📋 Key Information Summary
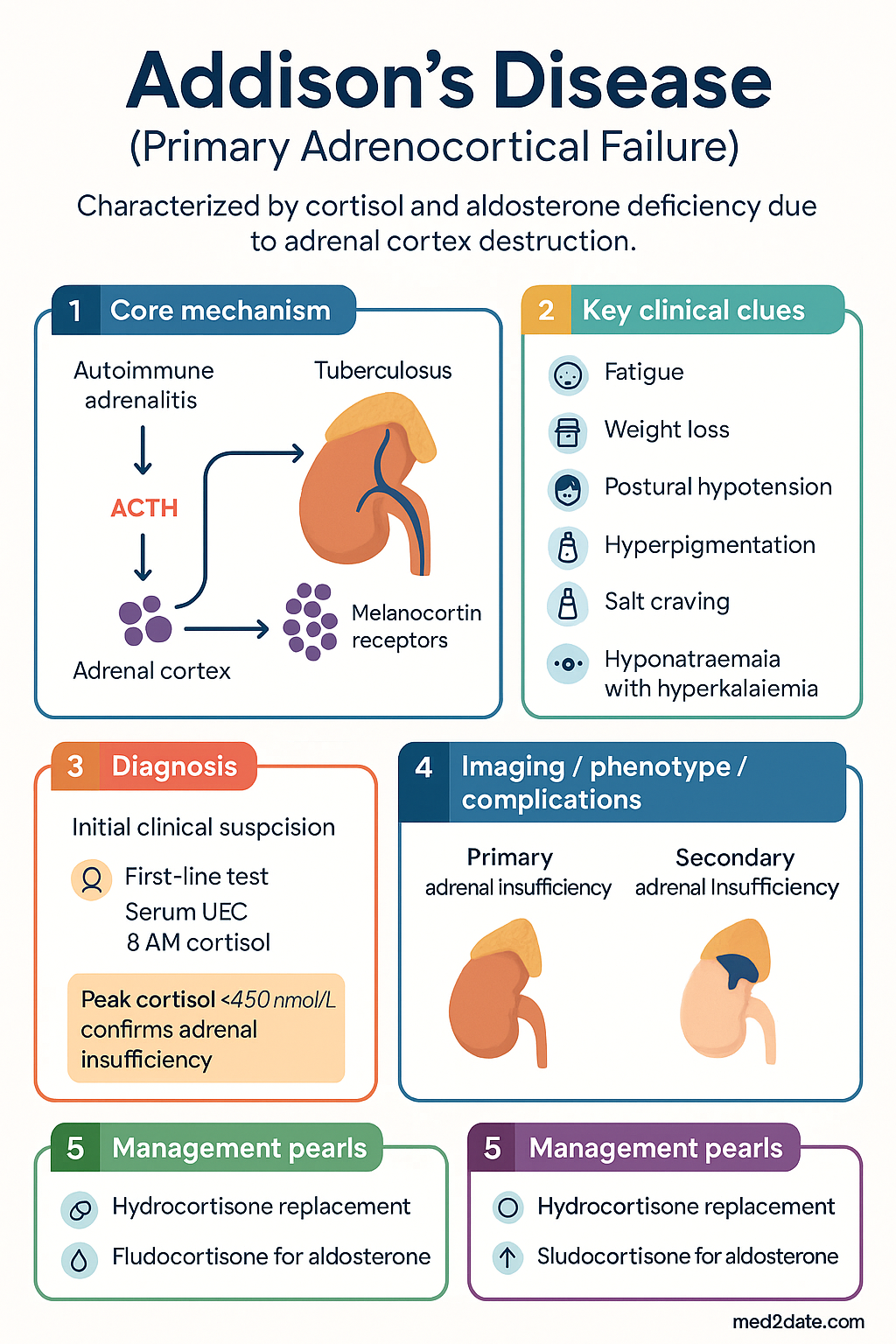
- Addison's disease is primary adrenocortical insufficiency characterised by cortisol and aldosterone deficiency due to destruction of the adrenal cortex.
- Autoimmune adrenalitis accounts for ~85% of cases in Australia; tuberculosis remains important in immigrant and ATSI populations.
- Prevalence in Australia is approximately 45–60 per million; incidence ~5 per million per year, with a female-to-male ratio of 2–3:1.
- Classic presentation includes fatigue, weight loss, postural hypotension, hyperpigmentation (due to ACTH excess), salt craving, and hyponatraemia with hyperkalaemia.
- Adrenal crisis is a medical emergency — presenting with hypotensive shock, altered consciousness, fever, and abdominal pain — with mortality up to 6% per episode.
- Short Synacthen Test (SST) is the gold-standard diagnostic test in Australia; a peak cortisol <450 nmol/L at 30–60 min confirms adrenal insufficiency (MBS Item 66682).
- Hydrocortisone is the preferred glucocorticoid replacement (15–25 mg/day divided into 2–3 doses); fludrocortisone replaces aldosterone (50–200 µg once daily).
- Sick day rules require patients to double or triple oral hydrocortisone during intercurrent illness; if unable to tolerate oral intake, emergency IM hydrocortisone 100 mg must be administered immediately.
- All patients should carry a Steroid Card, an emergency hydrocortisone kit (100 mg IM ampoule + syringe), and an Adrenal Crisis Letter.
- Screen for associated autoimmune conditions (thyroid disease, type 1 diabetes, premature ovarian insufficiency, coeliac disease, vitiligo) at diagnosis and periodically.
- Emergency department management of adrenal crisis: IV 0.9% sodium chloride bolus 1 L (adult), hydrocortisone 100 mg IV/IM stat, then 50 mg IV/IM 6-hourly until haemodynamically stable.
- Patients require lifelong monitoring with annual review of replacement adequacy, bone density, autoimmune screen, and adrenal crisis prevention education.
🎧 Audio Brief
Introduction & Australian Epidemiology
Addison's disease, or primary adrenocortical insufficiency, arises from progressive destruction of the adrenal cortex, resulting in deficient production of cortisol, aldosterone, and adrenal androgens. The condition must be distinguished from secondary (pituitary) and tertiary (hypothalamic) causes, which present with cortisol deficiency alone due to insufficient ACTH stimulation.
In Australia, the estimated prevalence is 45–60 cases per million population, with an incidence of approximately 5 per million per year. Autoimmune adrenalitis is the predominant aetiology in Australian tertiary referral centres, accounting for roughly 85% of diagnosed cases. The peak age of onset is between 30 and 50 years, with a marked female predominance (F:M ratio 2–3:1) reflecting the autoimmune basis of the disease.
The insidious onset and non-specific early symptoms mean that diagnosis is frequently delayed by months to years. Studies suggest that up to 50% of adrenal cortex may be destroyed before clinical insufficiency becomes apparent. Once identified, however, the condition is readily treatable with lifelong hormone replacement. The principal ongoing risk is adrenal crisis, which remains a significant cause of morbidity and potentially preventable death.
Given the association with other autoimmune disorders, patients with Addison's disease require screening for polyglandular autoimmune syndromes — particularly autoimmune thyroid disease (present in ~50% of cases), type 1 diabetes mellitus (~10–15%), premature ovarian insufficiency (~10%), coeliac disease (~5–8%), and vitiligo (~10–15%). In the Australian setting, healthcare providers should also consider infectious aetiologies such as tuberculosis, which remains relevant in Aboriginal and Torres Strait Islander communities and in patients from high-burden countries.
Pathophysiology & Causes
Normal Adrenal Function
The adrenal cortex comprises three functional zones: the zona glomerulosa (mineralocorticoid — aldosterone), the zona fasciculata (glucocorticoid — cortisol), and the zona reticularis (androgens — DHEA, androstenedione). Cortisol secretion is regulated by the hypothalamic–pituitary–adrenal (HPA) axis via ACTH, which also drives adrenal melanocortin receptors, explaining the characteristic hyperpigmentation of primary insufficiency.
Aldosterone secretion is primarily controlled by the renin–angiotensin–aldosterone system (RAAS) and serum potassium. Its loss in Addison's disease leads to sodium wasting, potassium retention, and the metabolic derangements that distinguish primary from secondary adrenal insufficiency.
Aetiologies
| Aetiology | Frequency (Australia) | Key Features |
|---|---|---|
| Autoimmune adrenalitis | ~85% | 21-hydroxylase antibodies positive; associated with APS-1 & APS-2; lymphocytic infiltration on histology |
| Tuberculosis | ~5–10% | Important in ATSI populations, immigrants from high-burden countries; calcified adrenals on CT |
| Adrenal haemorrhage / infarction | ~2–3% | Waterhouse–Friderichsen syndrome (meningococcal); anticoagulant therapy; antiphospholipid syndrome |
| Metastatic infiltration | ~1–2% | Lung, breast, melanoma; usually bilateral and >90% destruction required |
| Infectious | Rare | HIV/CMV (in advanced immunosuppression), histoplasmosis, cryptococcosis |
| Congenital adrenal hyperplasia | Rare | 21-hydroxylase deficiency most common; usually diagnosed neonatally or in childhood |
| Adrenoleucodystrophy | Rare | X-linked; very long-chain fatty acid accumulation; consider in young males |
| Other (drugs, sarcoidosis, amyloidosis) | Rare | Ketoconazole, etomidate, mitotane; granulomatous disease |
Autoimmune Mechanisms
Autoimmune destruction involves CD4+ and CD8+ T-cell mediated cytotoxicity against adrenocortical cells. Circulating antibodies to 21-hydroxylase (CYP21A2) are detectable in ~85% of autoimmune cases and serve as a useful serological marker. Addison's disease may occur in isolation or as part of autoimmune polyendocrine syndromes:
- APS-1 (APECED): Autosomal recessive; AIRE gene mutation; triad of chronic mucocutaneous candidiasis, hypoparathyroidism, and Addison's disease. Onset usually in childhood.
- APS-2 (Schmidt syndrome): Polygenic; Addison's disease + autoimmune thyroid disease ± type 1 diabetes; adult onset; HLA-DR3/DR4 associated.
Clinical Features & Adrenal Crisis
Gradual Onset — Chronic Insufficiency
The presentation is often insidious over weeks to months, with progressive non-specific symptoms that may be attributed to other diagnoses:
| System | Symptoms / Signs | Mechanism |
|---|---|---|
| General | Fatigue, malaise, weakness, weight loss, anorexia | Cortisol deficiency; reduced gluconeogenesis |
| Pigmentation | Generalised hyperpigmentation — creases, buccal mucosa, scars, areolae | ACTH and MSH excess stimulating melanocortin-1 receptors |
| Cardiovascular | Postural hypotension, dizziness, syncope | Cortisol + aldosterone deficiency → volume depletion, reduced vascular tone |
| Gastrointestinal | Nausea, vomiting, abdominal pain, salt craving, diarrhoea | Electrolyte disturbance; cortisol deficiency GI effects |
| Metabolic | Hyponatraemia, hyperkalaemia, hypoglycaemia (especially in children) | Aldosterone loss → Na⁺ wasting, K⁺ retention; cortisol loss → impaired gluconeogenesis |
| Musculoskeletal | Myalgia, arthralgia | Electrolyte disturbance; androgen deficiency |
| Psychiatric | Depression, irritability, difficulty concentrating, reduced libido | Cortisol and androgen deficiency |
Adrenal Crisis
Adrenal (Addisonian) crisis is a life-threatening endocrine emergency characterised by acute haemodynamic compromise due to cortisol deficiency. It may be the presenting feature of undiagnosed Addison's disease or occur in patients on replacement therapy who are inadequately dosed during intercurrent illness.
Precipitants of Adrenal Crisis
- Intercurrent infection or febrile illness (most common — ~40–50% of crises)
- Gastroenteritis with vomiting/diarrhoea leading to failure to absorb oral hydrocortisone
- Surgery, trauma, or other physiological stress without glucocorticoid stress dosing
- Withholding or forgetting replacement therapy
- Pregnancy and labour without adequate dose adjustment
- Starting medications that accelerate cortisol metabolism (e.g., rifampicin, phenytoin, carbamazepine, mitotane)
1. IV access — draw blood for glucose, UEC, cortisol, blood cultures if febrile.
2. Hydrocortisone 100 mg IV bolus (or IM if no IV access). Do NOT wait for cortisol results.
3. IV 0.9% sodium chloride 1 L over 30–60 min (adult). Repeat as needed. Children: 20 mL/kg bolus.
4. Dextrose 10% if hypoglycaemic.
5. Continue hydrocortisone 50 mg IV/IM 6-hourly until haemodynamically stable and tolerating oral intake.
6. Identify and treat the precipitant (antibiotics for infection, etc.).
7. Involve endocrinology early.
Investigations
Initial Screening (Biochemistry)
Short Synacthen Test (SST) — Gold Standard
The SST is the primary confirmatory test in Australia and is available through pathology services (MBS Item 66682 — Synacthen stimulation test).
1. Administer IV or IM tetracosactide (Synacthen®) 250 µg.
2. Measure serum cortisol at 0, 30, and 60 minutes.
3. A peak cortisol ≥450 nmol/L (using immunoassay) at 30 or 60 min indicates an adequate adrenal response and excludes adrenal insufficiency.
4. Cortisol below this threshold is diagnostic of adrenal insufficiency.
Notes: The 1 µg (low-dose) SST may be more sensitive for early or partial insufficiency but is not standardised in Australian laboratories. Perform the test at any time of day in suspected crisis; in stable outpatients, an 8 AM baseline cortisol should be drawn first.
Aetiological Investigations
Associated Autoimmune Screen (at Diagnosis)
| Condition | Screening Test | Frequency |
|---|---|---|
| Autoimmune thyroid disease | TSH, free T4, TPO antibodies | At diagnosis, then annually |
| Type 1 diabetes | Fasting glucose, HbA1c, GAD antibodies | At diagnosis, then annually (fasting glucose/HbA1c) |
| Coeliac disease | IgA tissue transglutaminase (tTG-IgA) + total IgA | At diagnosis; repeat if new GI symptoms develop |
| Premature ovarian insufficiency | FSH, oestradiol (if menstruating and <40 years) | At diagnosis; if menstrual irregularity develops |
| Vitiligo | Clinical inspection | At each review |
Management & Sick Day Rules
Long-Term Replacement Therapy
Dosing Principles
- Physiological replacement — aim for the lowest dose that controls symptoms. Over-replacement increases osteoporosis, cardiovascular, and metabolic risk.
- Mimic circadian rhythm — two-thirds of the daily hydrocortisone dose in the morning, one-third in the early afternoon. Avoid late-evening dosing (insomnia).
- Modified-release hydrocortisone (Plenadren®) — once-daily formulation providing more physiological cortisol profile; superior quality of life in some studies. Not PBS-listed in Australia; limited availability.
- Fludrocortisone is not required in secondary adrenal insufficiency (the RAAS is intact as it does not depend on ACTH).
Sick Day Rules
Emergency Kit & Patient Education
| Item | Details |
|---|---|
| Hydrocortisone ampoule | Hydrocortisone sodium succinate 100 mg powder for injection (Solu-Cortef® or generic). PBS General Benefit. |
| Syringe + drawing-up needle | 5 mL syringe + 21G needle for reconstitution. |
| IM needle | 23G × 25 mm (or 25G × 16 mm for paediatric) for intramuscular injection into the anterolateral thigh. |
| Steroid emergency card | Card detailing diagnosis, usual medications, and emergency dose. Must be carried at all times. |
| Adrenal crisis letter | Letter from endocrinologist for ED staff with management instructions — laminated, kept with kit. |
Monitoring
| Parameter | Frequency | Purpose |
|---|---|---|
| Clinical symptoms (fatigue, weight, BP, pigmentation) | Every 3–6 months (first year), then annually | Assess replacement adequacy — under- vs over-replacement |
| Blood pressure (supine + standing) | Every visit | Postural drop suggests under-replacement of fludrocortisone or hydrocortisone |
| Serum electrolytes (Na⁺, K⁺) | Every 3–6 months, then annually | Hyponatraemia or hyperkalaemia suggests fludrocortisone under-replacement |
| Plasma renin activity (if available) | Annually or when adjusting fludrocortisone | Most objective marker of mineralocorticoid replacement adequacy |
| Weight, BMI | Every visit | Weight gain may indicate over-replacement |
| Bone mineral density (DEXA scan) | At diagnosis; then every 2–5 years | Glucocorticoid over-replacement increases fracture risk |
| Autoimmune screen (TSH, HbA1c) | Annually | Screen for associated autoimmune conditions |
| Sick day rules / emergency kit review | Every visit | Reinforce education; check kit expiry dates; update adrenal crisis letter |
Biomarkers of Replacement Adequacy
No single biochemical test perfectly reflects physiological cortisol replacement. In clinical practice, a combination of symptom assessment, body weight trajectory, electrolytes, and ACTH levels is used. Serum cortisol day curves may be helpful in selected patients (e.g., those with persistent symptoms despite apparently adequate dosing).
- Over-replacement signs: Weight gain, Cushingoid features (moon face, central adiposity, striae), osteoporosis, hyperglycaemia, hypertension.
- Under-replacement signs: Persistent fatigue, weight loss, postural hypotension, hyperpigmentation, hyponatraemia, elevated ACTH.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Bornstein SR, Allolio B, Arlt W, et al. Diagnosis and treatment of primary adrenal insufficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2016;101(2):364–389.
- 2. Husebye ES, Pearce SH, Krone NP, Kämpe O. Adrenal insufficiency. Lancet. 2021;397(10274):613–629.
- 3. Rushworth RL, Torpy DJ, Falhammar H. Adrenal crisis. N Engl J Med. 2019;381(9):852–861.
- 4. Australian Institute of Health and Welfare (AIHW). Admitted patient care 2021–22: adrenal insufficiency hospitalisations. Canberra: AIHW; 2023.
- 5. Bettering the Evaluation and Care of Health (BEACH). Prevalence of adrenal insufficiency in Australian general practice. Aust Fam Physician. 2019;48(10):734–738.
- 6. Bancos I, Hahner S, O'Sullivan J, Arlt W. Diagnosis and management of adrenal insufficiency. Lancet Diabetes Endocrinol. 2015;3(3):216–226.
- 7. Chakera AJ, Vaidya B. Addison disease in adults: diagnosis and management. Am J Med. 2010;123(5):409–413.
- 8. Gurnell EM, Hunt PJ, Curran SE, et al. Long-term DHEA replacement in primary adrenal insufficiency: a randomized, controlled trial. J Clin Endocrinol Metab. 2008;93(2):400–409.
- 9. RHDAustralia (formerly TSANZ). The Australian tuberculosis control guidelines. 4th ed. Darwin: RHDAustralia; 2021.
- 10. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.
- 11. Quinkler M, Ekman B, Zhang P, Ismail MB. Mortality data from the European Adrenal Insufficiency Registry (EU-AIR). Eur J Endocrinol. 2018;179(2):113–120.
- 12. Hahner S, Spinnler C, Reisch N, et al. Association between chronic and acute complications in adrenal insufficiency — a survey of 853 patients. Eur J Endocrinol. 2015;172(5):597–604.