📋 Key Information Summary
- The hypothalamic–pituitary axis (HPA) governs growth, reproduction, metabolism, stress response, water balance and circadian rhythm via a hierarchical three-tier endocrine system.
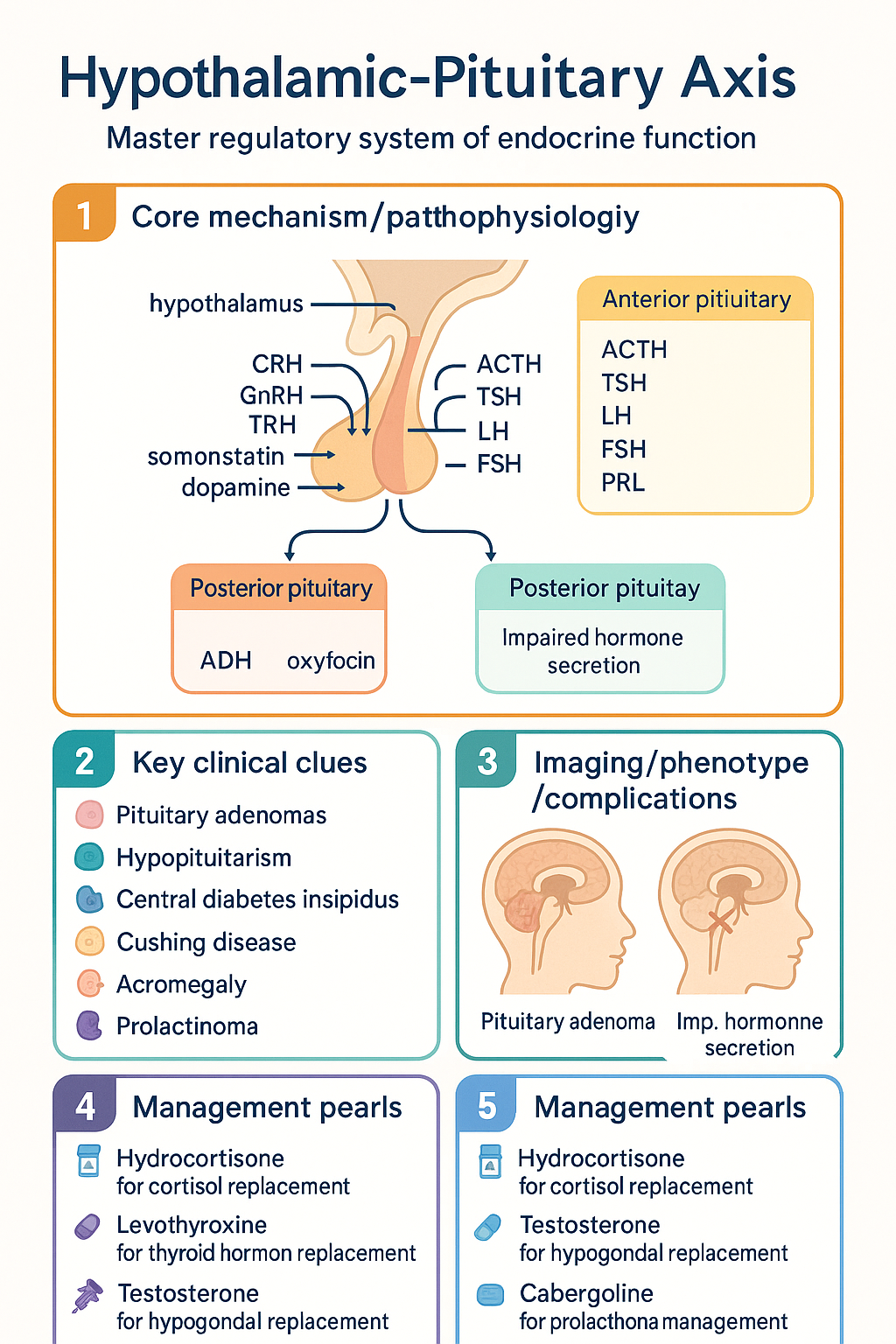
- The hypothalamus secretes releasing/inhibiting hormones (CRH, GnRH, TRH, GHRH, somatostatin, dopamine) that regulate anterior pituitary trophic hormones.
- Six anterior pituitary hormones — ACTH, TSH, LH, FSH, GH, PRL — each act on peripheral target glands with negative feedback maintaining homeostasis.
- Posterior pituitary releases ADH (vasopressin) and oxytocin, synthesised in the hypothalamus and stored in the posterior lobe.
- Negative feedback from cortisol, thyroid hormones, oestradiol/testosterone, and IGF-1 at both hypothalamic and pituitary levels is the primary regulatory mechanism.
- Dynamic stimulation testing (insulin tolerance test, glucagon stimulation test, ACTH stimulation test) is the gold standard for assessing HPA reserve in suspected hypopituitarism.
- The insulin tolerance test (ITT) remains the gold standard for GH and cortisol reserve assessment in Australia but requires cardiac monitoring and experienced endocrine supervision.
- TRH and GnRH stimulation tests assess TSH and gonadotrophin reserve respectively; the short Synacthen test is the most practical screening test for adrenal reserve.
- Pituitary adenomas (both functioning and non-functioning) account for the majority of HPA pathology encountered in Australian endocrine practice.
- Hypopituitarism may present insidiously; panhypopituitarism is life-threatening if adrenal insufficiency is not recognised and treated before other hormone replacement.
- Cushing disease (ACTH-secreting pituitary adenoma) and acromegaly (GH-secreting adenoma) require specialist management at tertiary centres with multidisciplinary pituitary teams.
- Aboriginal and Torres Strait Islander peoples have higher rates of diabetes and metabolic syndrome, which may complicate HPA-related endocrine assessment; culturally safe care and awareness of remote access barriers are essential.
🎧 Audio Brief
Introduction & Australian Epidemiology
The hypothalamic–pituitary axis (HPA) is the master regulatory system of endocrine function. It operates through a three-tiered hierarchical model: the hypothalamus produces releasing and inhibiting hormones, the anterior pituitary secretes trophic hormones, and peripheral target glands produce end-effectors that feed back to modulate upstream secretion. This elegant feedback architecture governs growth, reproduction, thyroid function, adrenal stress responses, water balance, lactation and circadian rhythm.
In Australian clinical practice, disorders of the HPA encompass pituitary adenomas (both functioning and non-functioning), hypopituitarism from any cause (surgery, radiation, infiltrative disease, traumatic brain injury, Sheehan syndrome), central diabetes insipidus, and syndromes of inappropriate hormone excess such as Cushing disease, acromegaly and prolactinoma.
Pituitary adenomas are found incidentally in approximately 10–15% of the general population on high-resolution MRI, though clinically significant tumours are far less common. Non-functioning pituitary adenomas are the most frequently encountered subtype in Australian endocrine clinics. Prolactinomas are the most common functioning adenoma, with an estimated prevalence of 50–60 per 100,000 in women and 10–15 per 100,000 in men. Acromegaly has an estimated prevalence of 40–60 per million in Australia, with a diagnostic delay of 7–10 years being common. Cushing disease incidence is approximately 1–2 per million per year.
Traumatic brain injury (TBI) is an increasingly recognised cause of hypopituitarism, with studies from Australian trauma centres reporting anterior pituitary deficiency in 25–50% of moderate-to-severe TBI survivors. Awareness of this association is critical for long-term follow-up.
Anatomy & Hormones of the HPA
Hypothalamic Releasing & Inhibiting Hormones
The hypothalamus lies in the diencephalon, inferior to the third ventricle and superior to the pituitary stalk (infundibulum). Neurosecretory neurons synthesise releasing and inhibiting peptides that travel via the hypophyseal portal system to the anterior pituitary.
| Hypothalamic Hormone | Abbreviation | Action on Anterior Pituitary |
|---|---|---|
| Corticotrophin-releasing hormone | CRH | Stimulates ACTH release from corticotrophs |
| Thyrotrophin-releasing hormone | TRH | Stimulates TSH (and PRL) release from thyrotrophs/lactotrophs |
| Gonadotrophin-releasing hormone | GnRH | Stimulates LH and FSH release from gonadotrophs (pulsatile secretion required) |
| Growth hormone–releasing hormone | GHRH | Stimulates GH release from somatotrophs |
| Somatostatin (SRIF) | SS | Inhibits GH and TSH release |
| Dopamine | DA | Inhibits PRL release from lactotrophs (tonic inhibition) |
Anterior Pituitary Hormones
The anterior pituitary (adenohypophysis) contains five major cell types, each producing a characteristic hormone. The somatotrophs (producing GH) constitute approximately 50% of anterior pituitary cells, making GH excess (acromegaly) and GH deficiency the most common anterior pituitary disorders.
| Cell Type | Hormone | Target Gland / Tissue | End-Product / Effect |
|---|---|---|---|
| Corticotroph | ACTH | Adrenal cortex | Cortisol (and adrenal androgens) |
| Thyrotroph | TSH | Thyroid gland | T3, T4 |
| Gonadotroph | LH, FSH | Gonads | Oestradiol / progesterone, testosterone, gametogenesis |
| Somatotroph | GH | Liver, bone, soft tissues | IGF-1, linear growth, metabolic effects |
| Lactotroph | PRL | Mammary gland | Lactation, gonadal suppression |
Posterior Pituitary Hormones
The posterior pituitary (neurohypophysis) stores and releases two hormones synthesised in the supraoptic and paraventricular nuclei of the hypothalamus:
- ADH (arginine vasopressin, AVP): Regulates water reabsorption via V2 receptors in the renal collecting duct. Deficiency causes central diabetes insipidus; excess causes SIADH.
- Oxytocin: Stimulates uterine contraction during labour and milk ejection during lactation. Emerging evidence supports a role in social bonding and behaviour.
Regulation & Feedback Mechanisms
The Negative Feedback Model
The HPA is regulated by classical negative feedback loops. Each target gland hormone inhibits the secretion of its upstream trophic hormone at both the hypothalamic and pituitary levels. This maintains circulating hormone concentrations within a narrow physiological range.
- Hypothalamic–Pituitary–Adrenal (HPA) axis: Cortisol suppresses CRH and ACTH secretion. The diurnal cortisol rhythm (peak at ~08:00, nadir at midnight) is driven by the suprachiasmatic nucleus and sleep–wake cycle.
- Hypothalamic–Pituitary–Thyroid (HPT) axis: T3 (both circulating and locally converted from T4 via type 2 deiodinase in the pituitary) suppresses TRH and TSH.
- Hypothalamic–Pituitary–Gonadal (HPG) axis: Oestradiol and testosterone suppress GnRH, LH and FSH. Inhibin B (from Sertoli cells / granulosa cells) selectively suppresses FSH.
- GH–IGF-1 axis: IGF-1 (produced by the liver in response to GH) feeds back to suppress GH secretion at the pituitary and hypothalamus. Ghrelin (stomach) and somatostatin (hypothalamus) provide additional regulation.
Pulsatile Secretion
Several HPA hormones are secreted in a pulsatile fashion rather than continuously. GnRH must be delivered in pulses (every 60–90 minutes) to stimulate LH and FSH; continuous GnRH paradoxically down-regulates gonadotrophs (the basis for GnRH agonist therapy). GH is secreted in bursts, predominantly during slow-wave sleep. These pulsatile patterns are clinically important when interpreting single hormone measurements.
The Hypophyseal Portal System
The hypophyseal portal system is a specialised capillary network connecting the median eminence of the hypothalamus to the anterior pituitary. It delivers releasing and inhibiting hormones in high local concentration, bypassing the systemic circulation. Disruption of the portal system (e.g., by pituitary stalk transection in trauma or surgery) causes hypopituitarism and paradoxical hyperprolactinaemia (loss of tonic dopamine inhibition).
Dynamic Testing
Dynamic stimulation tests are essential for evaluating the functional reserve of the HPA. Basal hormone levels may be misleadingly normal, particularly for GH and ACTH, which have pulsatile or diurnal secretion patterns. All dynamic tests should be performed in specialist endocrine units with appropriate monitoring and resuscitation facilities.
Insulin Tolerance Test (ITT)
The ITT remains the gold standard test for both GH and cortisol reserve assessment in Australia. Regular insulin (Actrapid®) 0.1–0.15 units/kg IV is administered to achieve symptomatic hypoglycaemia (blood glucose <2.2 mmol/L). Adequate hypoglycaemia must be confirmed; the test is invalid otherwise.
| Parameter | Normal Response | Interpretation |
|---|---|---|
| Peak cortisol | ≥500 nmol/L | Adequate adrenal reserve; <500 nmol/L suggests adrenal insufficiency |
| Peak GH | ≥5 µg/L (varies by assay) | Adequate GH reserve; lower thresholds suggest GHD |
Short Synacthen Test (SST)
The SST is the most widely used screening test for adrenal reserve in Australian hospitals. Synacthen (tetracosactide 250 µg IM or IV) is administered and serum cortisol measured at 0, 30 and 60 minutes. A peak cortisol ≥500 nmol/L at 30 or 60 minutes indicates adequate adrenal reserve. It is safe, widely available on MBS, and does not require endocrine supervision — making it the preferred first-line test in the general ward or ED setting.
Glucagon Stimulation Test (GST)
The GST is an alternative to the ITT for patients in whom insulin-induced hypoglycaemia is contraindicated. Glucagon 1 mg IM is administered and cortisol and GH measured at 0, 90, 120, 150 and 180 minutes. Normal response: peak cortisol ≥500 nmol/L and peak GH ≥3 µg/L. Nausea is a common side effect. The GST is available at major Australian endocrine centres.
TRH Stimulation Test
TRH (protirelin) 200 µg IV is administered with TSH measured at 0, 20 and 60 minutes. A normal TSH rise (increment ≥2 mU/L from baseline) excludes secondary hypothyroidism. In Australia, protirelin has limited commercial availability and the test is largely superseded by a combination of basal TSH and free T4 measurement, with clinical context.
GnRH Stimulation Test
GnRH 100 µg IV is administered with LH and FSH measured at 0, 30 and 60 minutes. An adequate LH rise (increment ≥2 IU/L) suggests intact gonadotroph reserve. The test is helpful in differentiating hypothalamic from pituitary causes of hypogonadism, particularly in the workup of delayed puberty.
GH Stimulation Tests
Because GH secretion is pulsatile, a random GH level is unreliable. Two stimulation tests are required to confirm adult GH deficiency (GHD). In Australia, the ITT is preferred; the GST or macimorelin test are alternatives. IGF-1 alone cannot exclude GHD, as up to 30% of adults with confirmed GHD have a normal IGF-1 level.
Clinical Disorders of the HPA
Hypopituitarism
Hypopituitarism refers to deficiency of one or more anterior pituitary hormones. Causes include pituitary adenomas (non-functioning and functioning), craniopharyngioma, pituitary surgery or radiotherapy, traumatic brain injury, subarachnoid haemorrhage, Sheehan syndrome, lymphocytic hypophysitis, haemochromatosis, sarcoidosis and infiltrative disorders.
Replacement therapy — order of priority:
Prolactinoma
Prolactinomas are the most common functioning pituitary adenoma. Microprolactinomas (<10 mm) predominate in women of reproductive age; macroprolactinomas (>10 mm) are more common in men. Elevated prolactin causes amenorrhoea, galactorrhoea, infertility in women, and erectile dysfunction, reduced libido and hypogonadism in men.
Cushing Disease
Cushing disease refers specifically to ACTH-secreting pituitary adenoma causing hypercortisolism. It accounts for approximately 70% of endogenous Cushing syndrome cases. Clinical features include central obesity, moon face, supraclavicular fat pads, purple striae, proximal myopathy, easy bruising, glucose intolerance, hypertension, osteoporosis and psychiatric disturbance.
First-line treatment: Transsphenoidal pituitary surgery by an experienced neurosurgeon (remission rate 65–90% for microadenomas). Second-line options include pituitary radiotherapy, bilateral adrenalectomy, and steroidogenesis inhibitors (ketoconazole, metyrapone, osilodrostat — specialist use).
Acromegaly
Acromegaly is caused by a GH-secreting pituitary adenoma in >95% of cases. Chronic GH/IGF-1 excess leads to acral enlargement, coarsened facial features, prognathism, soft tissue swelling, arthralgia, carpal tunnel syndrome, obstructive sleep apnoea, cardiomyopathy, colonic polyps and diabetes mellitus.
Treatment: Transsphenoidal surgery is first-line. Adjunctive therapy includes somatostatin receptor ligands (octreotide LAR, lanreotide), GH receptor antagonist (pegvisomant), and cabergoline for mild IGF-1 elevation. Pegvisomant is PBS-listed under authority for acromegaly refractory to somatostatin analogues.
Central Diabetes Insipidus (CDI)
CDI results from deficient ADH secretion, causing polyuria (>3 L/day), polydipsia, and the passage of dilute urine (urine osmolality <300 mOsm/kg). Aetiology includes pituitary surgery, trauma, craniopharyngioma, Langerhans cell histiocytosis, and autoimmune hypophysitis. Idiopathic CDI accounts for 25–50% of cases.
Syndrome of Inappropriate ADH Secretion (SIADH)
SIADH is characterised by euvolaemic hyponatraemia with inappropriately concentrated urine. Common causes in Australian practice include CNS disorders (meningitis, encephalitis, stroke), pulmonary disease (pneumonia, small-cell lung carcinoma), medications (SSRIs, carbamazepine, cyclophosphamide) and post-operative state. Management centres on treating the underlying cause, fluid restriction (500–1000 mL/day), and in severe/refractory cases, salt tablets with loop diuretics or tolvaptan.
Investigations
A systematic approach to HPA investigation includes basal hormone measurement, dynamic stimulation testing, and anatomical imaging. The following table summarises key investigations and their availability in Australia.
Special Populations
ATSI Health Considerations
Aboriginal and Torres Strait Islander peoples experience a disproportionate burden of endocrine and metabolic disease that directly and indirectly impacts HPA function and the interpretation of endocrine tests. The following considerations are important in clinical practice:
📚 References
- 1. Melmed S, Auchus RJ, Goldfine AB, Koenig RJ, Rosen CJ. Williams Textbook of Endocrinology. 14th ed. Philadelphia: Elsevier; 2020.
- 2. Fleseriu M, Auchus R, Bancos I, et al. Consensus on diagnosis and management of Cushing's disease: a guideline update. Lancet Diabetes Endocrinol. 2021;9(12):847–875.
- 3. Katznelson L, Laws ER, Melmed S, et al. Acromegaly: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2014;99(11):3933–3951.
- 4. Fleseriu M, Hashim IA, Engel T, et al. Hypothalamic–pituitary–adrenal axis dysfunction in adults: an Endocrine Society scientific statement. J Clin Endocrinol Metab. 2024;109(1):e1–e16.
- 5. Higham CE, Johannsson G, Shalet SM. Hypopituitarism. Lancet. 2016;388(10058):2403–2415.
- 6. Melmed S, Casanueva FF, Hoffman AR, et al. Diagnosis and treatment of hyperprolactinemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(2):273–288.
- 7. Australian Institute of Health and Welfare (AIHW). Diabetes: Australian Facts. Canberra: AIHW; 2023.
- 8. Royal Australasian College of Physicians (RACP). Position Statement: Aboriginal and Torres Strait Islander Health. Sydney: RACP; 2021.
- 9. Agha A, Rogers B, Sherlock M, et al. Anterior pituitary dysfunction in traumatic brain injury. Clin Endocrinol. 2004;61(5):581–588.
- 10. Grossman AB. Clinical review: The diagnosis and management of central hypothyroidism. J Clin Endocrinol Metab. 2024;109(2):e458–e469.
- 11. Molitch ME. Diagnosis and treatment of pituitary adenomas: a review. JAMA. 2017;317(5):516–524.
- 12. Pharmaceuticals Benefits Scheme (PBS). PBS Online. Australian Government Department of Health. Available at: https://www.pbs.gov.au. Accessed 2024.