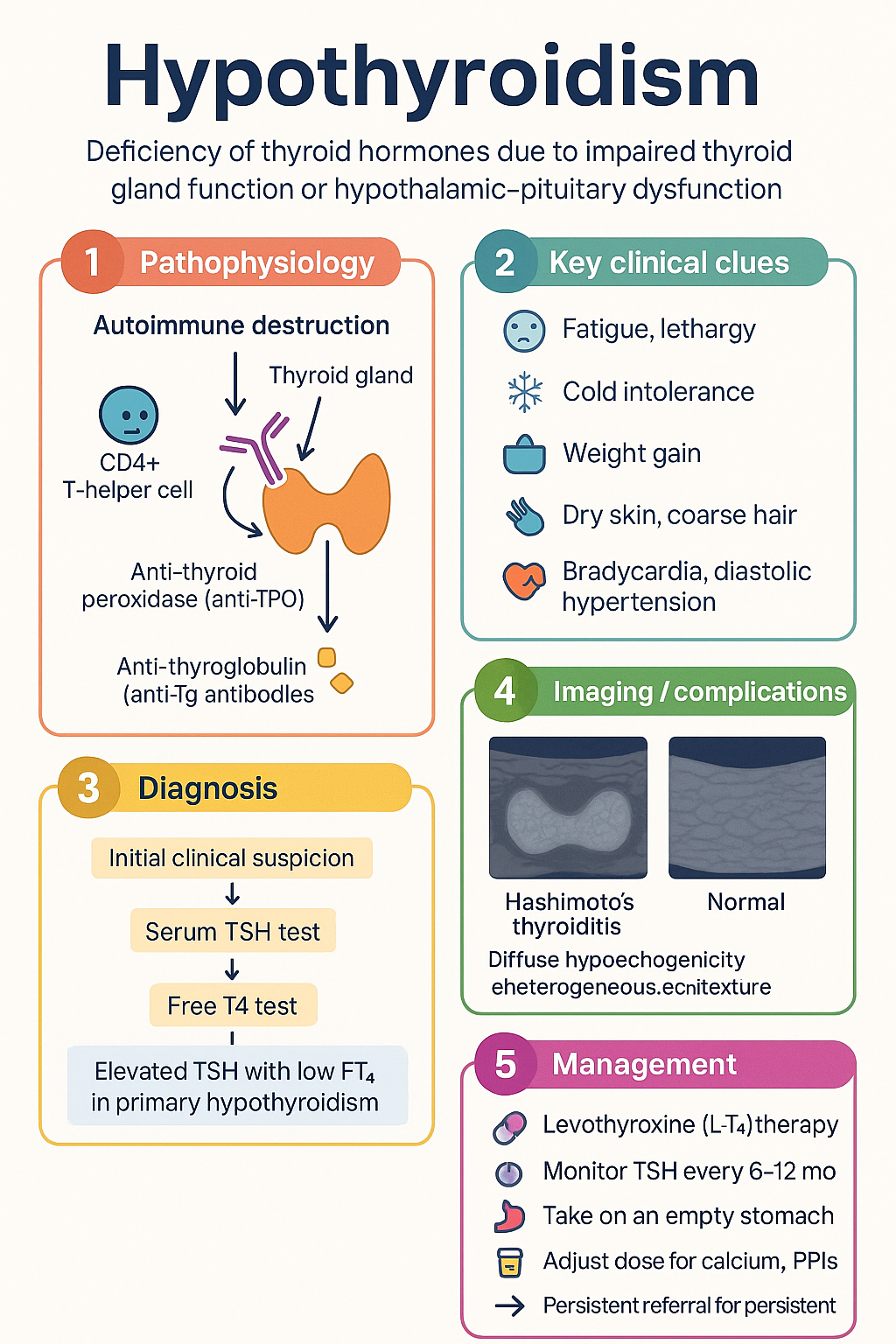
- Hypothyroidism is a deficiency of thyroid hormones (T3 and T4) resulting from impaired thyroid gland function (primary) or hypothalamic–pituitary dysfunction (secondary/central).
- Hashimoto's thyroiditis (chronic autoimmune thyroiditis) is the most common cause in iodine-replete populations such as Australia.
- The hallmark biochemical finding is an elevated serum TSH with low free T4 (FT4) in primary hypothyroidism; secondary hypothyroidism presents with low or inappropriately normal TSH and low FT4.
- Levothyroxine (L-T4) is the standard replacement therapy — e.g., Oroxine®, Eutroxsig® — initiated at 1.6 µg/kg/day in healthy young adults; lower starting doses in the elderly and cardiac disease.
- TSH should be measured 6–8 weeks after initiation or dose change, then every 6–12 months once stable; target TSH typically 0.4–4.0 mIU/L.
- Levothyroxine must be taken on an empty stomach 30–60 minutes before breakfast; concurrent calcium, iron, and PPIs impair absorption and require dose adjustment.
- Subclinical hypothyroidism (elevated TSH, normal FT4) is common; treatment is recommended when TSH >10 mIU/L or TSH 5–10 mIU/L with symptoms, positive TPO antibodies, or pregnancy intent.
- In pregnancy, the TSH upper reference limit is lower (trimester-specific); untreated hypothyroidism increases risk of miscarriage, pre-eclampsia, and impaired neurodevelopment.
- Myxoedema coma is a rare, life-threatening emergency requiring IV levothyroxine, IV hydrocortisone, ICU admission, and management of hypothermia and hyponatraemia.
- Aboriginal and Torres Strait Islander peoples have higher rates of autoimmune disease; screening and access to thyroid function testing in remote communities must be prioritised.
- Levothyroxine (Oroxine®, Eutroxsig®, generic L-T4) is PBS-listed as a General Benefit — no Authority required.
🎧 Audio Brief
Introduction & Australian Epidemiology
Hypothyroidism is a common endocrine disorder characterised by deficient production or action of thyroid hormones — thyroxine (T4) and triiodothyronine (T3) — resulting in a global reduction of metabolic activity. It is classified as primary (thyroid gland failure, >95 % of cases) or secondary/central (pituitary or hypothalamic disease).
Australia is an iodine-replete nation following the mandatory iodisation of bread salt (2009), and the overall prevalence of overt hypothyroidism is approximately 1–2 %, with subclinical hypothyroidism affecting an additional 4–10 % of adults depending on assay cut-offs. Women are 5–8 times more likely to be affected than men, and prevalence rises sharply with age — reaching 10–15 % in women over 60 years.
Hashimoto's thyroiditis (chronic lymphocytic / autoimmune thyroiditis) is the single most common aetiology in Australia, followed by iatrogenic causes — radioiodine (I-131) therapy and thyroidectomy for Graves' disease or thyroid carcinoma. Less common causes include drug-induced hypothyroidism (amiodarone, lithium, immune checkpoint inhibitors), iodine deficiency or excess, infiltrative diseases, and congenital hypothyroidism (detected via the Australian Newborn Bloodspot Screening Programme).
Hypothyroidism is readily diagnosed with a single serum TSH measurement and is one of the most satisfying conditions in endocrinology to treat, with near-complete symptom resolution in the majority of patients on appropriate levothyroxine replacement. Nevertheless, persistent symptoms despite biochemically normal TSH levels remain a clinical challenge and necessitate careful re-evaluation of adherence, absorption, comorbidities, and patient expectations.
Aetiology & Pathophysiology
The thyroid gland produces T4 (the predominant secretory product) and smaller quantities of T3 (the biologically active hormone). Thyroid hormone synthesis is regulated by the hypothalamic–pituitary–thyroid (HPT) axis via TRH → TSH → thyroid hormone negative feedback.
Primary Hypothyroidism
Destruction or dysfunction of the thyroid gland leads to reduced T4/T3 output and loss of negative feedback, resulting in compensatory TSH elevation. Causes include:
- Hashimoto's thyroiditis — the most common cause worldwide and in Australia. An autoimmune process mediated by CD4+ T-helper cells, anti-thyroid peroxidase (anti-TPO) antibodies, and anti-thyroglobulin (anti-Tg) antibodies. Lymphocytic infiltration gradually replaces functional thyroid tissue with fibrosis. Progression from euthyroidism → subclinical → overt hypothyroidism occurs at ~5 % per year in antibody-positive individuals.
- Iatrogenic — radioiodine (I-131) ablation for Graves' disease or thyroid cancer (hypothyroidism develops in 50–80 % within 5–10 years); total thyroidectomy; external beam radiotherapy to the neck.
- Drug-induced — amiodarone (type 2 amiodarone-induced thyroiditis or inhibition of 5'-deiodinase); lithium (inhibits thyroid hormone release); immune checkpoint inhibitors (ipilimumab, nivolumab, pembrolizumab — thyroiditis with subsequent hypothyroidism in 5–20 %); tyrosine kinase inhibitors (lenvatinib, sunitinib); interferon-α; interleukin-2.
- Iodine deficiency — historically the leading cause globally; now uncommon in Australia due to mandatory iodisation programmes, but mild deficiency persists in some regions (e.g., parts of Tasmania, some Aboriginal and Torres Strait Islander communities).
- Iodine excess — the Wolff–Chaikoff effect; excess iodine transiently inhibits thyroid hormone synthesis. Relevant in patients receiving iodinated contrast, amiodarone, or Lugol's iodine.
- Infiltrative diseases — amyloidosis, sarcoidosis, haemochromatosis, Riedel's thyroiditis, Langerhans cell histiocytosis.
- Congenital — thyroid dysgenesis (agenesis, ectopy) accounts for ~85 %; dyshormonogenesis (inborn errors of thyroid hormone synthesis) ~15 %. Detected by the Australian Newborn Bloodspot Screening Programme (heel-prick TSH at 48–72 hours).
Secondary (Central) Hypothyroidism
Caused by insufficient TSH secretion from the pituitary or TRH from the hypothalamus. Causes include pituitary adenomas, craniopharyngiomas, pituitary surgery or radiotherapy, Sheehan syndrome, lymphocytic hypophysitis, sarcoidosis, and haemochromatosis. Key diagnostic feature: low or inappropriately normal TSH with low FT4 — TSH is not a reliable marker for monitoring replacement in these patients.
Subclinical Hypothyroidism
Defined biochemically as elevated TSH (typically 4.5–10 mIU/L) with normal FT4. Represents early thyroid failure. Most patients are asymptomatic or have non-specific symptoms. Approximately 2–5 % progress to overt hypothyroidism annually, particularly if TPO-antibody positive. Management remains controversial; treatment is generally recommended when TSH >10 mIU/L or with symptoms, positive antibodies, pregnancy planning, or cardiovascular risk factors.
Clinical Features
The clinical presentation of hypothyroidism is insidious and often non-specific, leading to delayed diagnosis. Symptoms correlate with the degree and duration of thyroid hormone deficiency and the patient's age. Many features are absent in mild or subclinical disease.
Common Symptoms
| System | Symptoms & Signs |
|---|---|
| Constitutional | Fatigue, lethargy, cold intolerance, weight gain (usually modest, 2–5 kg), hypothermia |
| Dermatological | Dry skin, coarse hair, hair loss (including lateral third of eyebrows — Queen Anne sign), brittle nails, myxoedema (non-pitting oedema of skin, especially periorbital) |
| Cardiovascular | Bradycardia, diastolic hypertension, pericardial effusion, elevated LDL cholesterol, accelerated atherosclerosis |
| Neuropsychiatric | Cognitive slowing, poor concentration, depression, carpal tunnel syndrome, delayed deep tendon reflexes (prolonged relaxation phase) |
| Gastrointestinal | Constipation, reduced appetite |
| Musculoskeletal | Myalgia, arthralgia, proximal muscle weakness, elevated CK |
| Reproductive | Menorrhagia, oligomenorrhoea, infertility, erectile dysfunction, hyperprolactinaemia (galactorrhoea) |
| Haematological | Macrocytic or normocytic anaemia |
| ENT | Goitre (Hashimoto's), hoarse voice, macroglossia |
Myxoedema Coma
Myxoedema coma is a rare but life-threatening decompensation of severe, untreated hypothyroidism with a mortality rate of 25–60 %. It typically occurs in elderly patients with longstanding undiagnosed hypothyroidism, precipitated by infection, surgery, cold exposure, sedatives, or medication non-adherence.
- Profound hypothermia (<35 °C)
- Altered consciousness — confusion → stupor → coma
- Severe bradycardia, hypotension
- Hypoventilation with respiratory failure (CO₂ retention)
- Hyponatraemia (dilutional, impaired free water excretion)
- Hypoglycaemia
Investigations & Diagnosis
Diagnosis of primary hypothyroidism is biochemical, centred on serum TSH and FT4. Clinical history, examination, and antibody testing assist in determining the aetiology.
First-Line Investigations
Diagnostic Interpretation
| Pattern | TSH | FT4 | Interpretation |
|---|---|---|---|
| Overt primary hypothyroidism | ↑↑ (typically >10) | ↓ | Confirmed; treat with levothyroxine |
| Subclinical hypothyroidism | ↑ (4.5–10) | Normal | Consider treatment if TPO+, symptomatic, or TSH >10 |
| Central hypothyroidism | Low or inappropriately normal | ↓ | Suspect pituitary/hypothalamic pathology; MRI pituitary |
| Isolated TSH elevation | Mildly ↑ | Normal | Repeat in 6–8 weeks; consider assay interference, heterophilic antibodies, macro-TSH |
Additional Investigations
- Thyroid ultrasound: Not routinely required for diagnosis. Indicated if goitre, palpable nodule, or asymmetric thyroid enlargement. Features of Hashimoto's include diffuse hypoechogenicity, heterogeneous echotexture, and fibrous septations.
- FBC: Normocytic or macrocytic anaemia.
- Lipid profile: Hypercholesterolaemia (↑ LDL) and occasionally hypertriglyceridaemia. Should improve with adequate replacement.
- Serum CK: Often elevated (2–10× normal) in overt hypothyroidism — a common source of unnecessary investigation for myopathy.
- Sodium: Hyponatraemia (dilutional) may be present.
- Prolactin: Mildly elevated due to TRH stimulation of lactotrophs. Galactorrhoea may occur.
- MRI pituitary: Required if central hypothyroidism suspected to exclude structural lesion.
Management (Levothyroxine)
Levothyroxine (L-T4, synthetic thyroxine) is the standard and preferred replacement therapy for all forms of hypothyroidism. It is a prohormone that undergoes peripheral conversion to the active T3 by type 1 and type 2 deiodinases. T3 supplementation (liothyronine) is not routinely recommended and is not PBS-listed in Australia.
Levothyroxine Dosing
Administration Guidance
- Take levothyroxine 30–60 minutes before breakfast, on an empty stomach, with water only.
- Separate by ≥4 hours from: calcium supplements, iron tablets, antacids (Mg/Al), sucralfate, cholestyramine, PPIs (esomeprazole, omeprazole — raise gastric pH and reduce absorption).
- Soy-based infant formula and high-fibre diets may reduce absorption.
- Consistency matters — patients who eat breakfast immediately after dosing should do so consistently; the dose can be titrated to achieve target TSH with this pattern.
- Bedtime dosing (≥3 hours after last meal) is an acceptable alternative if morning adherence is poor — some studies suggest comparable or superior absorption.
Monitoring After Initiation
- Re-check TSH at 6–8 weeks after starting or changing dose. Adjust by 12.5–25 µg increments.
- Target TSH: 0.4–4.0 mIU/L for most adults. In younger patients, aim for the lower half of the reference range (0.4–2.5 mIU/L) for optimal well-being.
- Once stable: Check TSH annually (or more frequently if symptoms change, weight alters significantly, or new interacting medications introduced).
- Overtreatment: Suppressing TSH <0.1 mIU/L in non-cancer patients increases risk of atrial fibrillation (especially elderly) and osteoporosis (especially postmenopausal women). Avoid.
- Do not use FT4 alone for monitoring — TSH is the most sensitive marker in primary hypothyroidism.
Persistent Symptoms Despite Normal TSH
A subset of patients (10–15 %) report persistent fatigue, cognitive difficulty, or weight gain despite TSH within target range. Management approach:
- Reassess adherence and administration technique.
- Investigate comorbidities: iron deficiency, vitamin D deficiency, coeliac disease, depression, sleep apnoea, chronic fatigue syndrome.
- Check FT4 and FT3 — consider whether FT3 is low-normal (some patients have impaired deiodinase conversion; combination T4/T3 therapy is not routinely recommended but may be trialled under specialist endocrinology guidance).
- Set realistic expectations — some symptoms may be unrelated to thyroid status.
- Refer to endocrinology if refractory.
Subclinical Hypothyroidism — Treatment Decision
Monitoring
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Autoimmune thyroid disease, including Hashimoto's thyroiditis, occurs in Aboriginal and Torres Strait Islander peoples, though population-level prevalence data are limited. Several barriers to diagnosis and management exist that must be addressed through culturally safe, community-centred care.
📚 References
- 1. Chaker L, Bianco AC, Jonklaas J, Peeters RP. Hypothyroidism. Lancet. 2017;390(10101):1550–1562.
- 2. Garber JR, Cobin RH, Gharib H, et al. Clinical practice guidelines for hypothyroidism in adults: cosponsored by the American Association of Clinical Endocrinologists and the American Thyroid Association. Endocr Pract. 2012;18(6):988–1028.
- 3. Pearce SH, Brabant G, Duntas LH, et al. 2013 ETA guideline: management of subclinical hypothyroidism. Eur Thyroid J. 2013;2(4):215–228.
- 4. Alexander EK, Pearce EN, Brent GA, et al. 2017 guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and the postpartum. Thyroid. 2017;27(3):315–389.
- 5. RACGP. Red Book: Guidelines for preventive activities in general practice. 9th ed. East Melbourne: RACGP; 2018.
- 6. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander health performance framework. Canberra: AIHW; 2023.
- 7. Li Y, Teng D, Shi X, et al. Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: national cross sectional study. BMJ. 2020;369:m997. [TSH population reference data]
- 8. Ross DS. Diagnosis of and screening for hypothyroidism. In: UpToDate, Cooper DS (Ed). Wolters Kluwer; 2024. Accessed June 2024.
- 9. NHMRC. National evidence-based guideline: diagnosis, management and prevention of congenital hypothyroidism. Canberra: NHMRC; 2019.
- 10. Wiersinga WM, Duntas L, Fadeyev V, Nygaard B, Vanderpump MP. 2012 ETA guidelines: the use of L-T4 + L-T3 in the treatment of hypothyroidism. Eur Thyroid J. 2012;1(2):55–71.
- 11. Pharmaceuticals Benefits Scheme (PBS). Levothyroxine sodium. Australian Government Department of Health. Available at: pbs.gov.au. Accessed June 2024.
- 12. Australian Government Department of Health. National Newborn Bloodspot Screening — Congenital Hypothyroidism. Available at: www.newbornscreening.gov.au. Accessed June 2024.