📋 Key Information Summary
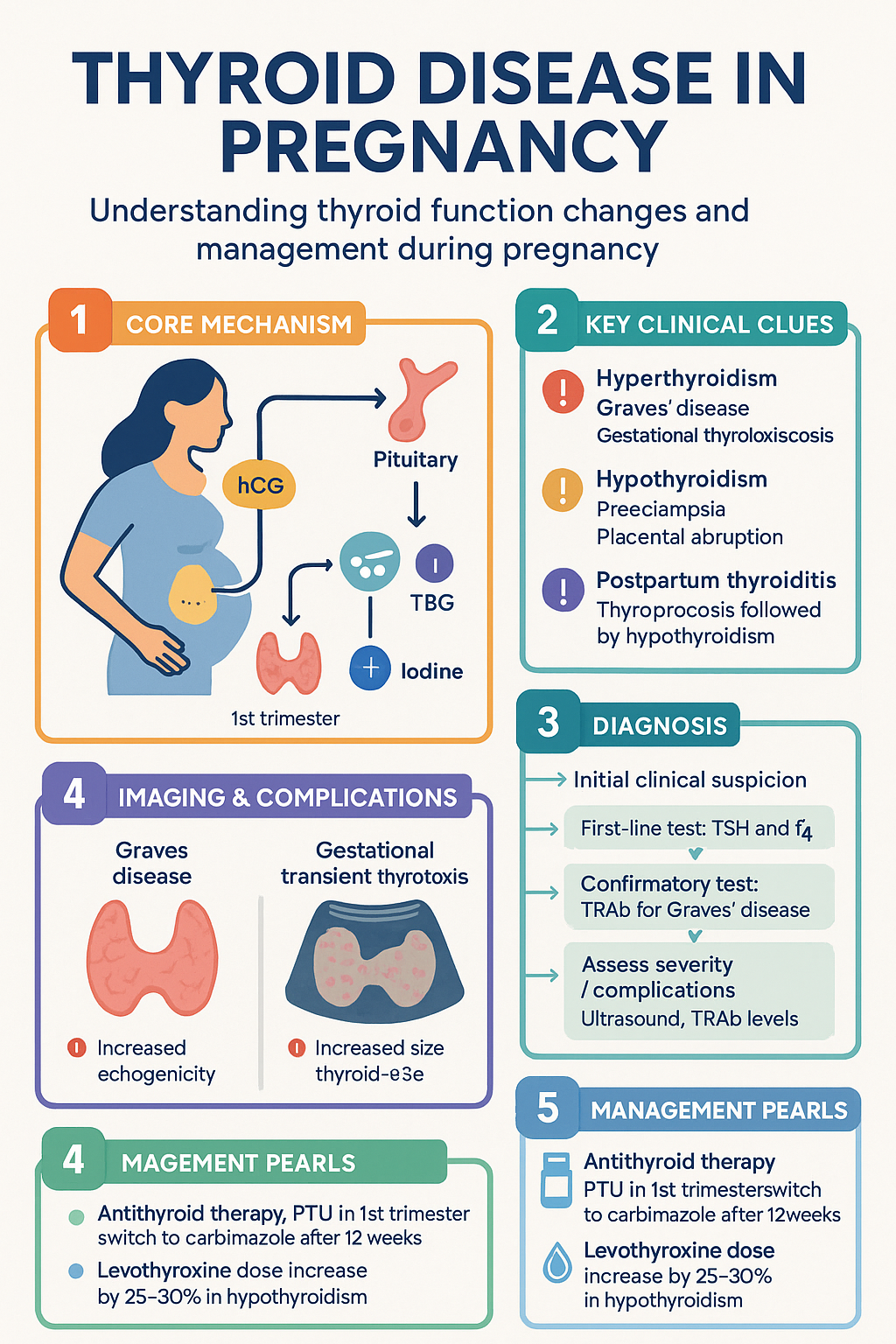
- Pregnancy causes significant physiological changes in thyroid function: hCG-driven TSH suppression in the first trimester, increased TBG, and increased iodine clearance.
- Use trimester-specific reference ranges for TSH and free T4 — ideally established from the local laboratory population (APTS 2012 data widely referenced in Australia).
- Hyperthyroidism in pregnancy is most commonly due to Graves' disease; transient hCG-mediated hyperthyroidism (gestational thyrotoxicosis) requires no antithyroid therapy.
- Propylthiouracil (PTU) is the preferred antithyroid drug in the first trimester due to methimazole-associated embryopathy risk; switch to carbimazole after 12 weeks if needed.
- Untreated maternal hypothyroidism is associated with pre-eclampsia, placental abruption, preterm birth, and impaired neurocognitive development in the offspring.
- Levothyroxine dose requirements increase by approximately 30–50% in pregnancy; empirically increase dose by 25–30% as soon as pregnancy is confirmed in women with known hypothyroidism.
- Postpartum thyroiditis occurs in 5–10% of women, typically presenting with thyrotoxicosis at 1–6 months postpartum, followed by hypothyroidism at 4–8 months.
- Radioactive iodine (I-131) is absolutely contraindicated in pregnancy and in women who may become pregnant.
- TSH receptor antibodies (TRAb) should be measured in the third trimester in Graves' disease to assess neonatal thyrotoxicosis risk.
- Australia recommends a minimum iodine intake of 220 µg/day in pregnancy and 270 µg/day during lactation; iodine supplementation (150 µg/day) is advised for all pregnant and breastfeeding women.
- Aboriginal and Torres Strait Islander women have higher rates of thyroid disease and may face barriers to timely screening and specialist follow-up in remote settings.
🎧 Audio Brief
Introduction & Australian Epidemiology
Thyroid disease in pregnancy requires careful management due to altered thyroid physiology, teratogenic risks of antithyroid drugs, and the profound impact of maternal thyroid hormones on foetal neurodevelopment. Thyroid dysfunction is one of the most common endocrine disorders encountered during pregnancy, with overt hypothyroidism affecting 0.3–0.5% and overt hyperthyroidism affecting 0.1–0.4% of pregnancies. Subclinical thyroid disease is far more prevalent, with subclinical hypothyroidism present in 2–5% and isolated hypothyroxinaemia in approximately 1–2% of pregnant women.
In Australia, thyroid autoimmunity (positive thyroid peroxidase antibodies) is found in approximately 10–15% of pregnant women, making it the most common autoimmune condition in pregnancy. The Australian Thyroid Study and data from the Australian Preterm Thyroid (APTS) trial have informed local trimester-specific reference ranges. Iodine deficiency remains a concern in parts of Australia despite mandatory fortification of bread with iodised salt since 2009.
This guideline covers the physiological adaptations of the thyroid axis during pregnancy, the diagnosis and management of hyperthyroidism (predominantly Graves' disease), hypothyroidism, and postpartum thyroiditis, with reference to Australian PBS-listed therapies, MBS item numbers, and national health priorities.
Physiological Changes in Pregnancy
Pregnancy induces substantial alterations in thyroid physiology that must be understood to avoid misdiagnosis and inappropriate treatment.
hCG-Mediated TSH Suppression
Human chorionic gonadotropin (hCG) shares structural homology with TSH and exerts a weak thyroid-stimulating effect. Rising hCG levels in the first trimester cause a nadir in TSH between weeks 8–12 of gestation. TSH levels below the non-pregnant lower limit (typically <0.1 mIU/L) may be normal in the first trimester. The upper limit of normal for TSH in the first trimester is approximately 2.5 mIU/L in most Australian reference datasets, though local laboratory ranges should be used.
Increased Thyroid-Binding Globulin (TBG)
Oestrogen-driven hepatic synthesis of TBG increases from the first trimester, reaching a plateau in the second trimester at approximately twice the non-pregnant level. Total T4 and total T3 rise proportionally, but free T4 and free T3 remain relatively stable (or mildly decrease) in a euthyroid pregnancy. Measurement of total T4 without interpretation using trimester-specific ranges is not recommended.
Iodine Homeostasis
Increased renal iodide clearance during pregnancy (estimated glomerular filtration rate increases by 40–50%) and placental transfer of iodine to the foetus elevate iodine requirements. The WHO, NHMRC, and Australian National Iodine Nutrition Survey recommend a minimum intake of 220 µg/day during pregnancy and 270 µg/day during lactation. Women in areas of marginal iodine deficiency should receive iodine supplementation of 150 µg/day, as is the routine recommendation of the Endocrine Society of Australia and the Australasian Society of Thyroidologists (AST).
Trimester-Specific Reference Ranges (Australian Data)
| Parameter | First Trimester | Second Trimester | Third Trimester |
|---|---|---|---|
| TSH (mIU/L) | 0.03 – 2.5 | 0.13 – 3.0 | 0.3 – 3.5 |
| Free T4 (pmol/L) | 11 – 19 | 10 – 17 | 9 – 16 |
| Free T3 (pmol/L) | 3.2 – 5.5 | 3.0 – 5.0 | 2.8 – 4.5 |
Note: Ranges are indicative and derived from APTS and published Australian cohorts. Individual laboratories should apply population-specific reference intervals. MBS item 66720 (thyroid function tests) is generally available through Medicare.
Hyperthyroidism in Pregnancy (Graves' Disease)
Diagnosis
Overt hyperthyroidism complicates approximately 0.2% of pregnancies. Graves' disease is the most common cause (85–90%), with toxic multinodular goitre and toxic adenoma accounting for most of the remainder. Gestational transient thyrotoxicosis (GTT), occurring in 1–3% of pregnancies, is caused by high hCG levels (especially with hyperemesis gravidarum or multiple pregnancy) and is a distinct entity requiring no antithyroid treatment.
Distinguishing Graves' Disease from Gestational Transient Thyrotoxicosis
| Feature | Graves' Disease | Gestational Transient Thyrotoxicosis |
|---|---|---|
| Onset | Any trimester; may predate pregnancy | First trimester (weeks 6–12) |
| TSH receptor antibodies (TRAb) | Positive | Negative |
| Goitre | Diffuse goitre ± bruit | No goitre or small, non-tender |
| Ophthalmopathy | Present in ~25% | Absent |
| Thyroid ultrasound | Diffuse hypoechogenicity, increased vascularity | Normal or mildly heterogeneous |
| Time course | Persistent without treatment | Resolves by mid-pregnancy |
| Treatment | Antithyroid drugs | Supportive care; no antithyroid drugs |
Antithyroid Drug Therapy
The choice and timing of antithyroid drugs (thionamides) in pregnancy is guided by teratogenic risk data and the severity of thyrotoxicosis.
Management of Graves' Disease — Trimester-by-Trimester
Beta-Blocker Use
Propranolol may be used short-term for symptomatic control of adrenergic symptoms (tachycardia, tremor, anxiety) in thyrotoxicosis. Dose: 10–40 mg PO TDS–QDS. Avoid prolonged use in pregnancy due to risk of intrauterine growth restriction, bradycardia, and neonatal hypoglycaemia. Atenolol is specifically avoided in pregnancy (associated with IUGR).
Thyroid Storm in Pregnancy
Hypothyroidism in Pregnancy
Prevalence & Aetiology
Overt hypothyroidism affects 0.3–0.5% of pregnancies, and subclinical hypothyroidism (SCH) affects 2–5%. Autoimmune thyroiditis (Hashimoto's disease) is the most common aetiology. Other causes include prior radioiodine therapy, thyroidectomy, iodine deficiency, and medications (amiodarone, lithium, immune checkpoint inhibitors).
Impact of Untreated Hypothyroidism
Maternal hypothyroidism is associated with significant adverse outcomes, and treatment substantially reduces these risks:
- Pre-eclampsia (OR 1.7–2.5)
- Placental abruption
- Preterm birth (<37 weeks)
- Low birth weight
- Postpartum haemorrhage
- Impaired neurocognitive development in offspring (IQ reduction of 3–7 points in some studies)
- Gestational diabetes (in some cohorts)
Management of Overt Hypothyroidism
Subclinical Hypothyroidism (SCH) in Pregnancy
SCH is defined as elevated TSH (above trimester-specific upper limit) with normal free T4. Management is guided by TPO antibody status and TSH level:
- TSH >10 mIU/L: Treat with levothyroxine regardless of antibody status.
- TSH 2.5–10 mIU/L + TPO antibody positive: Treat with levothyroxine (ATA 2017 strong recommendation).
- TSH 2.5–10 mIU/L + TPO antibody negative: Consider treatment, especially if TSH >5 mIU/L or other risk factors (prior preterm birth, BMI >40). Monitor with TSH every 4 weeks.
Isolated Hypothyroxinaemia
Defined as normal TSH with free T4 below the 2.5th percentile for gestational age. Current Australian practice is to observe and recheck in 4 weeks, as the clinical significance remains debated and routine treatment is not recommended by ATA 2017 or Endocrine Society guidelines.
Postpartum Thyroiditis
Epidemiology & Pathogenesis
Postpartum thyroiditis (PPT) affects 5–10% of all women in the first year after delivery. It is an autoimmune-mediated destructive thyroiditis resulting from rebound immune activity following the immunosuppression of pregnancy. Risk factors include positive TPO antibodies (risk increases 3–4 fold), type 1 diabetes mellitus, prior PPT, other autoimmune conditions, and history of postpartum depression.
Clinical Phases
Management
| Phase | Management | Notes |
|---|---|---|
| Thyrotoxic (destructive) | Symptomatic treatment only: propranolol 10–20 mg PO TDS–QDS as needed. NO antithyroid drugs (this is destructive, not overproduction). | Reassure; explain self-limiting nature. Monitor FT4/TSH at 4–6 week intervals. |
| Hypothyroid | Levothyroxine 50–100 µg PO daily. Trial withdrawal after 6–12 months if TSH normalises. | If breastfeeding, levothyroxine is safe and recommended. If planning another pregnancy, recheck TSH pre-conception. |
| Recovery | Annual TSH monitoring for life (20–30% risk of permanent hypothyroidism). | Educate regarding symptoms of hypothyroidism; advise TSH check before next pregnancy. |
Postpartum Depression & Thyroiditis
Women presenting with postpartum depression should have TSH and FT4 measured as part of the workup, as hypothyroid PPT can present with predominantly psychiatric symptoms. Treatment of the hypothyroid phase may improve depressive symptoms, though the relationship is complex and not all postpartum depression is thyroid-mediated.
Investigations
The following investigations are relevant to thyroid disease in pregnancy. Availability and Medicare rebate status are noted.
Screening Recommendations
Universal thyroid screening in pregnancy is debated. Current Australian practice, aligned with the ATA 2017 guidelines, does not recommend universal screening but supports a targeted case-finding approach.
Indications for TSH Screening in Pregnancy
- Age >30 years
- Residence in an area of known moderate-to-severe iodine deficiency
- History of thyroid disease, thyroid surgery, or head/neck irradiation
- Family history of thyroid disease (first-degree relative)
- Known positive thyroid antibodies (TPOAb or TRAb)
- Symptoms or signs of thyroid dysfunction
- Type 1 diabetes mellitus or other autoimmune condition
- History of infertility, recurrent miscarriage, or preterm delivery
- Morbid obesity (BMI ≥40 kg/m²)
- Prior therapeutic head or neck irradiation
- Use of amiodarone, lithium, or recent iodinated contrast
Timing
Ideally screen before conception or at the first antenatal visit (typically 6–10 weeks). If initial TSH is normal and risk factors persist, recheck at 16–20 weeks and again in the third trimester if new symptoms develop.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Postpartum Management & Breastfeeding
Levothyroxine in Breastfeeding
Levothyroxine is safe during breastfeeding. Only trace amounts appear in breast milk. Continue at pre-pregnancy dose; recheck TSH at 6 weeks postpartum. No dose adjustment is required for breastfeeding.
Antithyroid Drugs in Breastfeeding
Both PTU and carbimazole are excreted in breast milk in small amounts. Current guidelines (ATA 2017, Endocrine Society) recommend:
- Carbimazole/methimazole: Preferred during breastfeeding at doses ≤20 mg/day. Considered safe; the relative infant dose is low (~1–2% of maternal dose).
- PTU: Less preferred during breastfeeding due to potential hepatotoxicity risk, but acceptable at doses ≤300 mg/day if carbimazole is not tolerated.
- Administer antithyroid drugs in divided doses after feeds to minimise infant exposure.
- Monitor infant thyroid function if maternal doses are high.
Screening for Postpartum Thyroiditis
Offer TSH at 3 months and 6 months postpartum to all women with TPO antibody positivity or history of prior PPT. Educate women about symptoms of both thyrotoxicosis and hypothyroidism in the postpartum period.
Quick Reference — Antithyroid Drug Selection in Pregnancy
📚 References
- 1. Alexander EK, Pearce EN, Brent GA, et al. 2017 Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and the Postpartum. Thyroid. 2017;27(3):315–389.
- 2. De Groot L, Abalovich M, Alexander EK, et al. Management of thyroid dysfunction during pregnancy and postpartum: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2012;97(8):2543–2565.
- 3. Andersen SL, Olsen J, Wu CS, Laurberg P. Severity of birth defects after propylthiouracil (PTU) exposure in early pregnancy: a cohort study. Lancet Diabetes Endocrinol. 2014;2(9):713–719.
- 4. Lazarus JH, Bestwick JP, Channon S, et al. Antenatal thyroid screening and childhood cognitive function (CATS trial). N Engl J Med. 2012;366(6):493–501.
- 5. National Health and Medical Research Council (NHMRC). Iodine supplementation for pregnant and breastfeeding women. NHMRC Public Statement. Canberra: NHMRC; 2010.
- 6. Li M, Eastman CJ, Waite KV, et al. Are Australian children iodine deficient? Results of the Australian National Iodine Nutrition Study. Med J Aust. 2006;184(4):165–169.
- 7. Stagnaro-Green A, Abalovich M, Alexander E, et al. Guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and postpartum. Thyroid. 2011;21(10):1081–1125.
- 8. Cooper DS, Laurberg P. Hyperthyroidism in pregnancy. Lancet Diabetes Endocrinol. 2013;1(3):238–249.
- 9. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander health performance framework 2020 summary report. Canberra: AIHW; 2020.
- 10. Korevaar TIM, Muetzel R, Medici M, et al. Association of maternal thyroid function during early pregnancy with offspring IQ and brain morphology in childhood: a population-based prospective cohort study. Lancet Diabetes Endocrinol. 2016;4(1):35–43.
- 11. Negro R, Schwartz A, Gismondi R, et al. Universal screening versus case finding for detection and treatment of thyroid hormonal dysfunction during pregnancy. J Clin Endocrinol Metab. 2010;95(4):1699–1707.
- 12. Services for Australian Rural and Remote Allied Health (SARRAH). Telehealth in rural and remote Australia. SARRAH Position Paper. 2021.
- 13. NHMRC, Australian Government Department of Health. The Australian Immunisation Handbook — Chapter 3: Vaccination for Aboriginal and Torres Strait Islander people. 11th ed (online). Canberra; 2022.