📋 Key Information Summary
- Paget's disease of bone is a focal disorder of accelerated bone remodelling leading to enlarged, structurally disorganised bone; prevalence in Australia is approximately 3–4% in people aged >55 years, with higher rates in Anglo-Celtic populations.
- Most common sites: pelvis, lumbar spine, skull, femur, and tibia; polyostotic disease (>1 bone) present in ~70% of symptomatic patients.
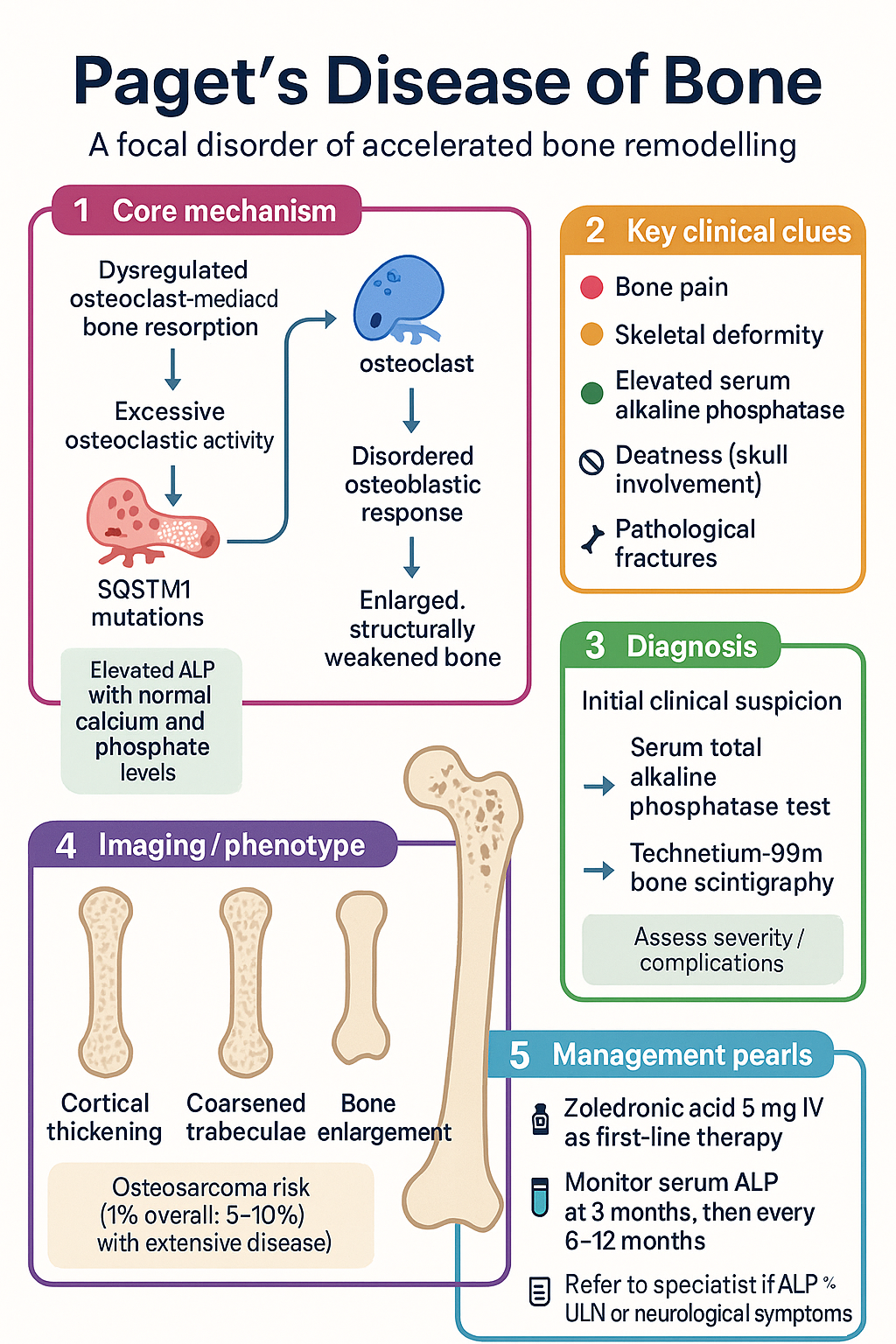
- The hallmark biochemical finding is an elevated serum total alkaline phosphatase (ALP) with normal calcium, phosphate, and liver transaminases.
- Plain radiographs remain the primary imaging modality — look for cortical thickening, coarsened trabeculae, and bone enlargement.
- Technetium-99m bone scintigraphy is the best modality for assessing disease extent (polyostotic vs monostotic) and detecting occult lesions.
- Indications for treatment: bone pain attributable to Paget's, periarticular pagetic bone causing osteoarthritis, pre-operative optimisation before orthopaedic surgery, hypercalcaemia, neurological compromise, and high-output cardiac failure.
- First-line therapy: zoledronic acid 5 mg IV single infusion — achieves ALP normalisation in >90% of patients with durable remission >5 years.
- Second-line/oral alternative: risedronate 30 mg PO daily for 2 months; pamidronate 60 mg IV over 2 h if zoledronic acid is contraindicated.
- Monitor serum total ALP at 3 months post-treatment, then every 6–12 months; re-treat if ALP rises >25% above nadir with recurrence of symptoms.
- Complications to screen for: pathological fractures, deafness (skull involvement), high-output cardiac failure (polyostotic disease), and secondary osteosarcoma (<1%).
- All patients require adequate calcium and vitamin D supplementation before and during bisphosphonate therapy to avoid hypocalcaemia.
- Refer to endocrinology or metabolic bone specialist if: ALP >3× ULN, skull involvement with neurological symptoms, suspected sarcomatous transformation, or refractory disease.
- Aboriginal and Torres Strait Islander Australians may present later with more advanced disease — ensure culturally safe assessment and access to IV bisphosphonate infusion services.
🎧 Audio Brief
Introduction & Australian Epidemiology
Paget's disease of bone (PDB) is a chronic focal disorder of bone remodelling characterised by disorganised and accelerated bone turnover. This results in enlarged, structurally weakened bone that is prone to deformity, fracture, and arthritic change. Although often asymptomatic, PDB can cause significant morbidity through bone pain, skeletal deformity, deafness, and pathological fracture.
PDB is common in individuals of Anglo-Celtic descent, and Australia has one of the highest prevalences worldwide. Population-based data from the Dubbo Osteoporosis Epidemiology Study and hospital discharge records estimate prevalence of approximately 3–4% in Australians aged over 55 years, rising to 8–10% in those over 80 years. Males are affected slightly more often than females (ratio ~1.3:1). PDB is rare before age 40 years.
In Australia, the condition is more prevalent in certain regions — notably parts of New South Wales, Victoria, and Queensland — likely reflecting the predominantly British and Irish heritage of early settler populations. Prevalence appears to be declining in younger birth cohorts, consistent with trends observed in the United Kingdom and New Zealand, possibly related to changing environmental exposures and improved childhood nutrition.
The disease is characterised by three phases: an initial osteoclastic phase of excessive bone resorption, a mixed osteoclastic–osteoblastic phase, and a late osteoblastic "burned-out" sclerotic phase. Disease may affect a single bone (monostotic, ~30%) or multiple bones (polyostotic, ~70%), with the pelvis, lumbar spine, skull, femur, and tibia most commonly involved.
Pathophysiology & Epidemiology
Pathophysiology
Paget's disease arises from dysregulated osteoclast-mediated bone resorption followed by disorganised osteoblastic bone formation. The fundamental abnormality lies within the osteoclast lineage, which produces excessive numbers of enlarged, hypernucleated osteoclasts that resorb bone at up to 20 times the normal rate. This triggers a compensatory but disordered osteoblastic response, producing woven bone with abnormal architecture.
Several genetic and environmental factors contribute:
- Genetic: Up to 40% of patients have a positive family history. Mutations in SQSTM1 (sequestosome-1 / p62) account for ~10–50% of familial cases and ~5–10% of sporadic cases in Australian cohorts. Other implicated genes include OPTN, NFκB, and VCP.
- Paramyxoviral hypothesis: Intracytoplasmic inclusions resembling measles virus nucleocapsids have been identified in pagetic osteoclasts, though definitive causation remains unproven.
- RANK/RANKL/OPG axis: Pagetic osteoclasts exhibit enhanced sensitivity to RANKL (receptor activator of nuclear factor kappa-B ligand) and overexpression of RANK, driving osteoclastogenesis. Denosumab targets this pathway.
- Environmental: Mechanical loading, low-dose radiation exposure, and possibly dietary calcium/vitamin D insufficiency in childhood may modulate risk.
Key Histological Features
| Phase | Histology | Clinical Correlate |
|---|---|---|
| Osteolytic (early) | Large osteoclasts with numerous nuclei (>20); excessive resorption lacunae | Bone pain, "blade of grass" advancing radiolucent fronts |
| Mixed (active) | Coupled osteoblast and osteoclast activity; disordered woven bone | Bone enlargement, deformity, elevated ALP |
| Sclerotic (burned-out) | Dense, sclerotic bone with reduced cellularity | Quiescent disease; ALP may normalise |
Clinical Features & Complications
The majority of patients with Paget's disease are asymptomatic at diagnosis, with the condition discovered incidentally through an elevated ALP or characteristic radiographic findings. When symptomatic, clinical features depend on the site and extent of skeletal involvement.
Presenting Features by Site
| Site | Symptoms | Complications |
|---|---|---|
| Skull | Headache, enlarged hat size, hot overlying skin | Sensorineural or conductive deafness, cranial nerve compression (II, V, VII, VIII), platybasia |
| Lumbar spine | Low back pain, stiffness | Spinal stenosis, nerve root compression, vertebral body enlargement |
| Pelvis / acetabulum | Hip/groin pain, waddling gait | Secondary osteoarthritis of hip, pelvic deformity |
| Femur / tibia | Anterior thigh pain, leg bowing | Fissure fractures (incomplete transverse, convex lateral cortex), pathological fracture, coxa vara |
| Humerus | Shoulder/arm pain, bowing | Pathological fracture |
Major Complications
- Pathological fracture: Transverse (chalk stick) fractures of long bones, especially femoral shaft; incomplete fissure fractures on the convex (tensile) surface are a warning sign.
- Deafness: Sensorineural (cochlear otosclerosis) or conductive (ossicular chain involvement); affects up to 50% of patients with skull Paget's.
- Secondary osteosarcoma: Occurs in <1% of patients overall but rises to ~5–10% in those with extensive polyostotic disease with skull involvement. Presents as sudden worsening pain and rapid swelling at a pagetic site. 5-year survival is poor.
- High-output cardiac failure: Arises when >15–20% of the skeleton is involved; the arteriovenous shunting within highly vascular pagetic bone increases cardiac output.
- Hypercalcaemia / hypercalciuria: Uncommon; more likely if the patient is immobilised with active polyostotic disease.
- Spinal cord / cauda equina compression: From vertebral body enlargement or epidural vascular dilatation — a neurological emergency.
- Immobility-related complications: VTE, pressure injuries, deconditioning from pain and deformity.
Investigations
Biochemical Investigations
Radiological Investigations
Other Assessments
- Audiometry: If skull involvement — baseline and monitor for progressive hearing loss.
- Echocardiography: If extensive polyostotic disease (>15% skeleton) or features of high-output cardiac failure.
- DXA (Dual-energy X-ray Absorptiometry): Standard osteoporosis assessment; MBS Item 12322. Pagetic bone may falsely elevate DXA values at involved sites — preferentially measure non-pagetic sites.
- Genetic testing for SQSTM1: Specialist referral. Offered if young-onset (<55 years), strong family history, or severe disease phenotype. Available through clinical genetics services in major Australian centres.
Management — Bisphosphonates & Medical Therapy
Indications for Treatment
Not all patients with Paget's disease require pharmacological treatment. Asymptomatic patients with isolated mild ALP elevation may be monitored. The following are established indications for bisphosphonate therapy:
- Bone pain attributable to pagetic activity (not osteoarthritis)
- Pre-operative optimisation before orthopaedic surgery on pagetic bone
- Prevention of complications: pathological fracture, neurological compression, spinal stenosis
- Hypercalcaemia or hypercalciuria due to active disease
- High-output cardiac failure secondary to polyostotic Paget's
- Involvement of weight-bearing bones with advancing osteolytic fronts
- Asymptomatic disease with ALP >2× ULN (treat to reduce long-term complications)
First-Line: Zoledronic Acid
Zoledronic acid achieves biochemical remission (ALP normalisation) in >90% of patients and has superior efficacy and durability compared with oral bisphosphonates. A single infusion provides remission lasting >5 years in the majority. It is the preferred agent when IV access is available.
Second-Line: Risedronate
Alternative Agents
Monitoring Response to Treatment
Symptomatic & Supportive Measures
- Analgesia: Paracetamol (first-line), NSAIDs (if no contraindication), or low-dose opioids for refractory pain.
- Physiotherapy: Maintain mobility, gait aids if needed, falls prevention.
- Calcium + vitamin D: Calcium 500–1000 mg/day + cholecalciferol 1000–2000 IU/day for all patients on bisphosphonates.
- Hearing aids: If sensorineural deafness from skull involvement.
- Orthopaedic referral: For significant deformity, pathological fracture, or planned joint replacement.
- Cardiology input: If high-output cardiac failure suspected.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Singer FR, Bone HG, Hosking DJ, et al. Paget's disease of bone: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2014;99(12):4408–4422.
- 2. Ralston SH, Corral-Gudino L, Cooper C, et al. Diagnosis and management of Paget's disease of bone in adults: a clinical guideline. J Bone Miner Res. 2019;34(4):579–604.
- 3. Tan A, Goodman K, Walker A, et al. Long-term randomized trial of intensive versus symptomatic management in Paget's disease of bone: the PRISM-EZ study. J Bone Miner Res. 2017;32(6):1165–1173.
- 4. Reid IR, Miller P, Lyles K, et al. Comparison of a single infusion of zoledronic acid with risedronate for Paget's disease. N Engl J Med. 2005;353(9):898–908.
- 5. Australian Institute of Health and Welfare (AIHW). Osteoporosis and Paget's disease in Australia. Canberra: AIHW; 2023. Cat. no. PHE 309.
- 6. The Royal Australian College of General Practitioners (RACGP). Guidelines for preventive activities in general practice. 10th ed. East Melbourne: RACGP; 2023.
- 7. Ebeling PR. Clinical practice: osteoporosis in men. N Engl J Med. 2008;358(14):1474–1482.
- 8. Cundy T, Naot D, Bava U, et al. SQSTM1 mutations in Paget's disease of bone in Australia: prevalence, genotype–phenotype correlation, and novel mutations. J Bone Miner Res. 2015;30(10):1892–1899.
- 9. National Health and Medical Research Council (NHMRC). Australian guidelines to reduce health risks from drinking alcohol. Canberra: NHMRC; 2020. [Relevant for bone health counselling.]
- 10. Ooi CG, Walsh CA, Gallagher JA, et al. Paget's disease of bone in Australia: prevalence and quality of life. Aust N Z J Med. 1999;29(3):382–388.
- 11. Devogelaer JP, Geusens P, Daci E, et al. Remission over 3 years in patients with Paget disease of bone treated with a single intravenous infusion of zoledronic acid. Arthritis Rheum. 2007;56(5):1563–1571.
- 12. Pharmaceutical Benefits Scheme (PBS). Zoledronic acid. Australian Government Department of Health. Available at: https://www.pbs.gov.au [Accessed 2025].
- 13. National Aboriginal Community Controlled Health Organisation (NACCHO) & RACGP. National guide to a preventive health assessment for Aboriginal and Torres Strait Islander people. 3rd ed. South Melbourne: RACGP; 2018.