📋 Key Information Summary
- Hypercalcaemia is defined as a serum adjusted calcium >2.60 mmol/L. Severe hypercalcaemia (≥3.50 mmol/L) is a medical emergency.
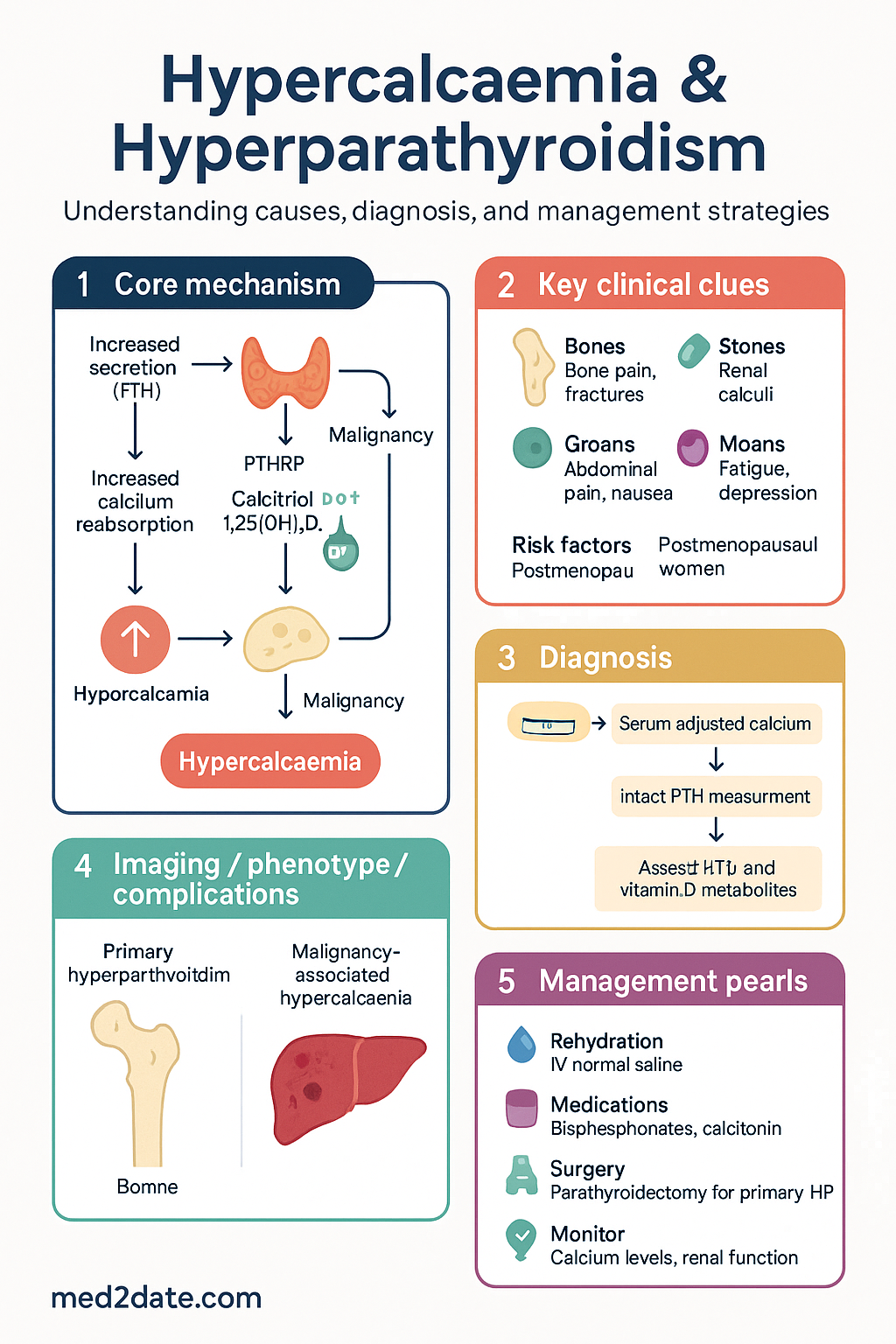
- The two most common causes are primary hyperparathyroidism (HPT) in outpatient settings and malignancy in hospitalised patients.
- Measurement of intact parathyroid hormone (PTH) is the single most important test to differentiate PTH-dependent from PTH-independent causes.
- PTH-dependent hypercalcaemia (raised PTH) is most commonly due to primary HPT (adenoma, hyperplasia).
- PTH-independent hypercalcaemia (suppressed PTH) requires measurement of PTHrP and vitamin D metabolites; malignancy (solid tumours, myeloma) is the leading cause.
- The classic mnemonic "Bones, Stones, Abdominal Groans, Psychic Moans and Fatigue Overtones" describes the varied clinical features.
- Acute management centres on aggressive IV normal saline rehydration to promote calciuresis.
- For moderate-severe hypercalcaemia, add a bisphosphonate (zoledronic acid or pamidronate) or denosumab for refractory cases.
- Calcitonin provides rapid but transient reduction in calcium and is useful as a bridge.
- Surgery (parathyroidectomy) is the definitive treatment for primary HPT, indicated for symptomatic patients or those meeting surgical criteria.
- Aboriginal and Torres Strait Islander peoples may have a higher prevalence of hyperparathyroidism and require culturally safe care pathways.
- Always consider lithium and thiazide diuretic use as contributing factors in PTH-dependent hypercalcaemia.
🎧 Audio Brief
Introduction & Australian Epidemiology
Hypercalcaemia is the most common metabolic disorder associated with cancer, and one of the most frequent endocrine abnormalities encountered in general practice. Its presence often signals serious underlying disease. In Australia, primary hyperparathyroidism (pHPT) is the most common cause in the ambulatory setting, with an estimated incidence of 0.2-0.3%, affecting postmenopausal women disproportionately. Malignancy-associated hypercalcaemia is the predominant cause in hospitalised patients, occurring in 10-30% of advanced cancer cases.
A systematic approach centred on parathyroid hormone (PTH) measurement is essential to guide investigation and targeted management. This guideline provides a framework for the diagnosis, investigation, and acute and chronic management of hypercalcaemia for Australian clinicians.
Pathophysiology & Causes
Normal serum calcium homeostasis is maintained by the integrated actions of PTH and 1,25-dihydroxyvitamin D (calcitriol). Hypercalcaemia results from increased bone resorption, increased gastrointestinal absorption, or decreased renal calcium excretion.
PTH-Dependent Causes
- Primary Hyperparathyroidism: Single adenoma (80-85%), multigland hyperplasia (10-15%), carcinoma (<1%).
- Lithium Therapy: Alters calcium set-point; long-term use.
- Familial Hypocalciuric Hypercalcaemia (FHH): Benign autosomal dominant condition; calcium:creatinine clearance ratio <0.01.
- Tertiary Hyperparathyroidism: Autonomous PTH secretion after long-standing secondary HPT (e.g., chronic kidney disease).
PTH-Independent Causes
- Malignancy:
- Humoral Hypercalcaemia of Malignancy: PTHrP secretion (squamous cell, renal, breast, bladder).
- Osteolytic Metastases: Local cytokine release (breast, myeloma).
- 1,25-Dihydroxyvitamin D Mediated: Lymphomas, granulomatous disease (sarcoidosis, TB).
- Endocrine: Thyrotoxicosis, phaeochromocytoma, adrenal insufficiency.
- Drugs: Vitamin D/A intoxication, thiazides (mild effect), theophylline toxicity.
- Other: Prolonged immobilisation, severe dehydration, Paget's disease.
Clinical Features (Bones, Stones, Groans, Psychic Moans)
Symptoms are often non-specific and correlate poorly with the absolute calcium level but more closely with the rate of rise. The classic mnemonic is commonly used as a framework.
| Category | Manifestations |
|---|---|
| Bones | Bone pain, pathological fractures, osteitis fibrosa cystica, subperiosteal resorption, osteoporosis. |
| Stones | Renal calculi (calcium oxalate/phosphate), nephrocalcinosis, polyuria, polydipsia (nephrogenic DI). |
| Abdominal Groans | Anorexia, nausea, vomiting, constipation, peptic ulcer disease, acute pancreatitis. |
| Psychic Moans | Lethargy, fatigue, depression, anxiety, cognitive dysfunction, confusion, psychosis, coma (in severe cases). |
| Other | Hypertension, shortened QTc, cardiac arrhythmias, muscle weakness. |
Investigations (PTH, PTHrP, Calcium, Imaging)
Initial and Specific Biochemical Tests
Localisation Imaging for Hyperparathyroidism
Imaging is pre-surgical and not for diagnosis. It guides the surgeon if minimally invasive parathyroidectomy is planned.
Management (IV Fluids, Bisphosphonates, Surgery)
Acute / Severe Hypercalcaemia Management
This is a step-wise, often concurrent, approach.
Surgical Management: Parathyroidectomy
Refer all patients with symptomatic primary HPT and consider in asymptomatic patients who meet surgical criteria.
| Surgical Indication (Any One) | Threshold |
|---|---|
| Age | <50 years |
| Serum Calcium | >0.25 mmol/L above normal range |
| Skeletal | T-score ≤ −2.5 at any site, vertebral fracture |
| Renal | eGFR <60 mL/min, 24-hr urine calcium >10 mmol/day, nephrolithiasis/nephrocalcinosis |
Special Populations
Aboriginal and Torres Strait Islander Health
📚 References
- 1. Sia KK, Clarke B, Kumar S. Hypercalcaemia in the Australian setting: causes and management. Med J Aust. 2022;216(9):456-461.
- 2. The Royal Australian College of General Practitioners (RACGP). Red Book: Guidelines for preventive activities in general practice. 10th edn. East Melbourne: RACGP; 2020.
- 3. Australian Institute of Health and Welfare (AIHW). Cancer in Australia 2021. Cancer series no.133. Cat. no. CAN 144. Canberra: AIHW; 2021.
- 4. Endocrine Society of Australia (ESA). Position statement on the management of primary hyperparathyroidism. Intern Med J. 2021;51(Suppl 1):5-15.
- 5. Bilezikian JP, Khan AA, Potts JT Jr, et al. Guidelines for the management of asymptomatic primary hyperparathyroidism: summary statement from the Third International Workshop. J Clin Endocrinol Metab. 2009;94(2):335-339.
- 6. Pharmaceuticals Benefits Scheme (PBS). Zoledronic Acid. Australian Government Department of Health. Available at: https://www.pbs.gov.au [Accessed October 2023].
- 7. Medical Services Advisory Committee (MSAC). Public Summary Document: Parathyroid imaging. Application No. 1273.1. Commonwealth of Australia; 2018.
- 8. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2017.
- 9. Aboriginal and Torres Strait Islander Health Performance Framework. Health system performance: Access to health services. Australian Institute of Health and Welfare. 2023.
- 10. Bushinsky DA, Monk RD. Calcium. Lancet. 1998;352(9124):306-311.