📋 Key Information Summary
- Primary hyperaldosteronism (PHA) is the most common cause of secondary hypertension, affecting 5–13% of all hypertensive patients and up to 20% with resistant hypertension.
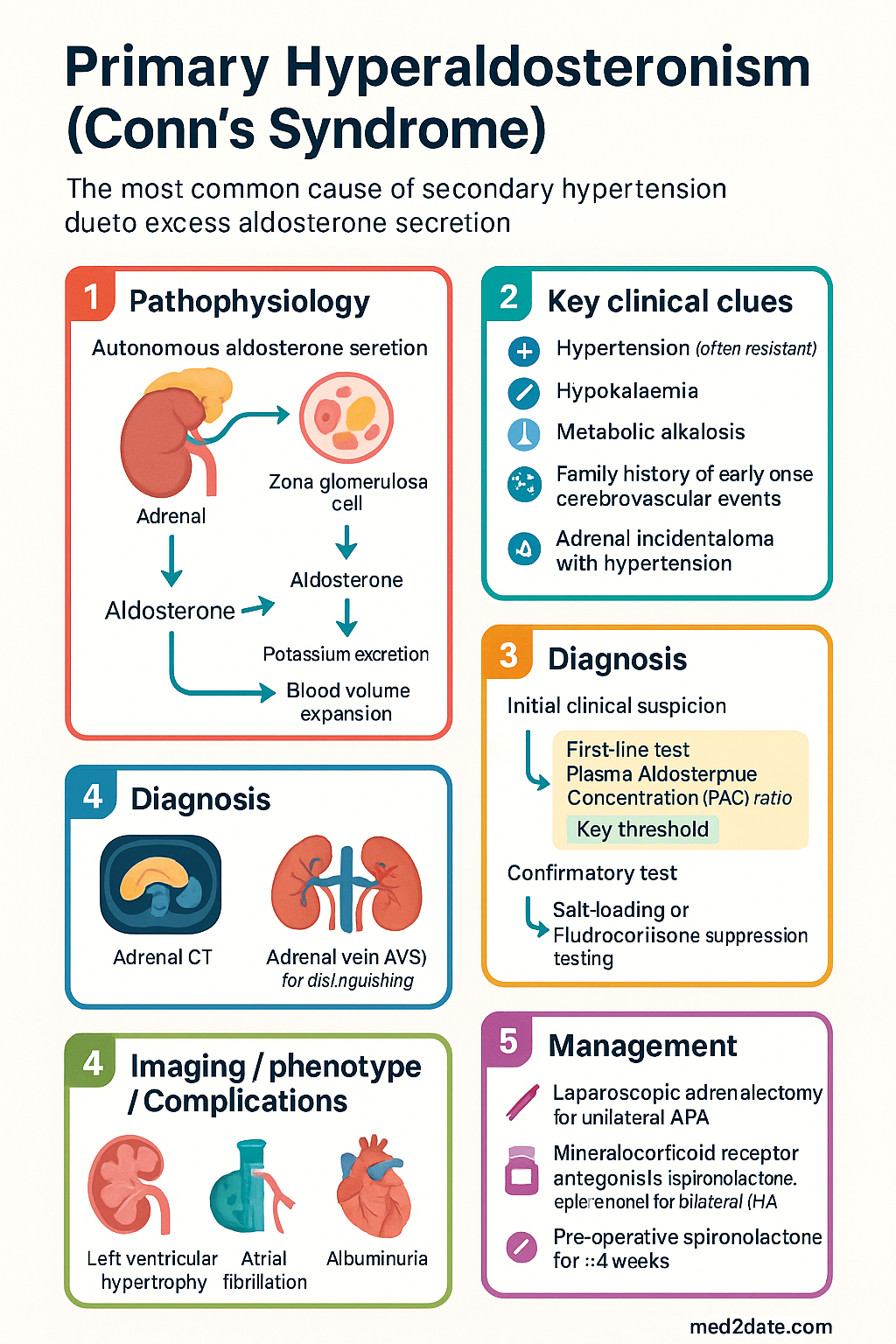
- PHA results from autonomous aldosterone secretion from an aldosterone-producing adenoma (APA) or bilateral idiopathic adrenal hyperplasia (IHA), with excess aldosterone causing sodium retention, potassium wasting, and renin suppression.
- Screening is indicated in all patients with resistant hypertension (≥3 antihypertensives), hypertension with spontaneous or diuretic-induced hypokalaemia, adrenal incidentaloma with hypertension, onset of hypertension before age 20, or hypertension with a family history of early-onset cerebrovascular events.
- The screening test of choice is the plasma aldosterone concentration (PAC) to plasma renin activity (PRA) ratio, performed in the morning after the patient has been ambulant for at least 2 hours, off interfering medications where possible for ≥4 weeks.
- A screening ARR ≥750 pmol/L per ng/mL/h (with PAC ≥415 pmol/L) is considered positive; confirmatory salt-loading or fludrocortisone suppression testing is then required.
- Confirmatory testing mandates a 4-day oral salt-loading protocol (slow-release NaCl 300 mmol/day with KCl supplementation) followed by 24-hour urine aldosterone collection — values >33 nmol/24 h confirm autonomous secretion.
- Adrenal CT is the initial localisation study but has poor sensitivity for micro-adenomas; adrenal vein sampling (AVS) by an experienced interventional radiologist is the gold standard for distinguishing unilateral APA from bilateral IHA.
- Unilateral APA is treated with laparoscopic adrenalectomy, which can cure or significantly improve hypertension in 50–80% of cases and resolve hypokalaemia in >90%.
- Bilateral IHA and patients unsuitable for surgery are managed medically with mineralocorticoid receptor antagonists — spironolactone (first-line) or eplerenone (fewer anti-androgenic side effects), titrated to blood pressure and potassium targets.
- Peri-operative management requires spironolactone pre-operatively for ≥4 weeks to normalise potassium and reduce operative risk; post-operative monitoring for hypoaldosteronism and hypotension is essential.
- PHA confers excess cardiovascular risk independent of blood pressure, including left ventricular hypertrophy, atrial fibrillation, albuminuria, and metabolic syndrome — early identification and treatment reduces long-term morbidity.
- Aboriginal and Torres Strait Islander peoples experience higher rates of resistant hypertension and cardiovascular disease; screening for PHA should have a lower threshold in this population.
🎧 Audio Brief
Introduction & Australian Epidemiology
Primary hyperaldosteronism (PHA), historically termed Conn's syndrome, is characterised by autonomous overproduction of aldosterone from the adrenal cortex, independent of the renin–angiotensin–aldosterone system (RAAS). The resultant aldosterone excess drives sodium and water retention, potassium excretion, and renin suppression, producing a clinical phenotype of hypertension (often resistant), hypokalaemia, and metabolic alkalosis.
Previously considered rare, PHA is now recognised as the most common specific cause of secondary hypertension. Prevalence estimates vary by population studied: 5–13% in general hypertension clinics, up to 20% in resistant hypertension, and 25–30% in patients with spontaneous hypokalaemia and hypertension. In Australia, with approximately 6 million adults affected by hypertension, the estimated burden of undiagnosed PHA is substantial — potentially 300,000–780,000 individuals.
The two principal subtypes are aldosterone-producing adenoma (APA, 30–40% of PHA) and bilateral idiopathic adrenal hyperplasia (IHA, 60–70%). Rare causes include familial hyperaldosteronism (FH types I–III), unilateral adrenal hyperplasia, and aldosterone-producing adrenocortical carcinoma. PHA affects all age groups, peaks in the 3rd–5th decades for APA and 5th–6th decades for IHA, and is more common in females for APA.
Undiagnosed PHA carries significant morbidity. Compared with patients who have essential hypertension at equivalent blood pressure levels, PHA patients have a 4-fold higher risk of atrial fibrillation, 6-fold higher risk of heart failure, and increased rates of left ventricular hypertrophy, stroke, coronary artery disease, metabolic syndrome, and albuminuria. Early detection and appropriate management are therefore critical to reducing long-term cardiovascular outcomes.
Pathophysiology & Causes
Normal Aldosterone Physiology
Aldosterone is synthesised in the zona glomerulosa of the adrenal cortex under the primary control of angiotensin II, serum potassium, and, to a lesser extent, ACTH. Angiotensin II acts via AT1 receptors on zona glomerulosa cells to stimulate aldosterone synthase (CYP11B2) and aldosterone production. Aldosterone then acts on the mineralocorticoid receptor (MR) in the distal nephron and collecting duct, upregulating epithelial sodium channels (ENaC) and Na⁺/K⁺-ATPase, promoting sodium reabsorption and potassium secretion.
Mechanisms of Autonomous Aldosterone Secretion
In PHA, aldosterone production escapes normal physiological regulation. The principal pathological mechanisms are:
| Subtype | Proportion | Mechanism | Key Features |
|---|---|---|---|
| Aldosterone-producing adenoma (APA) | 30–40% | Somatic mutations in KCNJ5, ATP1A1, ATP2B3, CACNA1D, or CTNNB1 genes; autonomous aldosterone secretion from a single adenoma | Younger patients, higher aldosterone levels, more likely hypokalaemic, curable by adrenalectomy |
| Bilateral idiopathic adrenal hyperplasia (IHA) | 60–70% | Diffuse or nodular hyperplasia of both adrenal glands; enhanced sensitivity to angiotensin II and other secretagogues | Older patients, milder biochemical phenotype, typically normokalaemic, medical management |
| Primary unilateral adrenal hyperplasia (UAH) | <2% | Nodular hyperplasia confined to one adrenal gland; functionally equivalent to APA | May be missed on CT; diagnosed by AVS |
| Familial hyperaldosteronism type I (FH-I / GRA) | <1% | Chimeric CYP11B1/CYP11B2 gene duplication; aldosterone regulated by ACTH instead of angiotensin II | Autosomal dominant, onset typically <20 years, suppressible with low-dose dexamethasone |
| Familial hyperaldosteronism type II | <5% | Linked to chromosome 7p22; can present as APA or IHA | Not dexamethasone-suppressible; familial clustering without chimeric gene |
| Familial hyperaldosteronism type III | Rare | Germline KCNJ5 mutations; severe bilateral adrenal hyperplasia with massive aldosterone excess | Childhood onset, may require bilateral adrenalectomy |
| Aldosterone-producing adrenocortical carcinoma | <1% | Malignant adrenal tumour with autonomous aldosterone and often cortisol or androgen co-secretion | Rapid onset, very high aldosterone, large (>4 cm) adrenal mass |
Downstream Pathological Effects
Excess aldosterone exerts deleterious effects through both genomic and non-genomic pathways:
- Mineralocorticoid receptor activation: Upregulation of ENaC and Na⁺/K⁺-ATPase in the distal nephron → sodium retention, volume expansion, hypertension, and hypokalaemia.
- Cardiac fibrosis: Direct MR activation in cardiomyocytes and fibroblasts promotes collagen deposition, left ventricular hypertrophy (LVH), and diastolic dysfunction independent of blood pressure.
- Vascular inflammation and endothelial dysfunction: Aldosterone increases reactive oxygen species (ROS) generation via NADPH oxidase, promoting vascular inflammation and impaired nitric oxide (NO) bioavailability.
- Metabolic effects: Aldosterone impairs insulin signalling through MR-mediated oxidative stress in adipose tissue and skeletal muscle, contributing to insulin resistance and metabolic syndrome.
- Renal injury: Glomerular hyperfiltration, podocyte injury, and tubulointerstitial fibrosis contribute to albuminuria and progressive renal impairment.
- Atrial fibrillation: Aldosterone-driven atrial fibrosis, electrical remodelling, and inflammation significantly increase AF risk — approximately 4-fold compared with essential hypertension.
Medication-Related Aldosterone Excess
Certain medications can exacerbate or unmask PHA. Liddle syndrome (gain-of-function ENaC mutation) and apparent mineralocorticoid excess (AME, 11β-HSD2 deficiency) are important differential diagnoses. Liquorice, carbenoxolone, and glycyrrhizic acid inhibit 11β-HSD2, causing pseudo-hyperaldosteronism with suppressed renin and aldosterone.
Clinical Features & Screening
Clinical Presentation
PHA most commonly presents with hypertension detected incidentally or during investigation for resistant or early-onset hypertension. The classic triad of hypertension, hypokalaemia, and metabolic alkalosis is present in fewer than 50% of patients — the majority are normokalaemic, making clinical suspicion paramount.
Symptoms and Signs
| Feature | Frequency | Mechanism |
|---|---|---|
| Hypertension | ~100% | Sodium retention, volume expansion |
| Spontaneous hypokalaemia (K⁺ <3.5 mmol/L) | ~37% (higher in APA) | Renal potassium wasting |
| Muscle weakness / cramps | Common with hypokalaemia | Altered muscle membrane potential |
| Polyuria / polydipsia | Moderate | Nephrogenic diabetes insipidus from hypokalaemia |
| Nocturia | Moderate | Polyuria, diuretic effects |
| Headaches | Common | Hypertension |
| Palpitations / arrhythmias | Moderate | Hypokalaemia, cardiac fibrosis, AF |
| Fatigue | Common | Hypokalaemia, metabolic derangement |
| Paraesthesiae | With severe hypokalaemia | Electrolyte disturbance |
| Metabolic alkalosis | With hypokalaemia | H⁺ secretion in distal nephron |
Cardiovascular Complications
PHA produces target organ damage disproportionate to the degree of hypertension:
- Left ventricular hypertrophy (LVH) — concentric, present in 40–50% at diagnosis
- Diastolic dysfunction — prevalence 45–65%
- Atrial fibrillation — 4-fold increased risk vs essential hypertension
- Heart failure — 6-fold increased risk
- Stroke — 2-fold increased risk
- Coronary artery disease — 2.5-fold increased risk
- Albuminuria / chronic kidney disease
Screening Indications
The Endocrine Society (2016) and Australian consensus guidelines recommend screening for PHA in the following groups:
Screening Test: Aldosterone–Renin Ratio (ARR)
The plasma aldosterone concentration to plasma renin activity (PAC/PRA) ratio, or aldosterone–renin ratio (ARR), is the recommended screening test. Accuracy depends on careful preparation:
Pre-test Preparation
- Timing: Blood drawn mid-morning, after the patient has been ambulant for ≥2 hours, seated for 5–15 minutes.
- Sodium intake: Patient should follow their usual (liberal) sodium diet — salt restriction can suppress aldosterone and cause false negatives.
- Potassium: Hypokalaemia should be corrected before testing (low K⁺ can suppress aldosterone secretion, causing false negatives).
- Medication adjustments: If clinically safe, withhold for ≥4 weeks:
- Spironolactone, eplerenone, amiloride, triamterene (potassium-sparing diuretics)
- High-dose liquorice
- Less interfering medications (hold ≥2 weeks if possible): β-blockers, clonidine, methyldopa, NSAIDs, ACE inhibitors, ARBs — these affect renin but may still allow ARR interpretation.
- Acceptable medications during screening: Verapamil (slow-release), hydralazine, prazosin, doxazosin — these have minimal effect on ARR.
Interpretation
| Parameter | Positive Screening | Notes |
|---|---|---|
| ARR (pmol/L per ng/mL/h) | ≥750 | Using PAC in pmol/L and PRA in ng/mL/h |
| PAC threshold | ≥415 pmol/L (~15 ng/dL) | Both ARR and PAC must be elevated for positive screen |
| PRA threshold | <0.6 ng/mL/h (suppressed) | Confirms renin suppression |
If the initial ARR is positive, repeat testing at least once to confirm. Persistent elevation warrants confirmatory testing.
Confirmatory Tests & Adrenal Vein Sampling
Confirmatory Salt-Loading Test
A positive screening ARR must be confirmed by demonstrating non-suppressible aldosterone secretion. The Endocrine Society recommends one of four confirmatory tests; the most widely used in Australia is the oral salt-loading test:
Alternative Confirmatory Tests
| Test | Protocol | Positive Result | Availability |
|---|---|---|---|
| Fludrocortisone suppression test | Fludrocortisone 0.1 mg QID × 4 days + NaCl supplementation; upright PAC on day 4 | Upright PAC >277 pmol/L at 10:00 am | Limited — specialist centres only |
| Captopril challenge test | Captopril 25–50 mg PO; measure PAC and PRA at baseline, 1 h, and 2 h | Post-captopril ARR remains elevated; PAC not suppressed by >30% | Widely available; less sensitive |
| IV saline infusion test | 2 L 0.9% NaCl IV over 4 hours; measure PAC pre- and post-infusion | Post-infusion PAC >139 pmol/L | Requires inpatient setting; haemodynamic monitoring |
Adrenal Imaging
Once PHA is biochemically confirmed, adrenal imaging is performed for localisation. However, imaging alone is insufficient for surgical decision-making — adrenal vein sampling is essential:
- Adrenal CT (thin-cut, contrast-enhanced): First-line imaging. Detects adenomas ≥1 cm, but has limited sensitivity for micro-adenomas and may show non-functioning incidental nodules. CT discordance with AVS occurs in 37–50% of cases.
- MRI adrenal: Alternative if CT contraindicated (contrast allergy, pregnancy). Similar sensitivity to CT.
- NP-59 scintigraphy: Largely superseded by AVS; limited availability in Australia.
Adrenal Vein Sampling (AVS)
AVS is the gold standard for distinguishing unilateral APA from bilateral IHA and is mandatory before adrenalectomy in patients aged <35 years with clear unilateral adenoma on CT. In patients aged <35 with a solitary adenoma >1 cm, normal contralateral adrenal, and florid biochemical phenotype, CT alone may suffice — but this is uncommon and expert review is recommended.
| AVS Result | Interpretation | Management |
|---|---|---|
| Both SI adequate, LI ≥4 | Unilateral aldosterone production (APA or UAH) | Laparoscopic adrenalectomy of the dominant side |
| Both SI adequate, LI <4 | Bilateral aldosterone production (IHA) | Medical therapy with MR antagonist |
| One or both SI inadequate | Technical failure — repeat AVS recommended | Repeat procedure or experienced centre referral |
Management (Medical & Surgical)
Management Algorithm
Treatment depends on subtype determination (unilateral vs bilateral) and patient operability:
Surgical Management: Laparoscopic Adrenalectomy
Laparoscopic (keyhole) adrenalectomy is the treatment of choice for confirmed unilateral APA or UAH. It is well-established at all major Australian surgical centres and is performed by urologists or endocrine surgeons.
Pre-operative Optimisation
- Spironolactone 25–100 mg daily for ≥4 weeks pre-operatively to: normalise serum potassium, reduce blood pressure, correct volume expansion, and reduce peri-operative cardiovascular risk.
- Target serum K⁺ ≥4.0 mmol/L and BP <140/90 mmHg before surgery.
- If spironolactone is not tolerated (gynaecomastia, breast tenderness), substitute amiloride 5–20 mg daily.
- Additional antihypertensives as needed: calcium channel blockers (amlodipine) preferred.
- Stop spironolactone on the day of surgery.
Post-operative Care
- Hypoaldosteronism risk: The contralateral suppressed adrenal may not immediately resume aldosterone production. Monitor for hypotension, hyperkalaemia, and hyponatraemia for 1–3 months post-operatively.
- Fludrocortisone 50–100 μg daily may be required temporarily if hyperkalaemia or hypotension develops post-operatively. Taper over weeks as contralateral adrenal recovers.
- Monitor serum electrolytes (Na⁺, K⁺) at 1 week, 1 month, 3 months, and 6 months post-operatively.
- BP reassessment at 1 month — taper or cease antihypertensives as BP normalises. 50–80% of patients achieve significant BP improvement or cure.
- Biochemical cure confirmed by normalised aldosterone, potassium without supplementation, and renin recovery.
Medical Management: Mineralocorticoid Receptor Antagonists
Medical therapy is indicated for bilateral IHA, patients declining or unfit for surgery, and as adjunctive pre-operative optimisation.
MRA Monitoring Protocol
- Serum potassium and creatinine at baseline, 1 week, 4 weeks, then every 3–6 months.
- Hold spironolactone/eplerenone if K⁺ >5.5 mmol/L; reduce dose if K⁺ 5.0–5.5 mmol/L.
- Target K⁺ 4.0–5.0 mmol/L. BP target <130/80 mmHg (or <140/90 if elderly/frail).
- Avoid concurrent use with ACE inhibitors, ARBs, or potassium supplements without careful K⁺ monitoring.
- Gynaecomastia management: switch from spironolactone to eplerenone or amiloride.
Additional Antihypertensives in PHA
If MRA monotherapy is insufficient for blood pressure control, add:
- Calcium channel blockers (amlodipine 5–10 mg daily): effective, no potassium effects, PBS general benefit.
- Thiazide diuretics (hydrochlorothiazide 12.5–25 mg daily): synergistic with MRA but increase hypokalaemia risk — monitor K⁺ closely.
- ACE inhibitors / ARBs: Can be used with MRAs but increase hyperkalaemia risk. May provide some benefit in suppressing residual angiotensin II–mediated aldosterone.
- β-blockers: Less useful as renin is already suppressed; may further reduce renin and cause false-negative ARR if re-testing.
Novel and Emerging Therapies
Baxdrostat and lorundrostat are selective aldosterone synthase (CYP11B2) inhibitors currently in Phase III trials. These agents reduce aldosterone production at the enzymatic level, independent of MR, and may offer improved efficacy for resistant PHA. They are not yet available on the PBS or TGA-listed in Australia.
Monitoring and Long-Term Follow-Up
- Post-surgical: Electrolytes (Na⁺, K⁺, creatinine) at 1 week, 1 month, 3 months, 6 months, then annually. ARR at 3 months to confirm biochemical cure. BP medication review — taper/cease as appropriate.
- Medical therapy: BP, K⁺, creatinine/eGFR at 1 week after any dose change, then every 3–6 months. Annual echocardiogram if LVH present at baseline.
- Cardiovascular risk reduction: Lipid management (statins as indicated), glycaemic monitoring, smoking cessation, weight management, exercise prescription.
- Atrial fibrillation screening: Annual ECG or ambulatory monitoring if symptomatic. Consider anticoagulation per CHA₂DS₂-VASc score.
- Renal monitoring: Annual urine ACR and eGFR.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Funder JW, Carey RM, Mantero F, et al. The management of primary aldosteronism: case detection, diagnosis, and treatment: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2016;101(5):1889–1916. doi:10.1210/jc.2015-4061
- 2. Monticone S, Burrello J, Tizzani D, et al. Prevalence and clinical manifestations of primary aldosteronism encountered in primary care practice. J Am Coll Cardiol. 2017;69(14):1811–1820. doi:10.1016/j.jacc.2017.01.052
- 3. Rossi GP, Bernini G, Caliumi C, et al. A prospective study of the prevalence of primary aldosteronism in 1,125 hypertensive patients. J Am Coll Cardiol. 2006;48(11):2293–2300. doi:10.1016/j.jacc.2006.07.059
- 4. Mulatero P, Monticone S, Bertello C, et al. Long-term cardio- and cerebrovascular events in patients with primary aldosteronism. J Clin Endocrinol Metab. 2013;98(12):4826–4833. doi:10.1210/jc.2013-2805
- 5. Milliez P, Girerd X, Plouin PF, et al. Evidence for an increased rate of cardiovascular events in patients with primary aldosteronism. J Am Coll Cardiol. 2005;45(8):1243–1248. doi:10.1016/j.jacc.2005.01.015
- 6. Rossi GP, Sacchetto A, Visentin P, et al. Changes in left ventricular anatomy and function in hypertension and primary aldosteronism. Hypertension. 1996;28(5):789–795. doi:10.1161/01.HYP.28.5.789
- 7. Stowasser M, Gordon RD. Primary aldosteronism: changing definitions and new concepts of physiology and pathophysiology both inside and outside the kidney. Physiol Rev. 2016;96(4):1327–1384. doi:10.1152/physrev.00026.2015
- 8. Vaidya A, Carey RM. Evolution of the primary aldosteronism syndrome: updating the approach. J Clin Endocrinol Metab. 2020;105(12):3771–3783. doi:10.1210/clinem/dgaa604
- 9. Australian Institute of Health and Welfare (AIHW). Cardiovascular disease in Aboriginal and Torres Strait Islander people. AIHW Cardiovascular Disease Series. Canberra: AIHW; 2023.
- 10. Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018;39(33):3021–3104. doi:10.1093/eurheartj/ehy339
- 11. The Royal Australian College of General Practitioners (RACGP). Guidelines for preventive activities in general practice. 10th edition. East Melbourne: RACGP; 2018.
- 12. National Aboriginal Community Controlled Health Organisation (NACCHO). National guide to a preventive health assessment for Aboriginal and Torres Strait Islander people. 3rd edition. South Melbourne: RACGP; 2018.
- 13. Lenders JWM, Duh QY, Eisenhofer G, et al. Pheochromocytoma and paraganglioma: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2014;99(6):1915–1942. doi:10.1210/jc.2014-1498
- 14. Freel EM, Stowasser M, Gordon RD. Mineralocorticoid receptor antagonists in primary aldosteronism. Clin Endocrinol (Oxf). 2015;82(6):747–754. doi:10.1111/cen.12735
- 15. Freeman MW, Halvorsen Y-D, Marshall W, et al. Phase 2 trial of baxdrostat for treatment-resistant hypertension. N Engl J Med. 2023;388(5):395–405. doi:10.1056/NEJMoa2213169