📋 Key Information Summary
- Definition: Primary amenorrhoea — no menarche by age 15 years or no secondary sexual characteristics by 13 years. Secondary amenorrhoea — cessation of menses for ≥3 months (or ≥6 months in oligomenorrhoeic women) in a previously menstruating individual.
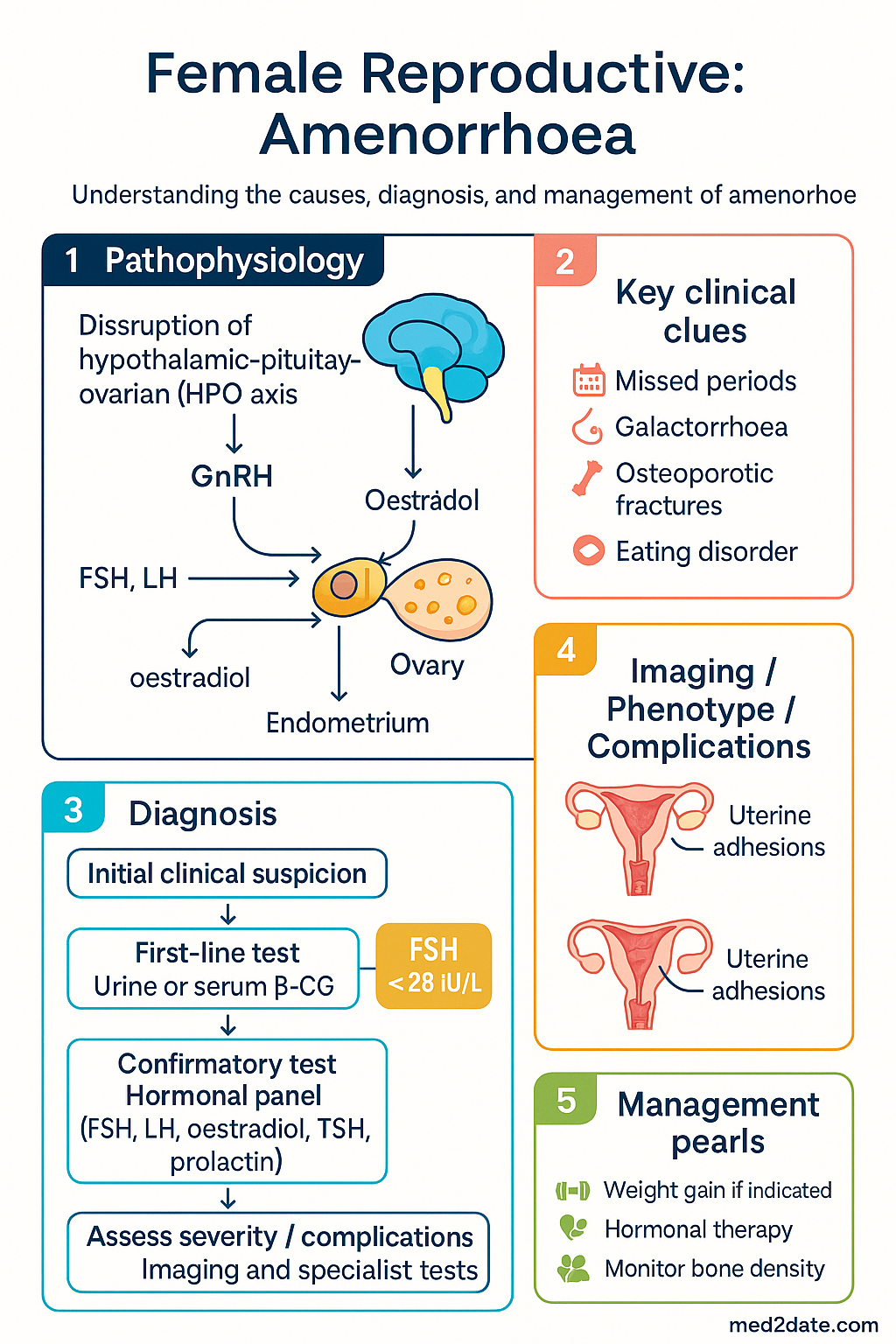
- First investigation for all patients: Urine or serum β-hCG — pregnancy is the most common cause of secondary amenorrhoea.
- Key hormonal panel: FSH, LH, oestradiol, TSH, prolactin, and free T4 form the essential initial work-up for both primary and secondary amenorrhoea.
- Hypergonadotrophic hypogonadism (FSH >25 IU/L) suggests ovarian failure; karyotype is mandatory in primary amenorrhoea to exclude Turner syndrome (45,X) and Swyer syndrome (46,XY DSD).
- Functional hypothalamic amenorrhoea (FHA) is the most common cause of secondary amenorrhoea in reproductive-age Australians and is a diagnosis of exclusion after organic causes are ruled out.
- Prolactin >1000 mIU/L warrants MRI pituitary (sella turcica) to exclude a macroprolactinoma; levels 500–1000 may represent microprolactinoma, medications, or stress.
- Polycystic ovary syndrome (PCOS) is diagnosed by Rotterdam criteria (two of three: oligo/anovulation, hyperandrogenism, polycystic ovaries on ultrasound) and is a leading cause of secondary amenorrhoea.
- Asherman syndrome should be suspected in any patient with amenorrhoea following uterine instrumentation (especially post-partum curettage or repeated D&C) and is confirmed on hysteroscopy.
- Bone protection: Oestrogen deficiency from any cause accelerates bone loss; all patients with prolonged amenorrhoea (>12 months) require a DXA scan and calcium/vitamin D optimisation.
- Fertility implications: Ovulation induction (letrozole first-line for PCOS, gonadotrophins for hypogonadotrophic hypogonadism) and referral to a fertility specialist should be discussed early where fertility is desired.
- Medicare rebates: Hormonal investigations (FSH, LH, oestradiol, TSH, prolactin) are MBS-rebatable under GP-requested pathology. MRI pituitary requires specialist referral for Medicare-eligible rebate in most cases.
- Safety alert: All patients with secondary amenorrhoea must have a pregnancy test before imaging with ionising radiation or initiating hormonal therapy.
🎧 Audio Brief
Introduction & Australian Epidemiology
Amenorrhoea is the absence of menstruation and is classified as primary (no menarche by age 15 years in the presence of normal secondary sexual characteristics, or by age 13 years with no secondary sexual characteristics) or secondary (cessation of menses for ≥3 months in a previously menstruating woman, or ≥6 months in a woman with prior oligomenorrhoea).
In Australia, secondary amenorrhoea is far more common than primary amenorrhoea. Functional hypothalamic amenorrhoea (FHA) and polycystic ovary syndrome (PCOS) together account for approximately two-thirds of secondary amenorrhoea presentations in primary care. Primary amenorrhoea, though less frequent, requires a more urgent and systematic work-up to exclude anatomical, chromosomal, and endocrine abnormalities.
PCOS affects an estimated 12–21% of Australian women of reproductive age, with higher prevalence in Aboriginal and Torres Strait Islander women, and is the most common endocrine disorder presenting with amenorrhoea or oligomenorrhoea. Turner syndrome (45,X) occurs in approximately 1 in 2500 live female births and is the most common chromosomal cause of primary amenorrhoea.
Early identification and appropriate work-up of amenorrhoea is essential — not only for fertility but also for prevention of osteoporosis, endometrial hyperplasia, cardiovascular disease, and psychological morbidity.
Classification & Pathophysiology
The hypothalamic–pituitary–ovarian (HPO) axis governs normal menstruation. Disruption at any level — hypothalamus, pituitary, ovary, or outflow tract — can produce amenorrhoea.
Primary Amenorrhoea
Primary amenorrhoea is defined as the absence of menarche by age 15 years with normal secondary sexual characteristics, or by age 13 years without secondary sexual development. It may be caused by:
- Gonadal dysgenesis — Turner syndrome (45,X) or mixed gonadal dysgenesis causing streak gonads and absent oestrogen production.
- Müllerian agenesis (MRKH syndrome) — congenital absence of the uterus and upper vagina with normal ovaries and karyotype (46,XX).
- Androgen insensitivity syndrome (AIS) — 46,XY karyotype with complete androgen receptor resistance; phenotypically female with absent uterus and undescended testes.
- Constitutional delay of puberty — a diagnosis of exclusion; more common in males but occurs in females, often with a family history.
- Congenital hypothalamic or pituitary defects — Kallmann syndrome (GnRH deficiency + anosmia), isolated GnRH deficiency.
Secondary Amenorrhoea
Secondary amenorrhoea is cessation of menses for ≥3 months in a woman who has previously menstruated. The causes are organised anatomically through the HPO axis:
| Level | Mechanism | Examples |
|---|---|---|
| Hypothalamic | Suppressed GnRH pulsatility | Functional hypothalamic amenorrhoea (stress, weight loss, exercise), Kallmann syndrome, infiltrative disease |
| Pituitary | Excess or deficient pituitary hormones | Hyperprolactinaemia, Sheehan syndrome, pituitary adenoma, hypophysitis |
| Ovarian | Ovarian failure or hormone excess | Premature ovarian insufficiency (POI), PCOS, gonadal dysgenesis |
| Uterine / Outflow | Endometrial destruction or outflow obstruction | Asherman syndrome, cervical stenosis, vaginal septum |
Normal menstruation requires an intact HPO axis, patent outflow tract, and responsive endometrium. A systematic anatomical approach ensures no cause is overlooked.
Causes — Hypothalamic
Functional Hypothalamic Amenorrhoea (FHA)
FHA is the most common cause of secondary amenorrhoea in reproductive-age Australian women. It results from suppression of GnRH pulsatility due to:
- Energy deficit / low body weight — BMI <18.5 kg/m² or rapid weight loss >10% body weight; commonly seen in eating disorders (anorexia nervosa, bulimia nervosa).
- Excessive exercise — endurance athletes, ballet dancers; the "female athlete triad" (low energy availability, menstrual dysfunction, low bone mineral density).
- Psychological stress — acute or chronic stress, bereavement, major life events.
FHA is a diagnosis of exclusion. Patients typically have low or low-normal FSH, LH, and oestradiol with no structural lesion on imaging.
Organic Hypothalamic Causes
- Kallmann syndrome — congenital GnRH deficiency with anosmia/hyposmia; may present as primary or secondary amenorrhoea.
- Infiltrative / destructive lesions — sarcoidosis, histiocytosis, cranial irradiation, traumatic brain injury.
- Medications — antipsychotics (via dopamine antagonism), chronic opioids, GnRH agonists.
Causes — Pituitary
Hyperprolactinaemia
Prolactin elevation suppresses GnRH pulsatility, causing amenorrhoea and galactorrhoea. Common causes include:
- Prolactinoma — the most common functioning pituitary adenoma; microprolactinoma (<10 mm) is more common in women; macroprolactinoma (≥10 mm) may cause visual field defects from optic chiasm compression.
- Medications — antipsychotics (risperidone, haloperidol), metoclopramide, domperidone, SSRI, methyldopa.
- Primary hypothyroidism — elevated TRH stimulates prolactin release.
- Macroprolactin — high-molecular-weight prolactin complex that is biologically inactive; causes a falsely elevated prolactin level (check with polyethylene glycol precipitation if suspected).
Hypopituitarism
Deficiency of one or more anterior pituitary hormones may cause amenorrhoea via gonadotrophin insufficiency. Causes include:
- Sheehan syndrome — post-partum pituitary necrosis due to obstetric haemorrhage; may present months to years after delivery.
- Pituitary adenoma or craniopharyngioma — mass effect destroying normal pituitary tissue.
- Pituitary apoplexy — acute haemorrhage or infarction within a pituitary adenoma; a neurosurgical emergency.
- Autoimmune hypophysitis — increasingly recognised with immune checkpoint inhibitor therapy.
Causes — Ovarian
Premature Ovarian Insufficiency (POI)
POI is defined as loss of ovarian function before age 40 years, characterised by amenorrhoea, elevated FSH (>25 IU/L on two occasions ≥4 weeks apart), and low oestradiol. Affects approximately 1% of women under 40 and 0.1% under 30.
- Idiopathic — most common; ~50–90% of cases.
- Autoimmune — associated with autoimmune thyroid disease (most common), adrenal insufficiency (autoimmune polyglandular syndrome), and coeliac disease.
- Iatrogenic — chemotherapy (especially alkylating agents: cyclophosphamide, busulfan), pelvic irradiation, bilateral oophorectomy.
- Chromosomal — Turner syndrome (45,X), Fragile X premutation (FMR1, 55–200 CGG repeats).
- Infections — mumps oophoritis (rare in vaccinated populations).
Karyotype is indicated in all patients with POI presenting before age 30. FMR1 premutation testing should be performed in all women with unexplained POI, as it has implications for offspring risk of Fragile X syndrome.
Polycystic Ovary Syndrome (PCOS)
Diagnosed using Rotterdam criteria — requires two of three:
- Oligomenorrhoea or anovulation (amenorrhoea in severe cases).
- Clinical and/or biochemical hyperandrogenism (acne, hirsutism, elevated free testosterone or FAI).
- Polycystic ovarian morphology on ultrasound (≥20 follicles per ovary or ovarian volume >10 mL, using modern transducer technology).
Exclude thyroid disease, hyperprolactinaemia, non-classical congenital adrenal hyperplasia (21-hydroxylase deficiency — check 17-OH progesterone), and androgen-secreting tumours (testosterone >5 nmol/L warrants urgent pelvic imaging).
Causes — Uterine (Outflow Tract)
Asherman Syndrome
Intrauterine adhesions (synechiae) causing partial or complete obliteration of the endometrial cavity. Almost always acquired following uterine instrumentation — most commonly post-partum curettage, repeated dilatation and curettage (D&C) for miscarriage, or endometrial ablation. Rarely congenital.
Diagnosis: Transvaginal ultrasound may suggest thin or absent endometrium. Gold standard is hysteroscopy, which allows simultaneous diagnosis and treatment (adhesiolysis).
Müllerian Agenesis (MRKH Syndrome)
Congenital absence of the uterus and upper two-thirds of the vagina in a 46,XX individual with normal ovaries. Presents as primary amenorrhoea with normal secondary sexual characteristics. Affects approximately 1 in 4500 female births. Associated renal anomalies (solitary kidney, pelvic kidney) in ~30% and skeletal anomalies in ~12%.
Diagnosis: MRI pelvis is the imaging modality of choice to delineate anatomy. Karyotype confirms 46,XX. FSH/LH/oestradiol are normal.
Cervical Stenosis
May be congenital or acquired following cervical surgery (cone biopsy, LLETZ) or radiation. Causes haematometra (retained menstrual blood) if complete. Treatment: cervical dilation.
Androgen Insensitivity Syndrome (AIS)
Complete AIS (CAIS): 46,XY karyotype with non-functional androgen receptors. Phenotypically female breast development (driven by aromatisation of testosterone to oestradiol) but absent uterus and absent or sparse pubic/axillary hair. Presents as primary amenorrhoea. Gonads (testes) carry a 2–5% risk of malignancy and are typically removed after puberty; oestrogen replacement is then required.
Investigations
A systematic, tiered approach avoids unnecessary testing while ensuring critical diagnoses are not missed.
Step 1 — Essential First-Line Investigations (All Patients)
Step 2 — Second-Line Investigations (Guided by First-Line Results)
Step 3 — Specialist Investigations
Management
Management is aetiology-driven. Key principles include treating the underlying cause, managing oestrogen deficiency (bone and cardiovascular protection), preserving fertility where desired, and addressing psychosocial impact.
Functional Hypothalamic Amenorrhoea (FHA)
- Address the precipitant: Weight restoration to BMI >18.5 kg/m² (target BMI ~20–25 kg/m²); reduce excessive exercise; manage psychological stress (CBT has level-I evidence in FHA).
- Oestrogen replacement: Combined oral contraceptive pill (COCP) or cyclic oestrogen–progestogen therapy for bone and cardiovascular protection if menses do not return within 6–12 months of lifestyle modification.
- Calcium 1000–1200 mg/day + Vitamin D 1000–2000 IU/day if dietary intake is inadequate or 25-OH vitamin D <75 nmol/L.
- Fertility: Pulsatile GnRH therapy (specialist only) has the highest ovulation rate; gonadotrophin therapy (FSH ± LH) is an alternative.
Hyperprolactinaemia
- Medication-induced: If clinically feasible, discontinue or switch the causative agent (e.g., switch antipsychotic to aripiprazole, a partial dopamine agonist).
- Microprolactinoma or idiopathic: Dopamine agonist therapy is first-line.
- Macroprolactinoma (>10 mm): Dopamine agonist first-line (surgery reserved for intolerance, resistance, or acute visual compromise). Monitor with serial prolactin levels and MRI at 3 months, then annually.
Premature Ovarian Insufficiency (POI)
- Hormone replacement therapy (HRT) is recommended at least until the average age of natural menopause (51–52 years) to mitigate osteoporosis, cardiovascular risk, and menopausal symptoms.
- First-line: Sequential oestrogen–progestogen HRT for women with an intact uterus, or oestrogen-only HRT post-hysterectomy.
- Alternative: COCP provides adequate replacement and contraception simultaneously (if pregnancy is undesired).
- Autoimmune screening: TSH, anti-adrenal antibodies (21-hydroxylase antibodies), coeliac serology (tTG-IgA), fasting glucose at diagnosis and annually.
- Fertility: Oocyte donation with IVF is the primary option for women with POI seeking pregnancy. Spontaneous conception occurs in 5–10% but is unpredictable.
Polycystic Ovary Syndrome (PCOS)
- Lifestyle modification is the first-line intervention for all women with PCOS — weight loss of 5–10% improves ovulatory function.
- Cycle regulation: Cyclical progestogen (medroxyprogesterone acetate 10 mg for 10–14 days per month) or COCP to prevent endometrial hyperplasia. Women with amenorrhoea >3 months without progestogen exposure are at increased risk of endometrial hyperplasia and carcinoma.
- Ovulation induction (fertility):
Asherman Syndrome
- Hysteroscopic adhesiolysis is the treatment of choice — performed by a gynaecologist with expertise in intrauterine surgery.
- Post-operative: Oestrogen therapy (oestradiol valerate 2 mg PO daily for 2–3 cycles) to stimulate endometrial regeneration. Intrauterine balloon stent or IUD placement may be used to prevent re-adhesion.
- Fertility: Pregnancy rates of 40–60% following adhesiolysis; IVF may be required if endometrium remains thin or re-adhesion recurs.
MRKH Syndrome
- Vaginal dilation is the first-line non-surgical approach (Frank method); success rates >90% with compliance.
- Surgical neovagina (McIndoe, Vecchietti, or Davydov techniques) if dilation fails.
- Fertility: Gestational surrogacy (with the patient's own oocytes) or uterine transplant (experimental; limited centres in Australia). Counsel regarding psychosocial support and peer groups (e.g., MRKH Australia).
Bone Protection and Cardiovascular Risk Management
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Quick Reference — Investigation Algorithm
📚 References
- 1. The Practice Committee of the American Society for Reproductive Medicine. Current evaluation of amenorrhea. Fertil Steril. 2008;90(5 Suppl):S219–S225.
- 2. Munro MG, Critchley HOD, Broder MS, Fraser IS; FIGO Working Group on Menstrual Disorders. FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding. Int J Gynaecol Obstet. 2011;113(1):3–13.
- 3. Teede HJ, Misso ML, Costello MF, et al. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Hum Reprod. 2018;33(9):1602–1618.
- 4. Webber L, Davies M, Anderson R, et al. ESHRE Guideline: management of women with premature ovarian insufficiency. Hum Reprod. 2016;31(5):926–937.
- 5. Melmed S, Casanueva FF, Hoffman AR, et al. Diagnosis and treatment of hyperprolactinemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(2):273–288.
- 6. Royal Australian College of General Practitioners (RACGP). Polycystic ovary syndrome: position statement. East Melbourne: RACGP; 2020.
- 7. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander health performance framework 2020 summary report. Canberra: AIHW; 2020.
- 8. Hoek A, Schoemaker J, Drexhage HA. Premature ovarian failure and ovarian autoimmunity. Endocr Rev. 1997;18(1):107–134.
- 9. Deans R, Abbott J. Review of intrauterine adhesions. J Minim Invasive Gynecol. 2010;17(5):555–569.
- 10. Gordon CM, Ackerman KE, Berga SL, et al. Functional hypothalamic amenorrhea: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2017;102(5):1413–1439.
- 11. Legro RS, Brzyski RG, Diamond MP, et al. Letrozole versus clomiphene for infertility in the polycystic ovary syndrome. N Engl J Med. 2014;371(2):119–129.
- 12. Atay V, Cam C, Muhcu M, Cam M, Karateke A. Comparison of letrozole and clomiphene citrate in women with polycystic ovaries undergoing ovarian stimulation. J Int Med Res. 2006;34(1):73–76.
- 13. Australian Government Department of Health. Medicare Benefits Schedule (MBS) Online. Canberra: Commonwealth of Australia; 2024.
- 14. Donnez J, Dolmans MM. Uterus transplantation: from animal models and human subjects to clinical practice. J Clin Endocrinol Metab. 2019;104(9):3581–3590.