📋 Key Information Summary
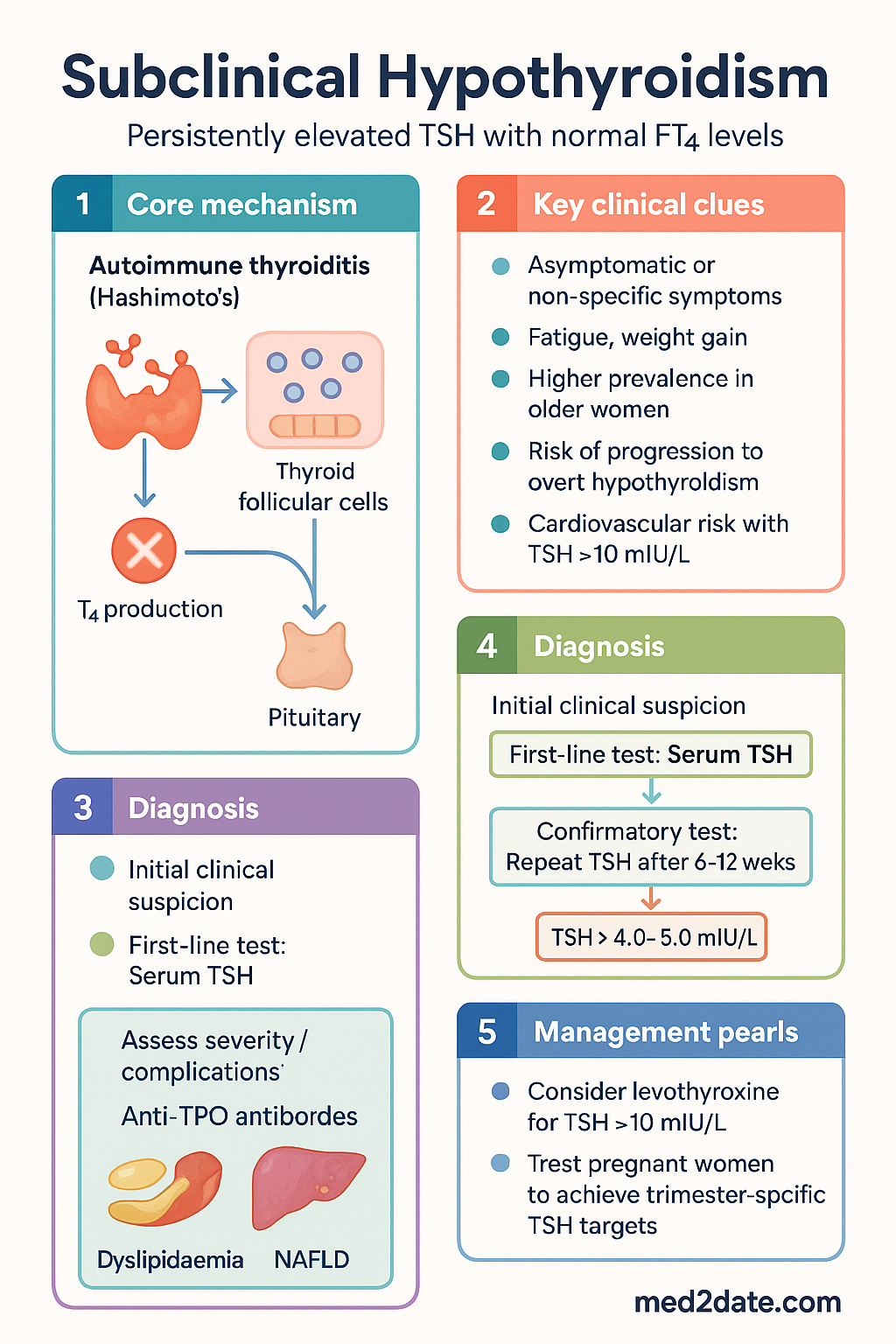
- Definition: Persistently elevated serum TSH (>4.0–5.0 mIU/L) with a normal free thyroxine (FT4) level.
- Prevalence: Common, affecting 4–10% of the general population, increasing with age and in women.
- Aetiology: Most commonly due to early Hashimoto's thyroiditis. Iodine status in Australia is generally adequate.
- Key Risk: Associated with progression to overt hypothyroidism (~2–5% per year), dyslipidaemia, and potential increased cardiovascular risk, particularly with TSH >10 mIU/L.
- Symptoms: Often asymptomatic. Non-specific symptoms (fatigue, weight gain) may be present but are not reliably diagnostic.
- Diagnosis: Requires confirmation of elevated TSH on at least two occasions 6–12 weeks apart, excluding transient causes.
- Treatment Indications: Consider levothyroxine for TSH >10 mIU/L, symptomatic patients, women planning pregnancy/pregnant, and those with high cardiovascular risk.
- Treatment Goal: Normalise TSH (target 0.5–2.5 mIU/L) and alleviate symptoms, avoiding over-treatment.
- First-Line Therapy: Levothyroxine (Oroxine®, Eutroig®) - low dose initiation (e.g., 25–50 mcg daily) with titration.
- Monitoring: TSH every 6–8 weeks after initiation/dose change, then annually once stable.
- Special Populations: Aggressive treatment in pregnancy (TSH target <2.5 mIU/L in T1). Caution in elderly/cardiac disease (start very low dose).
- ATSI Considerations: Increased prevalence and barriers to specialist access require community-tailored management and monitoring support.
🎧 Audio Brief
Introduction & Australian Epidemiology
Subclinical hypothyroidism (SCH) is a common biochemical abnormality characterised by an elevated serum thyroid-stimulating hormone (TSH) level in the presence of a normal free thyroxine (FT4) concentration. It represents a state of mild, compensated thyroid failure. While often asymptomatic, SCH has been associated with non-specific symptoms and adverse long-term health outcomes.
In Australia, the prevalence of SCH is estimated at 4–10% of the adult population, with higher rates in women (particularly older women) and in regions with historical iodine deficiency, although mandatory iodine fortification of bread (2009) has improved population iodine status. Data from the Australian Bureau of Statistics and AIHW indicate significant variation in management, highlighting the need for clear clinical guidance.
This guideline provides a framework for the investigation, risk stratification, and management of SCH in Australian primary care and specialist settings, aligning with contemporary evidence and local healthcare structures.
Epidemiology & Aetiology
Prevalence
Population-based studies, including Australian data, report a SCH prevalence of approximately 4–10%. Key determinants include:
- Age: Prevalence increases with age, exceeding 15% in women over 60 years.
- Sex: Female to male ratio is approximately 5:1.
- Iodine Intake: Both deficiency and excess can be contributory. Australia's mandatory fortification programme has made severe deficiency rare.
- Geography: Historical iodine-deficient areas (e.g., parts of Tasmania, Victorian Alps) may have higher rates.
Aetiology
The most common cause is autoimmune thyroiditis (Hashimoto's disease), identified by the presence of anti-thyroid peroxidase (anti-TPO) antibodies. Other causes include:
- Iatrogenic: Post-radioactive iodine therapy, partial thyroidectomy, external neck irradiation.
- Drug-induced: Amiodarone, lithium, immune checkpoint inhibitors, tyrosine kinase inhibitors.
- Transient causes: Subacute thyroiditis recovery, non-thyroidal illness syndrome resolution.
Clinical Implications & Risk
While many patients are asymptomatic, SCH is not benign. Key clinical implications encompass symptom burden, progression risk, and cardiovascular/metabolic associations.
Symptoms & Progression
Non-specific symptoms may include fatigue, cold intolerance, weight gain, constipation, and dry skin. Their correlation with TSH levels is poor. The annual risk of progression to overt hypothyroidism (low FT4) is approximately 2–5%, higher in those with positive anti-TPO antibodies and higher baseline TSH.
Cardiovascular & Metabolic Risk
Evidence links SCH, particularly with TSH >10 mIU/L, to:
- Dyslipidaemia: Elevated LDL cholesterol and total cholesterol.
- Atherosclerosis & CHD: Increased risk of coronary heart disease events and heart failure, especially in younger patients.
- Diastolic Hypertension.
- Non-alcoholic fatty liver disease (NAFLD).
Indications for Treatment
The decision to treat is individualised, weighing potential benefits against risks of over-treatment (e.g., atrial fibrillation, osteoporosis). Strong indications include:
For asymptomatic patients with TSH 5–10 mIU/L and low cardiovascular risk, active surveillance (TSH monitoring every 6–12 months) is a reasonable strategy.
Management & Monitoring
First-Line Therapy: Levothyroxine
Monitoring Protocol
Treatment Goal: Aim for TSH in the lower half of the reference range (approx. 0.5–2.5 mIU/L) in most adults. Avoid iatrogenic suppression (<0.5 mIU/L) due to risks of AF and osteoporosis.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Australian Institute of Health and Welfare (AIHW). Thyroid disease in Australia. Cat. no. PHE 243. Canberra: AIHW; 2020.
- 2. The Royal Australian College of General Practitioners (RACGP). Thyroid function tests – position statement. East Melbourne, Vic: RACGP; 2021.
- 3. Pearce SH, Brabant G, Duntas LH, et al. 2013 ETA Guideline: Management of Subclinical Hypothyroidism. Eur Thyroid J. 2013;2(4):215-228.
- 4. Lazarus J, Brown RS, Daumerie C, et al. 2014 European thyroid association guidelines for the management of subclinical hypothyroidism in pregnancy and in children. Eur Thyroid J. 2014;3(2):76-94.
- 5. National Health and Medical Research Council (NHMRC). Iodine supplementation for pregnant and breastfeeding women. NHMRC public statement. Canberra: NHMRC; 2010.
- 6. Biondi B, Cappola AR, Cooper DS. Subclinical Hypothyroidism: A Review. JAMA. 2019;322(2):153-160.
- 7. Chaker L, Bianco AC, Jonklaas J, Peeters RP. Hypothyroidism. Lancet. 2017;390(10101):1550-1562.
- 8. Australian Government Department of Health. The Australian Immunisation Handbook. (For vaccine considerations in autoimmune disease). Canberra.
- 9. The Endocrine Society of Australia (ESA). Position statement on the management of hypothyroidism. 2022.
- 10. Ngaosuwan K, Johnston DG, Godsland IF, et al. Increased Mortality in Subclinical Hypothyroidism: A Systematic Review and Meta-Analysis. J Clin Endocrinol Metab. 2021;106(11):e4607-e4617.