📋 Key Information Summary
- Factitious thyrotoxicosis results from surreptitious or accidental exogenous thyroid hormone ingestion, most commonly levothyroxine (T4).
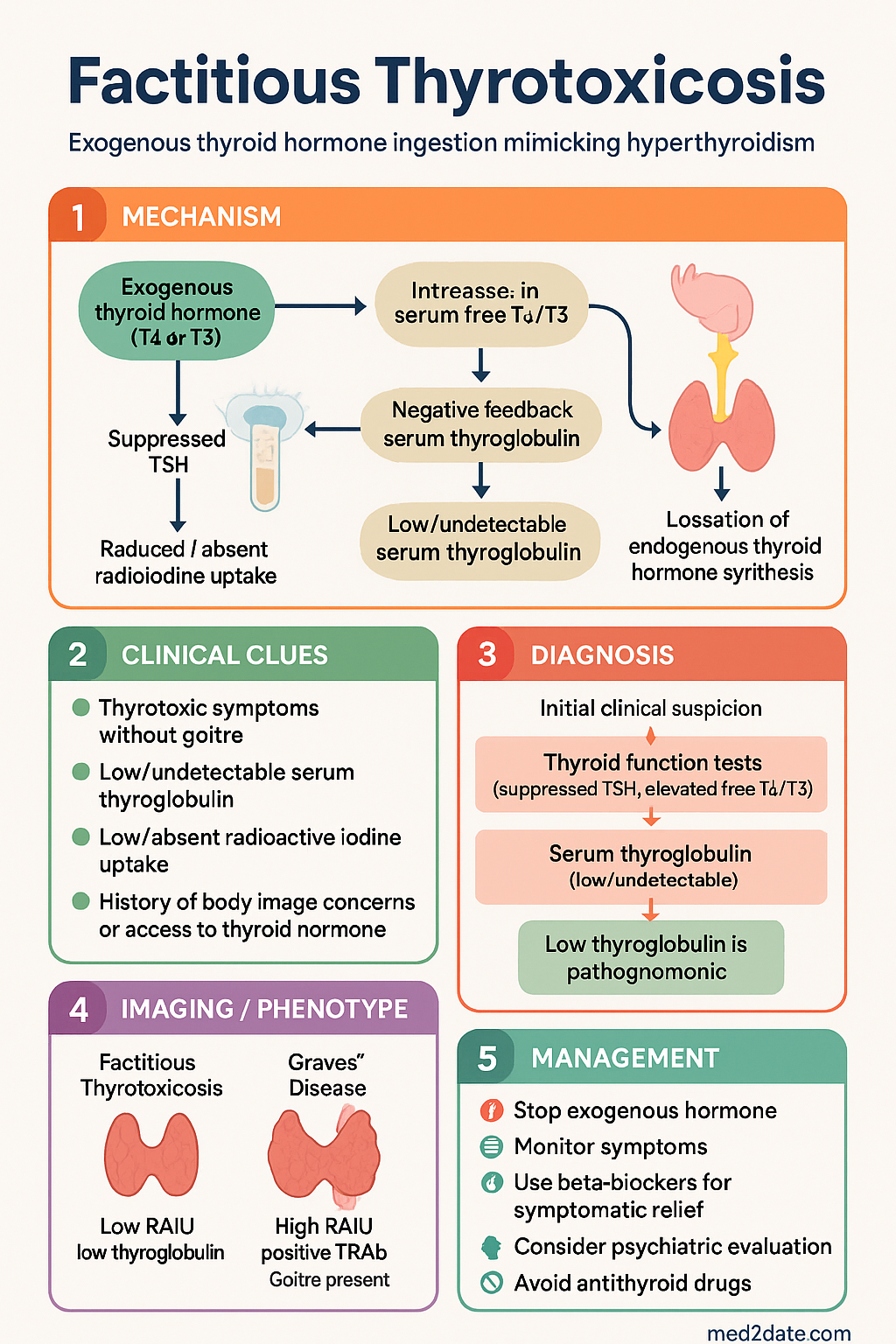
- Thyroid function tests show suppressed TSH with elevated free T4 and/or free T3 — mimicking endogenous hyperthyroidism biochemically.
- The hallmark discriminating feature is a low or undetectable serum thyroglobulin in the absence of thyroglobulin antibodies, distinguishing it from all causes of endogenous hyperthyroidism.
- Radioactive iodine uptake (RAIU) is low or absent in factitious thyrotoxicosis, contrasting with elevated uptake in Graves' disease or toxic nodular goitre.
- Clinical features include thyrotoxic symptoms without goitre, ophthalmopathy, or thyroid bruit — findings that favour Graves' disease.
- A thorough medication history is critical; patients may deny ingestion, or the source may be over-the-counter supplements or weight-loss products containing desiccated thyroid.
- Management is primarily supportive and observational: stop the exogenous hormone and monitor, as the half-life of T4 is approximately 7 days.
- Beta-blockers (propranolol or atenolol) provide symptomatic relief of adrenergic symptoms during the washout period.
- Antithyroid drugs (carbimazole, propylthiouracil) are not effective as the thyroid gland is not overproducing hormone.
- Consider underlying psychiatric illness (Munchausen syndrome, eating disorder, body dysmorphia) and arrange mental health support where appropriate.
- In cases of severe or intentional overdose, cholestyramine may accelerate T4 elimination by interrupting enterohepatic recirculation.
- Pregnancy must be excluded in women of reproductive age, as management priorities change significantly if the patient is pregnant.
🎧 Audio Brief
Introduction & Australian Epidemiology
Factitious thyrotoxicosis is a condition characterised by the clinical and biochemical features of thyrotoxicosis caused by the ingestion of exogenous thyroid hormone — most commonly levothyroxine (T4), but occasionally liothyronine (T3) or desiccated thyroid extract. It is an important mimic of endogenous hyperthyroidism and a recognised diagnostic pitfall in endocrine practice.
The condition may arise from deliberate surreptitious ingestion (self-administration in the context of Munchausen syndrome, eating disorders, or body dysmorphic disorder), iatrogenic overreplacement, or accidental ingestion — including over-the-counter weight-loss supplements contaminated with thyroid hormones. In Australia, the Therapeutic Goods Administration (TGA) has issued warnings regarding complementary medicines marketed for weight loss that contain undisclosed thyroid tissue or hormone.
Epidemiological data specific to Australia are limited, as the condition is under-reported and often misdiagnosed initially as Graves' disease. International case series suggest factitious thyrotoxicosis accounts for approximately 0.5–1% of referrals for thyrotoxicosis evaluation. The condition is more frequently identified in women aged 20–50 years, though cases occur across all demographics. Australian tertiary endocrine centres report sporadic cases, often presenting diagnostic challenges when patients deny exogenous hormone use.
Accurate recognition is essential: misdiagnosis as endogenous hyperthyroidism leads to inappropriate use of antithyroid drugs, unnecessary radioiodine therapy, or thyroidectomy — all of which carry significant morbidity. The key to diagnosis lies in the combination of suppressed TSH, elevated thyroid hormones, low thyroglobulin, and low radioiodine uptake — a pattern that is pathognomonic.
Pathophysiology & Recognition
Mechanism of Exogenous Thyrotoxicosis
When exogenous thyroid hormone (T4 or T3) enters the circulation, the resulting elevation in serum free T4 and/or free T3 exerts negative feedback on the hypothalamic–pituitary axis, suppressing TSH secretion. The suppressed TSH reduces stimulation of the thyroid gland, leading to:
- Cessation of endogenous thyroid hormone synthesis — the gland becomes quiescent.
- Decreased thyroglobulin production — thyroglobulin is a protein produced exclusively by thyroid follicular cells; when the gland is suppressed, serum thyroglobulin falls to low or undetectable levels.
- Reduced or absent radioiodine uptake — since the gland is not actively trapping iodine, RAIU is low.
In contrast, in endogenous hyperthyroidism (e.g., Graves' disease, toxic adenoma), the thyroid gland is autonomously overproducing hormone, resulting in high thyroglobulin and elevated RAIU (except in thyroiditis, where thyroglobulin is typically elevated due to gland destruction).
Sources of Exogenous Thyroid Hormone
| Source | Examples | Notes |
|---|---|---|
| Prescribed medications | Levothyroxine (Oroxine®, Eutrosig®), liothyronine (Cytomel®) | Iatrogenic overreplacement or deliberate self-administration; may be obtained from family members |
| Over-the-counter supplements | Weight-loss products, "thyroid support" supplements | May contain desiccated porcine thyroid tissue; TGA has issued alerts on contaminated products |
| Complementary/alternative medicine | Naturopathic thyroid extracts, glandular supplements | Variable and unregulated hormone content; patient may be unaware |
| Paediatric accidental ingestion | Grandparent's levothyroxine tablets | Common scenario in paediatric thyrotoxicosis evaluation |
Key Diagnostic Principles for Recognition
Clinicians should suspect factitious thyrotoxicosis when:
- Biochemical thyrotoxicosis is present without a goitre, thyroid bruit, or ophthalmopathy.
- Serum thyroglobulin is low or undetectable (in the absence of thyroglobulin antibodies).
- TSH receptor antibodies (TRAb) are negative.
- Radioiodine uptake is low or absent (if performed).
- There is a history suggestive of body image concerns, eating disorders, or prior factitious illness.
- The patient is taking or has access to thyroid hormone preparations.
Clinical Features vs Endogenous Hyperthyroidism
While the biochemical profile of factitious thyrotoxicosis may be indistinguishable from endogenous hyperthyroidism on standard thyroid function tests (TSH, free T4, free T3), several clinical features help differentiate the two.
| Feature | Factitious Thyrotoxicosis | Graves' Disease | Toxic Multinodular Goitre |
|---|---|---|---|
| Goitre | Absent (gland may atrophy) | Diffuse goitre, often with bruit | Multinodular goitre |
| Ophthalmopathy | Absent | Present in 25–50% | Absent |
| Dermopathy / pretibial myxoedema | Absent | Occasional | Absent |
| Thyroglobulin | Low / undetectable | Elevated | Elevated |
| TRAb (TSH receptor antibodies) | Negative | Positive (>95%) | Negative |
| Radioiodine uptake | Low / absent | Diffusely elevated | Patchy, variable |
| T4:T3 ratio | Higher if T4 ingestion; pure T3 elevation if liothyronine | Often T3-predominant | Usually T4-predominant |
| Response to antithyroid drugs | None (no endogenous overproduction) | Effective | Partially effective |
Shared Symptoms of Thyrotoxicosis
Regardless of the cause, patients with factitious thyrotoxicosis may exhibit the full spectrum of adrenergic and thyrotoxic symptoms:
- Palpitations, tachycardia, atrial fibrillation
- Heat intolerance, sweating
- Weight loss despite normal or increased appetite
- Tremor, anxiety, insomnia, emotional lability
- Diarrhoea or increased stool frequency
- Proximal myopathy
- Oligomenorrhoea or amenorrhoea in premenopausal women
- In severe cases: thyroid storm (rare with factitious ingestion but possible in massive overdose)
Investigations
First-Line Investigations
Second-Line / Confirmatory Investigations
Investigation Summary Table
| Test | Factitious | Graves' | Thyroiditis |
|---|---|---|---|
| TSH | ↓↓ | ↓↓ | ↓↓ |
| Free T4 / Free T3 | ↑ | ↑ | ↑ |
| Thyroglobulin | ↓↓ / undetectable | ↑↑ | ↑↑ |
| TRAb | Negative | Positive | Negative |
| RAIU | ↓↓ / absent | ↑↑ | ↓↓ / absent |
Management
Immediate Management
The cornerstone of management is cessation of exogenous thyroid hormone. No specific antidote exists. The half-life of levothyroxine (T4) is approximately 7 days, so resolution of thyrotoxicosis typically occurs over 2–4 weeks after cessation. Liothyronine (T3) has a shorter half-life (~1 day) and resolves more rapidly.
Symptomatic Management
Enhanced Elimination (Severe Overdose)
In cases of massive intentional ingestion (e.g., >5 mg levothyroxine, or any ingestion causing haemodynamic compromise), consider adjunctive measures to accelerate thyroid hormone clearance:
Management of Thyroid Storm (Rare)
Thyroid storm from exogenous hormone ingestion is rare but has been reported, particularly in paediatric accidental ingestion and intentional self-poisoning. Management follows standard thyroid storm protocols:
- ICU admission with continuous cardiac monitoring
- Beta-blockade: propranolol 1–2 mg IV (over 10 min) or 20–40 mg PO QID
- Hydrocortisone 100 mg IV Q6H (inhibits peripheral T4→T3 conversion)
- Cholestyramine 4 g PO TDS
- Consider plasmapheresis or plasma exchange in refractory cases
- Supportive care: active cooling, IV fluids, electrolyte correction
Note: Antithyroid drugs (carbimazole/PTU) and Lugol's iodine are not effective in factitious thyroid storm, as the excess hormone is exogenous. These agents are used only in endogenous thyroid storm.
Psychiatric Assessment & Follow-Up
When factitious thyrotoxicosis is confirmed — particularly in cases of surreptitious ingestion — a psychiatric evaluation should be arranged. Underlying conditions may include:
- Munchausen syndrome (factitious disorder imposed on self)
- Eating disorders (thyroid hormone used for weight loss)
- Body dysmorphic disorder
- Malingering (secondary gain, e.g., insurance claims)
- Depression, anxiety, or personality disorders
Approach the patient in a non-judgemental, supportive manner. Confrontational approaches typically result in denial and patient withdrawal from care. Multidisciplinary involvement (endocrinologist, psychiatrist, GP, social worker) is ideal.
Monitoring After Cessation
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Ross DS, Burch HB, Cooper DS, et al. 2016 American Thyroid Association guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis. Thyroid. 2016;26(10):1343-1421.
- 2. Kahaly GJ, Bartalena L, Hegedüs L, Leenhardt L, Poppe K, Pearce SH. 2018 European Thyroid Association guideline for the management of Graves' hyperthyroidism. Eur Thyroid J. 2018;7(4):167-186.
- 3. Bahn RS, Burch HB, Cooper DS, et al. Hyperthyroidism and other causes of thyrotoxicosis: management guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists. Endocr Pract. 2011;17(3):456-520.
- 4. Bharath Kumar OD, Srinivasan S. Factitious thyrotoxicosis: a diagnostic challenge. Aust Fam Physician. 2015;44(5):291-294.
- 5. The Royal Australian College of General Practitioners. RACGP clinical guidelines for thyroid disease management in primary care. Aust Fam Physician. 2020;49(Suppl):S1-S24.
- 6. Australian Institute of Health and Welfare. Thyroid disease in Australia. Cat. no. PHE 265. Canberra: AIHW; 2021.
- 7. Bogazzi F, Bartalena L, Martino E. Approach to the patient with amiodarone-induced thyrotoxicosis. J Clin Endocrinol Metab. 2010;95(11):4863-4870.
- 8. Sjoberg RJ, Simcic KJ, Kidd GS. The clinical utility of thyroglobulin measurement in the evaluation of thyroid disorders. Postgrad Med. 1993;94(4):67-74.
- 9. Mariotti S, Martino E, Cupini C, et al. Low serum thyroglobulin as a clue to the diagnosis of thyrotoxicosis factitia. N Engl J Med. 1982;307(7):410-412.
- 10. Bogazzi F, Bartalena L, Brogioni S, et al. Thyroid color flow doppler sonography and radioiodine uptake in 55 consecutive patients with amiodarone-induced thyrotoxicosis. J Endocrinol Invest. 2003;26(7):602-609.
- 11. National Health and Medical Research Council. National evidence-based guideline: diagnosis, management and prevention of thyroid disorders. Canberra: NHMRC; 2019.
- 12. Thyroid Society of Australia and New Zealand. Position statement on the investigation and management of thyrotoxicosis. Med J Aust. 2019;211(6):270-276.
- 13. Department of Health and Aged Care. Pharmaceutical Benefits Scheme: thyroid preparations. Available at: www.pbs.gov.au. Accessed 2024.