📋 Key Information Summary
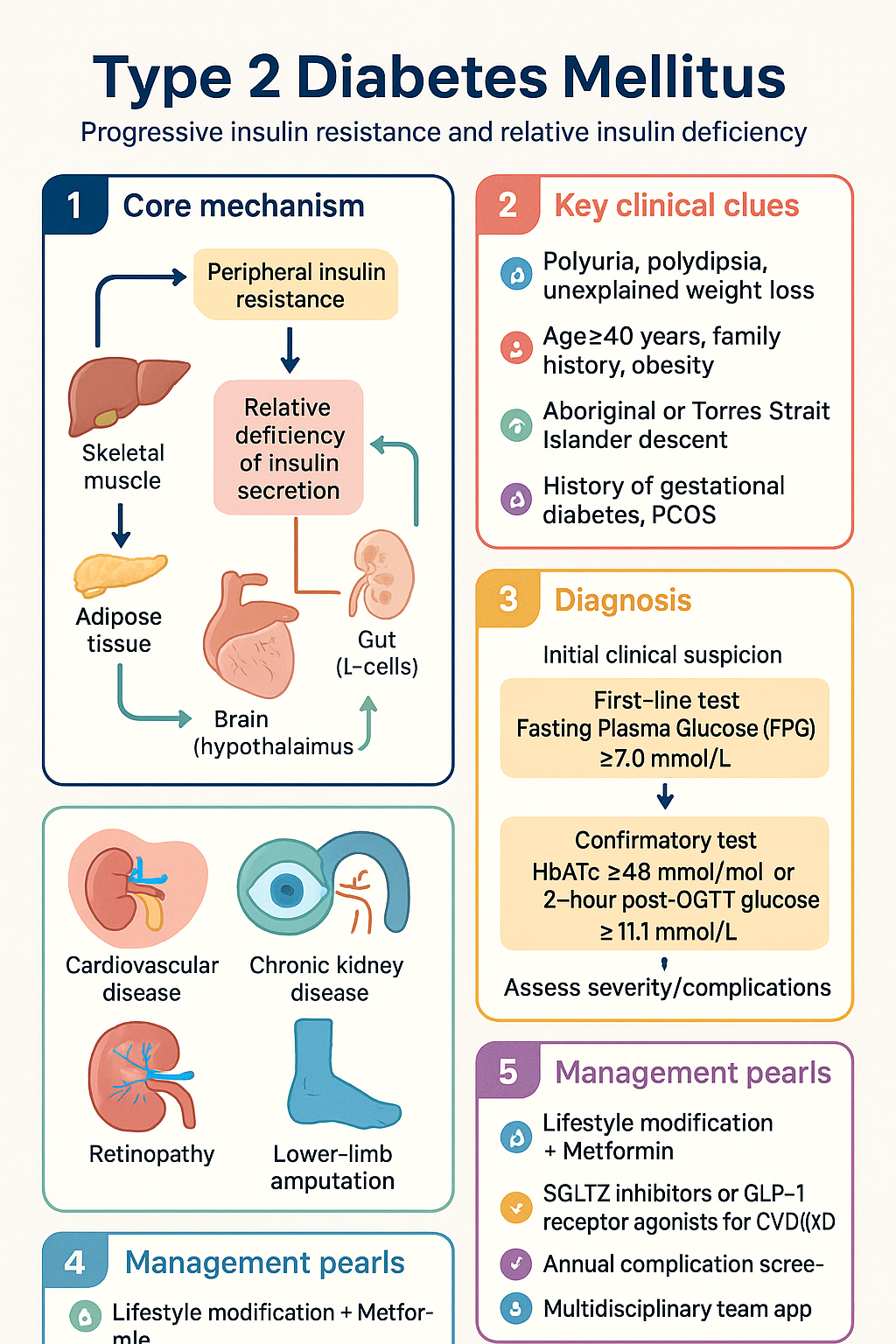
- Type 2 diabetes mellitus (T2DM) is characterised by progressive insulin resistance and relative insulin deficiency, accounting for approximately 85–90% of all diabetes in Australia.
- An estimated 1.3 million Australians live with T2DM; prevalence in Aboriginal and Torres Strait Islander peoples is approximately 2–4 times higher than in non-Indigenous Australians.
- Diagnosis requires a fasting plasma glucose (FPG) ≥7.0 mmol/L, HbA1c ≥6.5% (48 mmol/mol), or a 2-hour post-OGTT glucose ≥11.1 mmol/L, confirmed on two separate occasions (or a single test with symptoms).
- Screening is recommended every 3 years from age 40 (or 18 for high-risk groups including ATSI peoples, those with gestational diabetes history, or PCOS).
- Stepwise pharmacological management begins with metformin as first-line; SGLT2 inhibitors or GLP-1 receptor agonists are prioritised early in patients with established cardiovascular disease, heart failure, or CKD.
- HbA1c target is generally ≤53 mmol/mol (7.0%); individualise to ≤48 mmol/mol (6.5%) in younger patients with short disease duration and no hypoglycaemia risk, or relax to ≤64 mmol/mol (8.0%) in frailty or limited life expectancy.
- Annual comprehensive complication screening includes urine ACR, eGFR, retinopathy screening, foot assessment, and cardiovascular risk evaluation.
- SGLT2 inhibitors (empagliflozin, dapagliflozin) and GLP-1 RAs (semaglutide, liraglutide) have demonstrated cardiovascular and renal benefits independent of glycaemic control.
- Insulin therapy should be considered when HbA1c remains above target despite dual or triple oral/injectable therapy; basal insulin is the preferred starting regimen.
- Management of T2DM requires a multidisciplinary team approach including GP, endocrinologist, diabetes educator, dietitian, podiatrist, ophthalmologist, and psychologist.
- Weight management of ≥5–10% body weight significantly improves glycaemic control, blood pressure, and cardiovascular risk.
- Bariatric/metabolic surgery should be considered in adults with BMI ≥40 kg/m² (or ≥35 kg/m² with poorly controlled T2DM) when lifestyle and pharmacotherapy are insufficient.
🎧 Audio Brief
Introduction & Australian Epidemiology
Type 2 diabetes mellitus (T2DM) is a chronic, progressive metabolic disorder characterised by peripheral insulin resistance and a relative deficiency of insulin secretion from pancreatic beta cells. It is the most prevalent form of diabetes, accounting for approximately 85–90% of all diagnosed diabetes in Australia, and is strongly associated with obesity, metabolic syndrome, and sedentary lifestyle.
In Australia, an estimated 1.3 million people were living with T2DM in 2023, with prevalence continuing to rise due to ageing populations, increasing obesity rates, and improved case detection. T2DM is the seventh leading cause of death in Australia and a major contributor to cardiovascular disease, chronic kidney disease, lower-limb amputation, and preventable blindness.
The disease burden is not evenly distributed. Aboriginal and Torres Strait Islander peoples experience T2DM prevalence approximately 2–4 times greater than non-Indigenous Australians, with earlier onset, more aggressive complications, and higher mortality. Socioeconomic disadvantage, remote geography, and barriers to healthcare access compound these disparities.
The total direct cost of diabetes to the Australian healthcare system exceeds $6 billion annually, encompassing hospitalisations, medications (including PBS-listed agents and continuous glucose monitoring), allied health services, and management of complications.
Pathophysiology & Risk Factors
The pathogenesis of T2DM is multifactorial and involves the interplay of genetic susceptibility, environmental factors, and behavioural determinants. The "ominous octet" framework describes eight key pathophysiological mechanisms contributing to hyperglycaemia.
Core Pathophysiological Mechanisms
| Mechanism | Site | Clinical Consequence |
|---|---|---|
| Decreased insulin secretion | Pancreatic β-cells | Progressive β-cell failure; ~50% function lost at diagnosis |
| Increased hepatic glucose production | Liver | Fasting hyperglycaemia due to gluconeogenesis and glycogenolysis |
| Peripheral insulin resistance | Skeletal muscle, adipose tissue | Impaired glucose uptake; compensatory hyperinsulinaemia |
| Incretin defect | Gut (L-cells) | Reduced GLP-1 effect; impaired postprandial insulin release |
| Increased glucagon secretion | Pancreatic α-cells | Paradoxical hepatic glucose output postprandially |
| Increased renal glucose reabsorption | Kidney (SGLT2) | Raised renal threshold for glycosuria |
| Neurotransmitter dysfunction | Brain (hypothalamus) | Impaired appetite regulation and satiety signalling |
| Adipose tissue inflammation | Visceral fat | Chronic low-grade inflammation; lipotoxicity |
Risk Factors for T2DM
Risk factors can be categorised as non-modifiable and modifiable. The Australian Type 2 Diabetes Risk Assessment Tool (AUSDRISK) is a validated 10-item questionnaire used for population-level screening.
- Age ≥40 years (risk increases with age)
- Family history of T2DM (first-degree relative)
- Aboriginal or Torres Strait Islander descent
- History of gestational diabetes mellitus (GDM)
- Polycystic ovary syndrome (PCOS)
- Certain ethnic backgrounds (South Asian, Pacific Islander, Māori, Middle Eastern)
- Overweight/obesity (BMI ≥25 kg/m² or ≥23 kg/m² in Asian populations)
- Central adiposity (waist circumference >94 cm men, >80 cm women)
- Physical inactivity (<150 min moderate-intensity per week)
- Unhealthy dietary patterns (high glycaemic index, ultra-processed foods)
- Smoking
- Impaired fasting glucose (IFG) or impaired glucose tolerance (IGT)
- Hypertension, dyslipidaemia, obstructive sleep apnoea
- Medications: corticosteroids, atypical antipsychotics, thiazides, statins
Diagnosis & Screening
Diagnostic Criteria
The diagnosis of T2DM is based on either symptoms of hyperglycaemia (polyuria, polydipsia, unexplained weight loss) combined with a random plasma glucose ≥11.1 mmol/L, or asymptomatic hyperglycaemia confirmed on two separate occasions. The following tests are accepted for diagnosis:
| Test | Diabetes | Pre-diabetes | Normal |
|---|---|---|---|
| Fasting plasma glucose (FPG) | ≥7.0 mmol/L | 6.1–6.9 mmol/L | <6.1 mmol/L |
| 2-hour post-OGTT glucose | ≥11.1 mmol/L | 7.8–11.0 mmol/L | <7.8 mmol/L |
| HbA1c (IFCC) | ≥48 mmol/mol (6.5%) | 42–47 mmol/mol (6.0–6.4%) | <42 mmol/mol (<6.0%) |
| Random plasma glucose | ≥11.1 mmol/L (with symptoms) | — | — |
Screening Recommendations
The Royal Australian College of General Practitioners (RACGP) and the Australian Diabetes Society (ADS) recommend opportunistic screening using FPG or HbA1c for the following groups:
Pharmacological Management (Stepwise)
Pharmacotherapy for T2DM follows a stepwise approach aligned with the ADA/EASD consensus, RACGP guidelines, and Australian PBS availability. Lifestyle modification remains the foundation at every step. Agents are selected based on glycaemic efficacy, cardiovascular and renal benefit, hypoglycaemia risk, effect on weight, cost, and patient preference.
Step 1 — Lifestyle Modification + Metformin
Metformin remains the first-line pharmacological agent for T2DM unless contraindicated (eGFR <30 mL/min) or not tolerated.
Step 2 — Dual Therapy
If HbA1c remains above target after 3–6 months on metformin, add a second agent. Choice is guided by comorbidities:
Second-Line Agents
Step 3 — Triple Therapy
If dual therapy does not achieve target HbA1c after 3–6 months, a third agent from a complementary class is added. Common combinations include metformin + SGLT2i + GLP-1 RA, or metformin + SGLT2i + DPP-4i (note: do not combine GLP-1 RA with DPP-4i).
Step 4 — Insulin Therapy
Insulin should be initiated when HbA1c remains above target despite optimised oral/injectable therapy, or when HbA1c is >86 mmol/mol (10%) at presentation. Basal insulin is the preferred starting regimen.
Step 5 — Intensified Insulin Regimens
If basal insulin + oral agents fail to achieve target, consider basal-bolus insulin (adding rapid-acting insulin before meals) or a premixed insulin regimen. Continuous subcutaneous insulin infusion (CSII / insulin pump) is rarely indicated in T2DM but may be considered in select patients with persistent hyperglycaemia despite multiple daily injections.
Additional Agent Considerations
Complications & Glycaemic Targets
Glycaemic Targets
Glycaemic targets should be individualised based on patient age, duration of diabetes, life expectancy, hypoglycaemia risk, comorbidities, and patient preference. HbA1c is the primary monitoring metric.
Microvascular Complications
| Complication | Screening | Key Management |
|---|---|---|
| Diabetic retinopathy | Annual fundal photography from diagnosis (2-yearly if low risk). MBS item 10953. | Optimise HbA1c, BP, lipids. Intravitreal anti-VEGF (ranibizumab, aflibercept) for proliferative/DME. Refer ophthalmology. |
| Diabetic nephropathy | Annual urine ACR + eGFR from diagnosis. Repeat abnormal results within 3 months. | ACEi or ARB for albuminuria. SGLT2i (eGFR ≥20). Finerenone for CKD with albuminuria. BP target <130/80 mmHg. |
| Diabetic neuropathy | Annual 10 g monofilament + 128 Hz tuning fork assessment. | Painful neuropathy: pregabalin, duloxetine, or amitriptyline. Gabapentin as alternative. Foot ulcer prevention. |
Macrovascular Risk Management
Cardiovascular disease is the leading cause of death in people with T2DM. Comprehensive cardiovascular risk reduction requires a multifactorial approach:
Diabetic Foot Disease
Annual Review Checklist
| Component | Assessment | Frequency |
|---|---|---|
| HbA1c | Glycaemic control | 3–6 monthly |
| Blood pressure | Target <130/80 mmHg | Every visit |
| Lipid profile | LDL target per CV risk | Annual |
| Urine ACR + eGFR | Renal function / albuminuria | Annual |
| Retinal screening | Diabetic retinopathy | Annual |
| Foot examination | Monofilament + pulse + visual | Annual (high risk: every visit) |
| Weight / BMI / waist | Obesity management | Every visit |
| Depression screening | PHQ-9 or K10 | Annual |
| CVD risk assessment | Australian absolute CVD risk calculator | Every 2 years (or as needed) |
| Immunisation review | Influenza (annual), pneumococcal, COVID-19, hepatitis B | Annual review |
Special Populations
Pregnancy
Paediatrics
Elderly / Frail
Chronic Kidney Disease
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Royal Australian College of General Practitioners. General practice management of type 2 diabetes: 2024–2025. East Melbourne: RACGP; 2024.
- 2. American Diabetes Association Professional Practice Committee. Standards of Care in Diabetes — 2024. Diabetes Care. 2024;47(Suppl 1):S1–S321.
- 3. Davies MJ, Aroda VR, Collins BS, et al. Management of hyperglycaemia in type 2 diabetes, 2022: a consensus report by the ADA and EASD. Diabetologia. 2022;65(12):1925–1966.
- 4. Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes (EMPA-REG OUTCOME). N Engl J Med. 2015;373(22):2117–2128.
- 5. Heerspink HJL, Stefánsson BV, Correa-Rotter R, et al. Dapagliflozin in patients with chronic kidney disease (DAPA-CKD). N Engl J Med. 2020;383(15):1436–1446.
- 6. Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes (SUSTAIN-6). N Engl J Med. 2016;375(19):1834–1844.
- 7. Bakris GL, Agarwal R, Anker SD, et al. Effect of finerenone on chronic kidney disease outcomes in type 2 diabetes (FIDELIO-DKD). N Engl J Med. 2020;383(23):2219–2229.
- 8. Australian Institute of Health and Welfare. Diabetes: Australian facts. Canberra: AIHW; 2023. Cat. no. CVD 82.
- 9. Department of Health and Aged Care. National Diabetes Strategy 2021–2030. Canberra: Australian Government; 2021.
- 10. Wabe NT, Thomas J, Seo D, et al. Type 2 diabetes prevalence and management in Aboriginal and Torres Strait Islander peoples: a systematic review and meta-analysis. Diabetes Res Clin Pract. 2023;203:110866.
- 11. Australian Commission on Safety and Quality in Health Care. National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.
- 12. Lipscombe L, Butalia S, Dasgupta K, et al. Pharmacologic glycemic management of type 2 diabetes in adults: 2023 update. Can J Diabetes. 2023;47(7):558–576.