📋 Key Information Summary
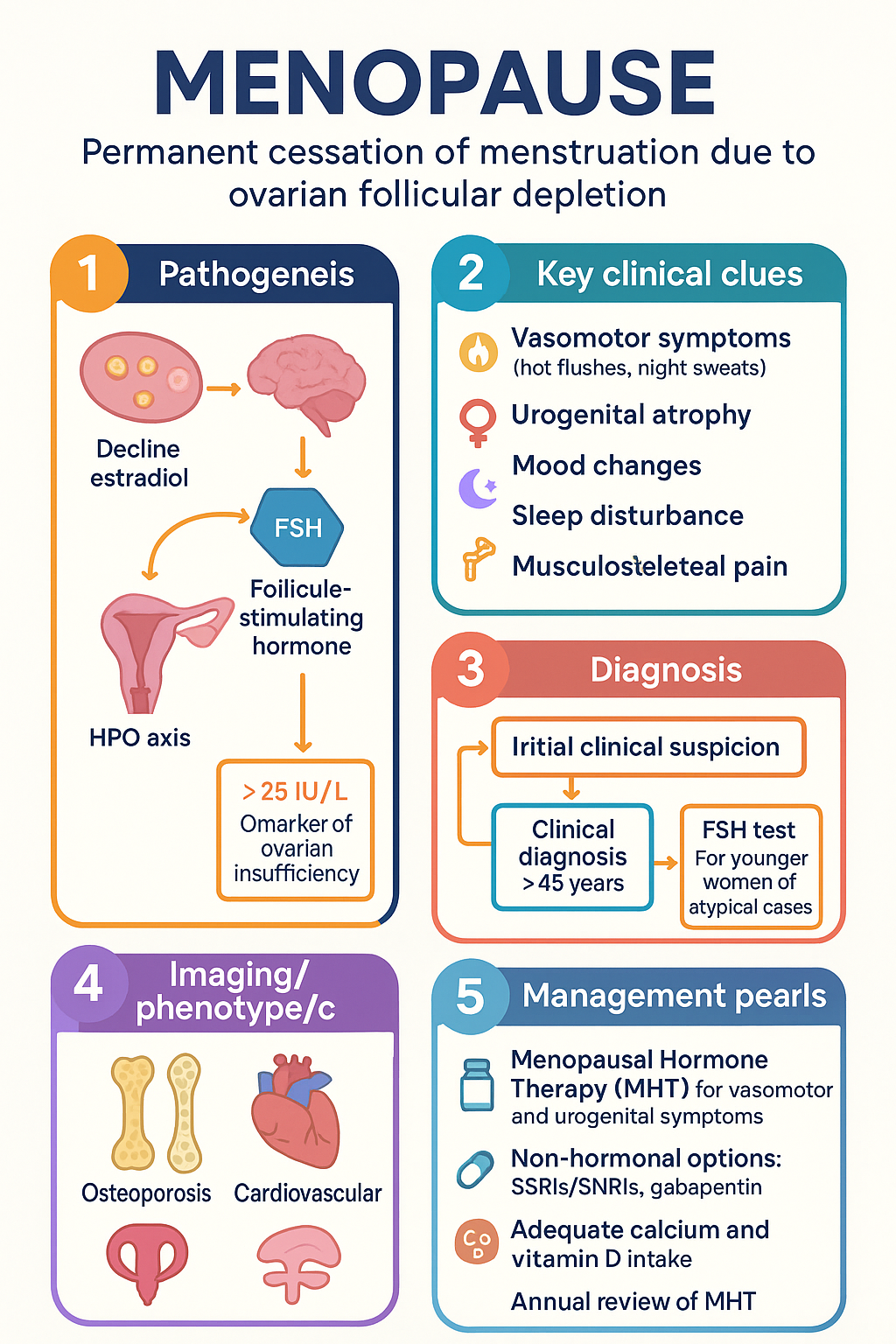
- Definition: Menopause is the permanent cessation of menstruation due to ovarian follicular depletion, confirmed retrospectively after 12 months of amenorrhoea.
- Stages: The menopausal transition (perimenopause) is characterised by irregular cycles and vasomotor symptoms, preceding the final menstrual period.
- Key Symptoms: Vasomotor symptoms (hot flushes, night sweats), urogenital atrophy, mood changes, sleep disturbance, and musculoskeletal pain are common.
- Long-term Risks: Oestrogen deficiency accelerates bone loss (osteoporosis) and is associated with an adverse cardiovascular risk profile.
- Diagnosis: Primarily clinical in women >45 years. Investigations (FSH) are reserved for younger women or atypical presentations.
- HRT First-line: Menopausal Hormone Therapy (MHT) is the most effective treatment for vasomotor and urogenital symptoms. Transdermal oestrogen is preferred for lower VTE risk.
- HRT Risks: Benefits generally outweigh risks for symptomatic women <60 years or within 10 years of menopause. Individual risk assessment for VTE, stroke, and breast cancer is mandatory.
- Non-hormonal Options: SSRIs/SNRIs (e.g., venlafaxine), gabapentin, and cognitive behavioural therapy are alternatives for VMS when MHT is contraindicated.
- Urogenital Syndrome: Vulvovaginal atrophy requires specific low-dose vaginal oestrogen therapy, which is safe and effective long-term.
- Bone Health: Baseline DEXA scan is recommended at menopause for women with risk factors. Adequate calcium and vitamin D intake are essential.
- Special Populations: Premature ovarian insufficiency (POI) requires hormone therapy until at least age 50. Management in ATSI women must be culturally safe and address access barriers.
- Review: MHT requires annual review of ongoing need, dose, and route, with consideration of discontinuation after 5 years unless symptoms persist.
🎧 Audio Brief
Introduction & Australian Epidemiology
Menopause is the permanent cessation of menstruation resulting from the loss of ovarian follicular activity. It is a physiological milestone defined retrospectively after 12 consecutive months of amenorrhoea in the absence of other pathological or physiological causes. The average age of natural menopause in Australia is 51-52 years.
The transition phase preceding menopause, known as perimenopause or the menopausal transition, can last for several years and is marked by irregular menstrual cycles and the onset of vasomotor symptoms (VMS). Approximately 80% of Australian women experience VMS, with 20-30% seeking medical treatment for moderate to severe symptoms. The demographic impact is substantial; with an ageing population, a significant proportion of the female population is either in the menopausal transition or post-menopausal.
The decline in oestradiol has widespread systemic effects, impacting cardiovascular, musculoskeletal, neurological, and urogenital health. Management aims to alleviate symptoms, improve quality of life, and mitigate long-term health risks, requiring an individualised approach based on symptom burden, personal preferences, and risk factor profile.
Physiology & Perimenopause
Menopause results from the exhaustion of the ovarian follicular pool. The reproductive years are characterised by cyclical follicular development, ovulation, and corpus luteum formation, driven by the hypothalamic-pituitary-ovarian (HPO) axis.
Stages of Reproductive Aging (STRAW+10 Criteria)
| Stage | Name | Key Characteristics |
|---|---|---|
| -5 to -3 | Reproductive | Regular menstrual cycles |
| -2 | Early Menopausal Transition | Persistent ≥7 day difference in cycle length |
| -1 | Late Menopausal Transition | ≥60 days of amenorrhoea; FSH rises |
| +1a to +1c | Postmenopause | Permanent amenorrhoea; oestradiol low |
During perimenopause, cycles become irregular due to fluctuating and often high oestradiol levels with low progesterone, creating a relatively hyper-oestrogenic, anovulatory state. This phase is associated with heavy menstrual bleeding in some women. Ultimately, oestradiol levels decline to a consistently low baseline.
Clinical Features & Complications
Vasomotor Symptoms (VMS)
Hot flushes and night sweats are the hallmark symptoms, affecting 75-80% of women. They are caused by dysfunction in the thermoregulatory nucleus of the hypothalamus due to oestrogen withdrawal.
Genitourinary Syndrome of Menopause (GSM)
Previously termed vulvovaginal atrophy, GSM encompasses vaginal dryness, irritation, dyspareunia, urinary urgency, and recurrent UTIs. It is progressive and does not spontaneously remit.
Long-Term Complications
Investigations
Diagnosis is clinical for women over 45 with typical symptoms and menstrual cycle changes. Investigations are not routinely required but can be useful in specific contexts.
Hormone Replacement Therapy (HRT) / Menopausal Hormone Therapy (MHT)
MHT remains the most effective treatment for vasomotor symptoms and urogenital atrophy. Therapy should be individualised, using the lowest effective dose for the shortest duration required, but with recognition that many women benefit from longer-term use for persistent symptoms and quality of life.
Systemic MHT for Vasomotor Symptoms
Non-Hormonal Prescribing for VMS
Local Oestrogen for GSM
Special Populations
📚 References
- 1. The Royal Australian College of General Practitioners (RACGP). Management of menopause. East Melbourne, Vic: RACGP; 2022.
- 2. Australasian Menopause Society (AMS). Menopause and midlife health: Information for women. 2023. Available from: [https://www.menopause.org.au].
- 3. Harlow SD, Gass M, Hall JE, et al. Executive summary of the Stages of Reproductive Aging Workshop + 10: addressing the unfinished agenda of staging reproductive aging. J Clin Endocrinol Metab. 2012;97(4):1159-68.
- 4. Lethaby A, Marjoribanks J, Kronenberg F, Roberts H, Eden J, Brown J. Phytoestrogens for menopausal vasomotor symptoms. Cochrane Database Syst Rev. 2013;(12):CD001395.
- 5. The North American Menopause Society (NAMS). The 2022 hormone therapy position statement of The North American Menopause Society. Menopause. 2022;29(7):767-794.
- 6. Baber RJ, Panay N, Fenton A; IMS Writing Group. 2016 IMS Recommendations on women's midlife health and menopause hormone therapy. Climacteric. 2016;19(2):109-50.
- 7. Australian Institute of Health and Welfare (AIHW). Menopause in Australia. Canberra: AIHW; 2023.
- 8. Marjoribanks J, Farquhar C, Roberts H, Lethaby A, Lee J. Long-term hormone therapy for perimenopausal and postmenopausal women. Cochrane Database Syst Rev. 2017;1(1):CD004143.
- 9. Sturdee DW, Panay N; International Menopause Society Writing Group. Recommendations for the management of postmenopausal vaginal atrophy. Climacteric. 2010;13(6):509-22.
- 10. The Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG). Management of the menopause. C-Obs 47. 2020.
- 11. National Aboriginal Community Controlled Health Organisation (NACCHO). Position statement: Aboriginal and Torres Strait Islander health. 2023.
- 12. The Australian Menopause Society (AMS). Consensus statement: The role of MHT in the management of menopause. 2024.