📋 Key Information Summary
- Thyroid storm is a life-threatening endocrine emergency characterised by severe thyrotoxicosis with multi-organ dysfunction — mortality 10–30% even with treatment.
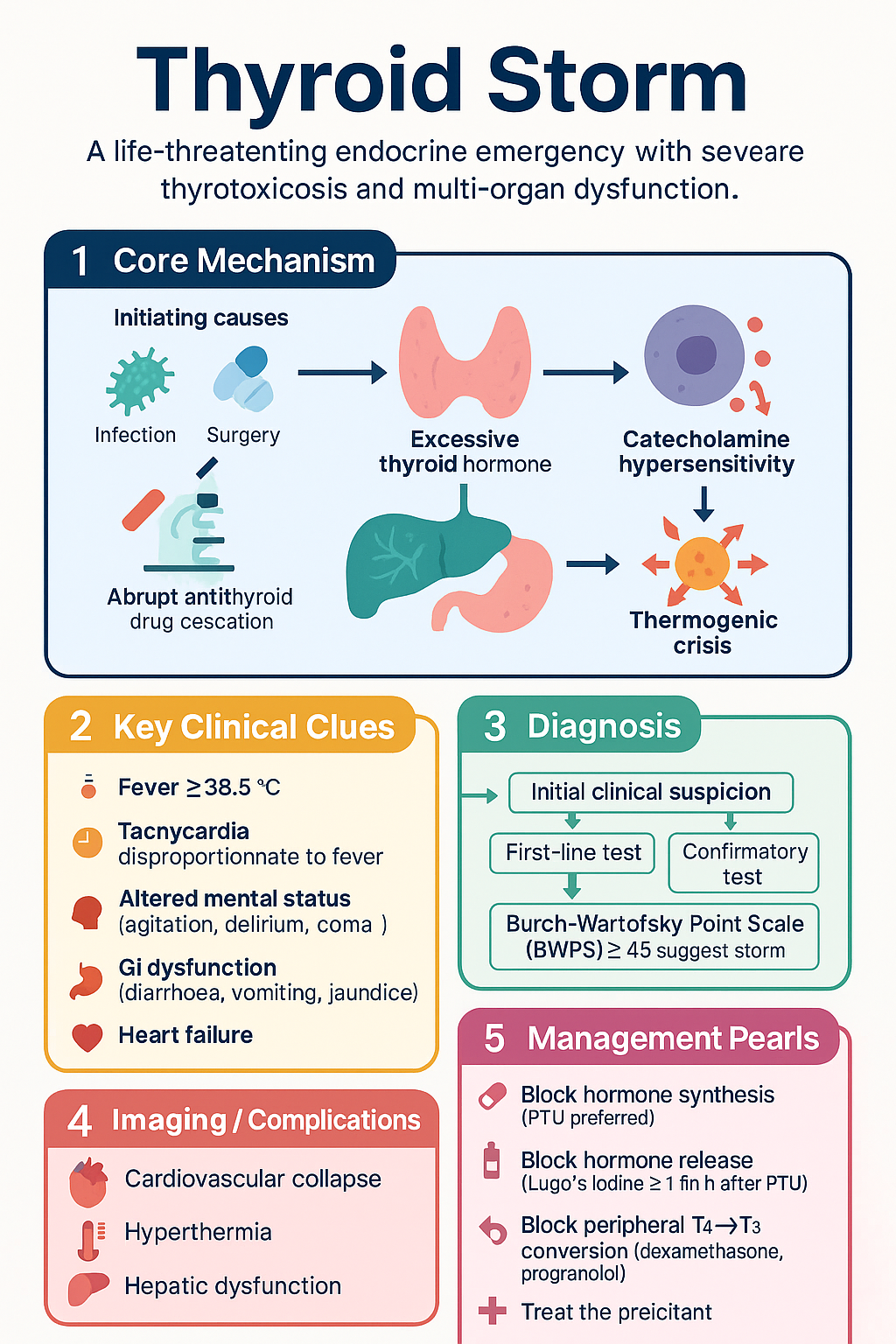
- Precipitants include infection, surgery/anaesthesia, trauma, radioiodine therapy, acute iodine load (CT contrast, amiodarone withdrawal), and abrupt antithyroid drug cessation.
- Diagnosis is clinical; the Burch–Wartofsky Point Scale (BWPS) ≥45 is highly suggestive (25–44 = impending storm).
- Core clinical features: fever ≥38.5°C, tachycardia disproportionate to fever, altered mental status (agitation, delirium, coma), GI dysfunction (diarrhoea, vomiting, jaundice), and heart failure.
- Management follows four pillars — block hormone synthesis (PTU preferred), block hormone release (Lugol's iodine ≥1 h after PTU), block peripheral T4→T3 conversion (dexamethasone, propranolol), and treat the precipitant.
- Propylthiouracil (PTU) 500 mg PO/NG loading then 250 mg every 4 h is first-line over carbimazole in storm because it also blocks peripheral T4→T3 conversion.
- Lugol's iodine (SSKI 5 drops TDS) or potassium iodide solution must be given ≥1 hour after the first dose of PTU to avoid fuelling new hormone synthesis.
- Propranolol 40–80 mg PO every 6 h (or 1–2 mg IV slow bolus) controls tachycardia and reduces peripheral T4→T3 conversion; avoid in severe heart failure or bronchospasm.
- Hydrocortisone 100 mg IV 6–8 hourly (or dexamethasone 2 mg IV 6-hourly) treats relative adrenal insufficiency and inhibits peripheral conversion.
- Active cooling with paracetamol + physical measures; avoid aspirin (displaces T4 from TBG, increasing free T4).
- Cholestyramine 4 g PO QDS reduces enterohepatic recirculation of thyroid hormones as adjunctive therapy.
- ICU admission is mandatory; liaise early with endocrinology and consider plasmapheresis or thyroidectomy as rescue in refractory cases.
- Aboriginal and Torres Strait Islander patients have higher Graves' disease prevalence; culturally safe care, interpreter services, and remote telehealth endocrinology input are essential.
🎧 Audio Brief
Introduction & Australian Epidemiology
Thyroid storm is a life-threatening exacerbation of thyrotoxicosis, representing the extreme end of the hyperthyroid spectrum. It is characterised by severe multi-organ decompensation — cardiovascular collapse, hyperthermia, altered consciousness, and hepatic/gastrointestinal dysfunction — and carries a mortality rate of 10–30% even with prompt, aggressive management.
In Australia, thyroid storm accounts for fewer than 2% of all thyrotoxicosis presentations but is disproportionately fatal. The most common underlying aetiology is Graves' disease, followed by toxic multinodular goitre and, less commonly, thyroiditis. The condition is triggered by an acute physiological stressor superimposed on existing (sometimes unrecognised) thyrotoxicosis.
Population-based data from the Australian Institute of Health and Welfare (AIHW) indicate that thyroid disorders affect approximately 1 in 10 Australians, with hyperthyroidism prevalence of 1.2–1.6%. Aboriginal and Torres Strait Islander populations have a higher burden of autoimmune thyroid disease, and remote-area patients face delayed recognition due to limited specialist access. Paediatric thyroid storm, although rare, has been reported in adolescent Graves' disease and carries a particularly high morbidity.
This guideline provides evidence-based recommendations for the recognition, scoring, investigation, and emergency management of thyroid storm in Australian clinical practice, aligned with Therapeutic Guidelines (eTG), the Australian Commission on Safety and Quality in Health Care (ACSQHC), and Endocrine Society of Australia (ESA) consensus statements.
Pathophysiology & Precipitants
Pathophysiology
Thyroid storm represents a state of extreme thyroid hormone excess combined with a heightened catecholamine response and systemic inflammatory activation. Several mechanisms converge:
- Excessive thyroid hormone: Markedly elevated free T4 (fT4) and free T3 (fT3) saturate nuclear thyroid hormone receptors in virtually every organ, increasing basal metabolic rate by up to 60–100%.
- Catecholamine hypersensitivity: Thyroid hormones upregulate β-adrenergic receptors, amplifying the haemodynamic effects of endogenous catecholamines — tachycardia, systolic hypertension with wide pulse pressure, and high-output cardiac failure.
- Thermogenic crisis: Uncoupled oxidative phosphorylation and increased Na⁺/K⁺-ATPase activity generate excessive heat, leading to hyperthermia that is often refractory to conventional antipyretics.
- Multi-organ dysfunction: Hepatic ischaemia causes conjugated hyperbilirubinaemia (jaundice); cerebral hyperperfusion and catecholamine excess cause delirium or coma; myocardial oxygen demand exceeds supply, precipitating heart failure or arrhythmia.
- Relative adrenal insufficiency: Accelerated cortisol metabolism in severe thyrotoxicosis depletes cortisol reserves, contributing to haemodynamic instability.
Common Precipitants
| Precipitant | Mechanism / Notes |
|---|---|
| Infection / sepsis | Most common trigger; cytokine-mediated increase in thyroid hormone release and peripheral conversion |
| Surgery / anaesthesia | Thyroid or non-thyroid surgery; manipulation of thyroid gland; inadequate pre-operative euthyroidism |
| Abrupt antithyroid drug cessation | Rebound hormone surge in Graves' disease |
| Radioiodine (RAI) therapy | Radiation thyroiditis with acute hormone release; pre-treat with antithyroid drugs if large gland or high fT4 |
| Iodine load | IV contrast for CT, amiodarone (both initiation and withdrawal — Jod-Basedow phenomenon or Wolff–Chaikoff failure) |
| Trauma / DKA / PE | Acute physiological stress; diabetic ketoacidosis is an under-recognised trigger |
| Parturition | Labour and delivery in undiagnosed or poorly controlled Graves' disease |
| Excessive thyroid hormone ingestion | Factitious thyrotoxicosis or intentional self-harm with levothyroxine |
Clinical Features & Scoring (Burch–Wartofsky)
Cardinal Features
- Hyperthermia: Temperature ≥38.5°C, often 39.5–41°C; diaphoretic, flushed skin.
- Cardiovascular: Tachycardia (HR >140 bpm) disproportionate to fever; systolic hypertension with wide pulse pressure; atrial fibrillation; high-output heart failure; cardiogenic shock.
- Neurological: Agitation, restlessness, anxiety progressing to delirium, psychosis, seizures, stupor, or coma (thyroid encephalopathy).
- Gastrointestinal: Nausea, vomiting, profuse diarrhoea, abdominal pain; hepatic dysfunction with conjugated hyperbilirubinaemia (jaundice).
- Respiratory: Tachypnoea, pulmonary oedema, respiratory failure.
- Miscellaneous: Goitre (may be absent in thyroiditis-induced storm), tremor, proximal myopathy, diaphoresis.
Burch–Wartofsky Point Scale (BWPS)
The BWPS is the most widely used scoring system for thyroid storm. It integrates thermoregulatory, cardiovascular, CNS, GI/hepatic, and precipitant parameters.
| Parameter | Criteria | Points |
|---|---|---|
| Temperature | 37.2–37.7 °C | 5 |
| 37.8–38.2 °C | 10 | |
| 38.3–38.8 °C | 15 | |
| 38.9–39.4 °C / ≥39.5 °C | 20 / 30 | |
| Heart rate | 100–109 / 110–119 bpm | 5 / 10 |
| 120–129 / 130–139 bpm | 15 / 20 | |
| ≥140 bpm | 25 | |
| Atrial fibrillation (add) | +10 | |
| CNS dysfunction | Absent | 0 |
| Mild (agitation) | 10 | |
| Moderate (delirium, psychosis, extreme lethargy) | 20 | |
| Severe (seizure, coma) | 30 | |
| GI / hepatic | Diarrhoea, nausea, vomiting, abdominal pain | 10 |
| Jaundice | 20 | |
| Precipitant history | Identifiable precipitant present | 10 |
| Heart failure | Peripheral oedema / bibasal crackles | 5 / 15 |
Investigations
Baseline Urgent Bloods
Imaging & Other Investigations
Emergency Management
Management of thyroid storm follows four concurrent pillars. All interventions should be initiated simultaneously in the emergency department and continued in ICU/HDU.
The Four Pillars of Thyroid Storm Management
Pillar 1 — Antithyroid Drugs (Block Synthesis)
Pillar 2 — Inorganic Iodine (Block Hormone Release)
Pillar 3 — Beta-Blockers & Corticosteroids
Beta-Blockers
Corticosteroids
Pillar 4 — Supportive Care & Treat Precipitant
| Intervention | Details |
|---|---|
| ICU / HDU admission | All patients with definite or likely storm (BWPS ≥45); continuous telemetry, invasive BP if shocked |
| IV fluid resuscitation | Isotonic crystalloid (0.9% NaCl or Hartmann's) 1–2 L bolus then 100–200 mL/h; monitor for fluid overload (high-output HF) |
| Active cooling | Paracetamol 1 g PO/IV QID (avoid aspirin — displaces T4 from TBG); ice packs, cooling blankets, evaporative cooling. Avoid dantrolene (unproven) |
| Infection source control | Broad-spectrum antibiotics if sepsis suspected (per eTG Antibiotic); blood cultures before first dose |
| Cholestyramine | 4 g PO QDS — reduces enterohepatic recycling of thyroid hormones; adjunctive, not a substitute for thionamides |
| VTE prophylaxis | Enoxaparin 40 mg SC OD (or 20 mg if CrCl <30); hyperthyroidism is prothrombotic |
| Avoid | Aspirin (↑ free T4), excessive sedation (respiratory depression), iodinated contrast (fuels hormone synthesis unless PTU on board) |
Adjunctive & Rescue Therapies
| Therapy | Indication | Notes |
|---|---|---|
| Plasmapheresis / plasma exchange | Refractory storm; severe organ failure unresponsive to 24–48 h of standard Rx | Rapidly reduces circulating T4/T3; available at major tertiary centres (e.g., RPA, Royal Melbourne, RBWH); discuss with nephrology/haematology |
| Emergency thyroidectomy | Last resort; refractory to medical Rx or contraindications to all medical options | Near-total thyroidectomy; requires experienced endocrine surgeon; pre-optimise with PTU + β-blocker + iodine for ≥1 h; high surgical risk |
| Potassium iodide (KI) via IV | If unable to take PO/NG and SSKI unavailable | Not routinely available in Australian hospitals; sodium iodide 500 mg IV over 24 h is an alternative (sourced through Special Access Scheme) |
| Bile-acid sequestrants | Adjunct to reduce enterohepatic recycling | Cholestyramine 4 g PO QDS or colestipol; separate from other medications by 1–2 h |
Treatment Timeline
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Akamizu T. Thyroid storm: a Japanese perspective. Thyroid. 2018;28(1):32–40. doi:10.1089/thy.2017.0243
- 2. Burch HB, Wartofsky L. Life-threatening thyrotoxicosis: thyroid storm. Endocrinol Metab Clin North Am. 1993;22(2):263–277.
- 3. Ross DS, Burch HB, Cooper DS, et al. 2016 American Thyroid Association guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis. Thyroid. 2016;26(10):1343–1421. doi:10.1089/thy.2016.0229
- 4. Satoh T, Isozaki O, Suzuki A, et al. 2016 Guidelines for the management of thyroid storm from the Japan Thyroid Association and Japan Endocrine Society (First edition). Endocr J. 2016;63(12):1025–1064.
- 5. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.
- 6. Australian Institute of Health and Welfare (AIHW). Thyroid disease in Australia. Cat. no. PHE 250. Canberra: AIHW; 2020.
- 7. Endocrine Society of Australia (ESA). Position statement on the management of thyroid disorders in pregnancy. Med J Aust. 2019;211(2):75–80.
- 8. Royal Australian College of General Practitioners (RACGP). Thyroid disease — a clinical update. Aust Fam Physician. 2019;48(10):718–724.
- 9. Angell TE, Lechner MG, Nguyen CT, Salvato VE, Nicoloff JT, LoPresti JS. Clinical features and hospital outcomes in thyroid storm: a retrospective cohort study. J Clin Endocrinol Metab. 2015;100(2):457–464.
- 10. Carroll R, Matfin G. Endocrine and metabolic emergencies: thyroid storm. Ther Adv Endocrinol Metab. 2010;1(3):139–145. doi:10.1177/2042018810382481
- 11. Aboriginal and Torres Strait Islander Health Performance Framework. Australian Institute of Health and Welfare; 2023. Available from: https://www.aihw.gov.au/reports/indigenous-australians/indigenous-health-performance-framework
- 12. Pharmaceutical Benefits Scheme (PBS). Australian Government Department of Health. Available from: https://www.pbs.gov.au