📋 Key Information Summary
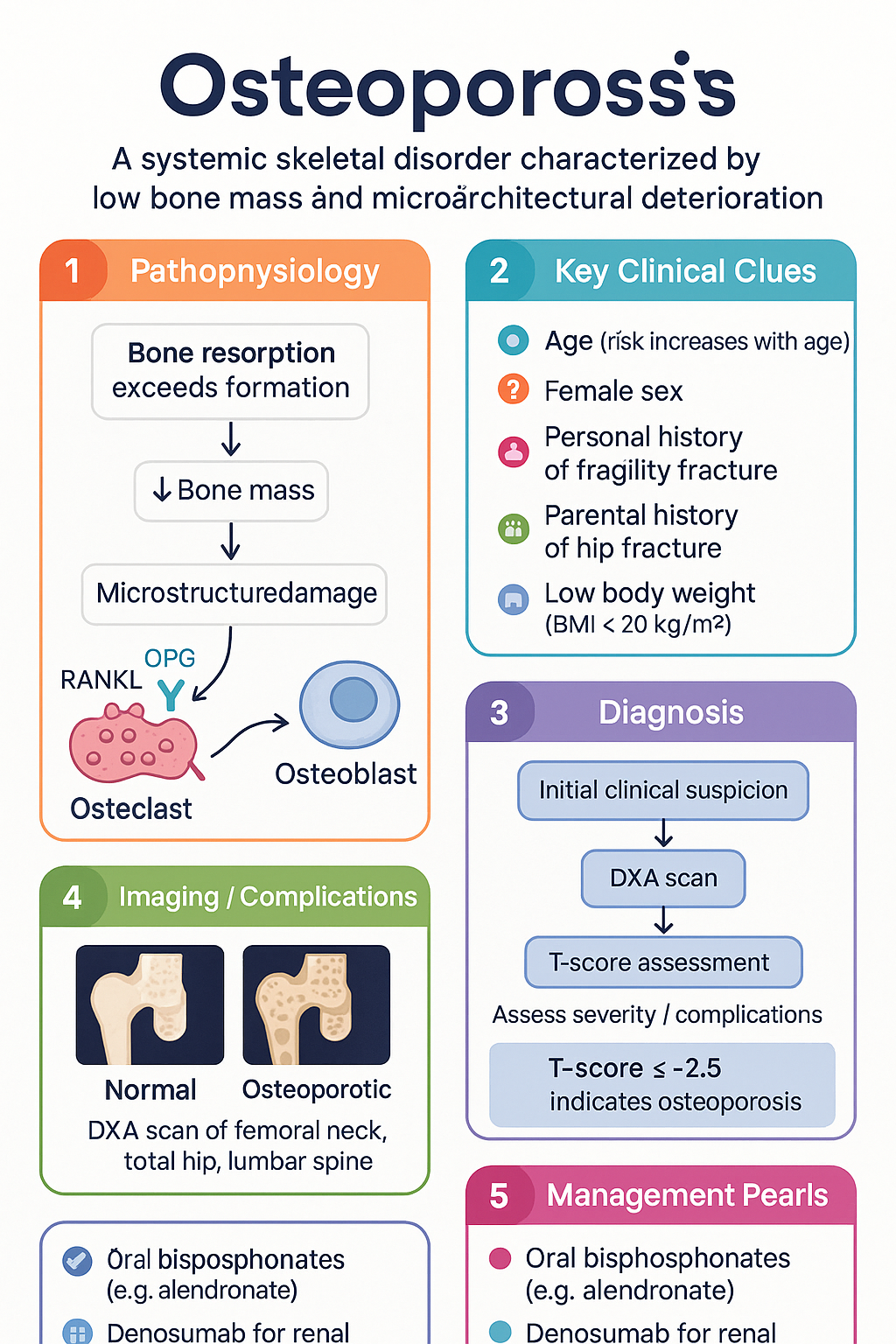
- Osteoporosis is defined by a bone mineral density (BMD) T-score ≤ −2.5 at the femoral neck, total hip, or lumbar spine on DXA scan.
- Fracture risk is assessed using the FRAX® tool, integrating clinical risk factors and BMD to guide treatment thresholds.
- First-line pharmacotherapy for most patients is an oral bisphosphonate (e.g., alendronate or risedronate).
- Denosumab is a first-line alternative, particularly for those with renal impairment or intolerance to oral bisphosphonates.
- Teriparatide is reserved for severe osteoporosis (e.g., very low T-scores, multiple fractures, or glucocorticoid-induced).
- Adequate calcium (≥1300 mg/day) and vitamin D (supplementation if deficient) are foundational for all patients.
- Weight-bearing and resistance exercise is a critical non-pharmacological intervention to reduce fall and fracture risk.
- Secondary causes (e.g., hyperparathyroidism, coeliac disease, chronic corticosteroids) must be actively excluded.
- Monitoring of treatment response is via serial DXA scans every 1–2 years and bone turnover markers.
- Osteoporosis management must consider Aboriginal and Torres Strait Islander peoples, who have higher fracture rates and barriers to care.
🎧 Audio Brief
Introduction & Australian Epidemiology
Osteoporosis is a systemic skeletal disorder characterised by low bone mass and microarchitectural deterioration of bone tissue, leading to enhanced bone fragility and a consequent increase in fracture risk. It represents a major public health issue in Australia.
In Australia, approximately 4.74 million people aged over 50 have osteoporosis or osteopenia. The condition is responsible for an estimated 172,000+ fractures each year, with significant associated morbidity, mortality, and healthcare costs. The risk of fragility fracture increases with age, and the burden falls disproportionately on women (approximately 75% of fractures), although men also account for a substantial proportion.
Hip fractures are particularly devastating, carrying a 1-year mortality rate of 20-30%. The direct medical costs of osteoporosis and related fractures in Australia are estimated at over $3.1 billion annually.
Epidemiology & Risk Factors (FRAX Score)
A fragility fracture is a fracture resulting from mechanical forces that would not ordinarily cause a fracture, typically a fall from a standing height or less.
Key Non-Modifiable Risk Factors
- Age (risk increases exponentially with age)
- Female sex
- Personal history of fragility fracture (strongest predictor of future fracture)
- Parental history of hip fracture
- Low body weight (BMI < 20 kg/m²)
Key Modifiable Risk Factors
- Current smoking
- Excess alcohol intake (> 3 standard drinks/day)
- Glucocorticoid therapy (≥ 7.5 mg prednisolone equivalent/day for ≥ 3 months)
- Vitamin D deficiency
- Conditions leading to secondary osteoporosis
FRAX® Tool
The WHO Fracture Risk Assessment Tool (FRAX®) estimates the 10-year probability of a major osteoporotic fracture (hip, spine, forearm, humerus) and hip fracture alone. It incorporates clinical risk factors with or without a BMD T-score.
Pathophysiology & Secondary Causes
Bone is in a constant state of remodelling, with osteoclasts resorbing old bone and osteoblasts forming new bone. Osteoporosis arises when bone resorption exceeds formation, leading to a net loss of bone mass and strength.
Common Secondary Causes in Australia
It is estimated that up to 30% of postmenopausal women and 50% of men with osteoporosis have an underlying secondary cause. These must be actively investigated.
| Category | Specific Conditions / Agents |
|---|---|
| Endocrine | Primary hyperparathyroidism, hyperthyroidism, Cushing's syndrome, hypogonadism, type 1 diabetes |
| Gastrointestinal | Coeliac disease, inflammatory bowel disease, chronic liver disease, malabsorption |
| Rheumatological | Rheumatoid arthritis, ankylosing spondylitis |
| Medications | Glucocorticoids, aromatase inhibitors (e.g., anastrozole), androgen deprivation therapy, some anticonvulsants, proton pump inhibitors (long-term) |
| Other | Chronic kidney disease (stage 4+), multiple myeloma, organ transplant, vitamin D deficiency |
Investigations (DEXA Scan, T-Score)
Bone Densitometry (DXA Scan)
Central Dual-Energy X-ray Absorptiometry (DXA) of the hip (femoral neck and total hip) and lumbar spine (L1–L4) is the gold standard for diagnosing osteoporosis. It is a safe, quick, and low-radiation scan.
Diagnostic Criteria (WHO)
- Normal: T-score ≥ −1.0
- Osteopenia (Low bone mass): T-score between −1.0 and −2.5
- Osteoporosis: T-score ≤ −2.5
- Severe Osteoporosis: T-score ≤ −2.5 with one or more fragility fractures.
Baseline & Screening Investigations
To exclude secondary causes and establish baseline parameters for monitoring.
Management
Non-Pharmacological Management
- Calcium: Aim for a total dietary + supplement intake of ≥ 1300 mg/day. Use supplements if intake is inadequate.
- Vitamin D: Supplement with cholecalciferol (e.g., 1000–2000 IU daily, or higher loading doses if deficient) to maintain a serum 25(OH)D level ≥ 50 nmol/L.
- Exercise: Weight-bearing (e.g., brisk walking, dancing) and resistance/strength training at least 3 times per week.
- Fall prevention: Home hazard assessment, balance training (e.g., Tai Chi), vision correction, medication review.
- Lifestyle: Smoking cessation, limit alcohol to ≤ 2 standard drinks/day.
Pharmacological Management — First-Line Therapies
Pharmacological Management — Second-Line & Severe Osteoporosis
Monitoring Therapy
- Bone Density (DXA): Repeat scan 1–2 years after initiating therapy, then every 2–3 years if stable. Assess for significant decline (least significant change ~4%).
- Bone Turnover Markers (BTMs): P1NP (formation) and CTX (resorption) can help assess adherence and response. Check at baseline and 3–6 months after starting treatment.
- Clinical Review: Monitor for new fractures, falls, medication side effects (e.g., GI for bisphosphonates), and adherence.
Special Populations
Aboriginal and Torres Strait Islander peoples experience a higher burden of osteoporosis and fragility fractures at a younger age compared to non-Indigenous Australians, linked to earlier onset of chronic disease comorbidities and socioeconomic factors.
📚 References
- 1. The Royal Australian College of General Practitioners (RACGP). Clinical guideline for the diagnosis and management of osteoporosis in postmenopausal women and men. 2017.
- 2. Australian Institute of Health and Welfare (AIHW). Osteoporosis. Cat. no. PHE 236. Canberra: AIHW; 2020.
- 3. Endocrine Society of Australia and Osteoporosis Australia. Position statement on the management of osteoporosis. 2020.
- 4. Kanis JA, et al. European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int. 2019;30(1):3-44.
- 5. Australian Government Department of Health. Pharmaceutical Benefits Scheme (PBS). Alendronate, Denosumab, Teriparatide. Available at pbs.gov.au. Accessed 2024.
- 6. Osteoporosis Australia. Calcium and Vitamin D in Osteoporosis. Consumer information. 2021.
- 7. National Health and Medical Research Council (NHMRC). Australian Guidelines to Reduce Health Risks from Drinking Alcohol. Canberra: NHMRC; 2020.
- 8. Sherrington C, et al. Effective exercise for the prevention of falls: a systematic review and meta-analysis. J Am Geriatr Soc. 2019;67(12):2505-2514.
- 9. Cummings SR, et al. Denosumab for treatment of postmenopausal osteoporosis: results of a randomized trial. J Bone Miner Res. 2009;24(2):293-310.
- 10. Neubauer L, et al. Fracture risk in Aboriginal and non-Aboriginal populations in New South Wales. Aust N Z J Public Health. 2019;43(5):457-463.