📋 Key Information Summary
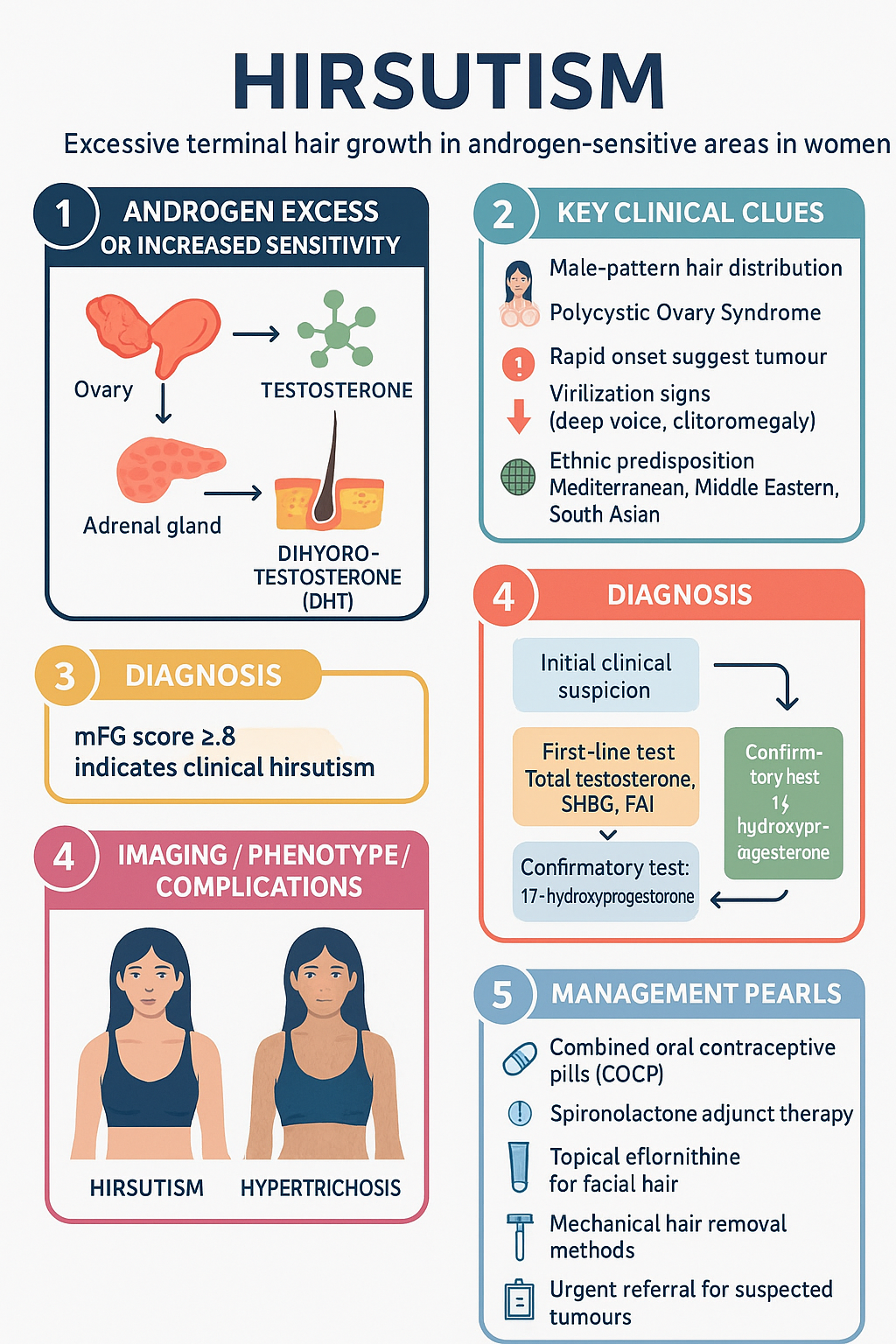
- Hirsutism is defined as excessive terminal hair growth in androgen-sensitive areas in women, following a male-pattern distribution, affecting approximately 5–10% of Australian women of reproductive age.
- Polycystic ovary syndrome (PCOS) accounts for 70–80% of hirsutism cases and must be evaluated in every patient presenting with excess androgenic hair growth.
- The modified Ferriman–Gallwey (mFG) score ≥8 is the standard threshold for clinical hirsutism; scores ≥8 warrant full endocrine investigation.
- Initial investigations include total testosterone, sex hormone-binding globulin (SHBG), free androgen index (FAI), 17-hydroxyprogesterone, thyroid function, and prolactin.
- Total testosterone >5 nmol/L or DHEA-S >twice the upper limit of normal should prompt urgent investigation for androgen-secreting tumours.
- First-line pharmacotherapy for hirsutism in PCOS is a combined oral contraceptive pill (COCP) — ethinyloestradiol/cyproterone acetate or ethinyloestradiol/drospirenone are preferred in Australia.
- Spironolactone 100–200 mg daily is the most effective anti-androgen adjunct; it is PBS-listed for this indication and should be used with reliable contraception.
- Topical eflornithine 13.9% (Vaniqa®) is PBS Authority Required and provides adjunctive facial hair reduction when combined with hormonal therapy.
- Pharmacotherapy requires a minimum 6-month trial before efficacy can be assessed; hair growth cycles dictate that visible improvement takes 4–6 months.
- Mechanical and cosmetic therapies (laser hair removal, electrolysis, waxing) complement pharmacotherapy but do not address the underlying cause.
- Non-classic congenital adrenal hyperplasia (NCCAH) due to 21-hydroxylase deficiency must be excluded with a morning 17-hydroxyprogesterone level; prevalence is 1–2% of the general population and 5–10% among women with hirsutism.
- Aboriginal and Torres Strait Islander women have a higher prevalence of PCOS and metabolic syndrome, requiring earlier metabolic screening and culturally safe management approaches.
🎧 Audio Brief
Introduction & Australian Epidemiology
Hirsutism is the excessive growth of terminal hair in androgen-sensitive areas in women, following a male-pattern distribution. It results from the interaction of circulating androgens with hair follicle 5α-reductase activity, converting testosterone to the more potent dihydrotestosterone (DHT). Hirsutism must be distinguished from hypertrichosis, which is generalised excess vellus hair growth not androgen-dependent.
In Australia, hirsutism affects approximately 5–10% of women of reproductive age, with the prevalence varying by ethnicity. Women of Mediterranean, Middle Eastern, and South Asian descent are more likely to present due to both a higher biological predisposition and greater psychosocial impact. Aboriginal and Torres Strait Islander women have a higher prevalence of PCOS and associated metabolic risk factors.
The condition carries significant psychosocial burden, with studies demonstrating increased rates of anxiety, depression, and impaired quality of life comparable to those seen in chronic dermatological conditions. Many patients delay seeking medical advice for years, having normalised the condition or been reassured inappropriately.
Aetiology & Pathophysiology
Mechanism of Androgen-Mediated Hair Growth
Hair follicles in androgen-sensitive areas (face, chest, abdomen, back, upper arms, thighs) respond to circulating androgens — principally testosterone and DHT. In the hair follicle, testosterone is converted to DHT by type 2 5α-reductase. DHT binds to the androgen receptor, stimulating vellus-to-terminal hair conversion and increasing the duration of the anagen (growth) phase. The clinical expression of hirsutism depends on the balance between circulating androgen levels, local 5α-reductase activity, and individual genetic sensitivity.
Causes of Hirsutism
| Category | Conditions | Approximate Frequency |
|---|---|---|
| Ovarian | PCOS (most common), ovarian hyperthecosis, androgen-secreting ovarian tumours (thecoma, Sertoli–Leydig cell tumour) | 70–80% |
| Adrenal | Non-classic congenital adrenal hyperplasia (21-hydroxylase deficiency), Cushing syndrome, adrenal carcinoma, adrenal adenoma | 5–10% |
| Iatrogenic / Exogenous | Anabolic steroids, danazol, valproate, testosterone, ciclosporin, phenytoin, minoxidil | 5–10% |
| Idiopathic | Normal androgen levels, increased peripheral sensitivity; often familial | 5–15% |
PCOS — The Predominant Cause
PCOS accounts for 70–80% of hirsutism presentations. The pathophysiology involves a self-perpetuating cycle of:
- LH hypersecretion and increased LH:FSH ratio driving ovarian androgen production
- Insulin resistance and compensatory hyperinsulinaemia — insulin acts as a co-gonadotrophin on ovarian theca cells and suppresses hepatic SHBG production, increasing free testosterone
- Reduced SHBG leading to a higher free androgen index (FAI)
- Adrenal androgen excess (DHEA-S) in approximately 20–30% of PCOS patients
- Central adiposity amplifying insulin resistance through adipokine-mediated pathways
The Rotterdam criteria (2003) define PCOS as two of three: oligo-anovulation, clinical and/or biochemical hyperandrogenism, and polycystic ovarian morphology on ultrasound — after exclusion of other causes.
Non-Classic Congenital Adrenal Hyperplasia (NCCAH)
NCCAH due to partial 21-hydroxylase deficiency (CYP21A2 mutations) is present in 1–2% of the general population and 5–10% of women presenting with hirsutism. It is inherited in an autosomal recessive manner. Impaired cortisol synthesis leads to ACTH-driven adrenal androgen overproduction. A morning 17-hydroxyprogesterone level >30 nmol/L (or >45 nmol/L post-Synacthen stimulation) is diagnostic.
Idiopathic Hirsutism
Defined as hirsutism with normal ovulatory function and normal circulating androgen levels. This likely reflects increased peripheral 5α-reductase activity or enhanced androgen receptor sensitivity. It tends to be familial and is a diagnosis of exclusion.
Clinical Assessment & Investigations
History
A thorough history should include:
- Onset and progression: Gradual onset since puberty suggests PCOS or idiopathic hirsutism; rapid onset or progression over months raises concern for neoplasm
- Menstrual history: Oligomenorrhoea, amenorrhoea, or irregular cycles suggest anovulation (PCOS)
- Virilisation features: Deepening of voice, clitoromegaly, temporal recession, increased muscle bulk — any feature warrants urgent investigation
- Medication review: Anabolic steroids (including concealed use), valproate, danazol, testosterone therapy
- Family history: PCOS, type 2 diabetes, premature adrenarche, NCCAH
- Weight history and metabolic symptoms: Central obesity, acanthosis nigricans (insulin resistance marker), gestational diabetes
- Fertility goals: Influences management approach and urgency
- Psychosocial impact: Assess using validated tools where available; many patients minimise distress
Modified Ferriman–Gallwey Score
The modified Ferriman–Gallwey (mFG) scoring system is the gold standard for objectively grading hirsutism. Nine androgen-sensitive body areas are scored from 0 (no terminal hair) to 4 (frankly virile), yielding a total score of 0–36.
Examination
- Calculate the mFG score systematically
- Assess for acanthosis nigricans (neck, axillae, groin) — a marker of insulin resistance
- Check for signs of Cushing syndrome: moon face, buffalo hump, striae, central obesity, proximal myopathy
- Palpate thyroid — goitre may indicate thyroid dysfunction
- Assess body habitus, BMI, waist circumference (metabolic risk)
- Examine for clitoromegaly (clitoral index >35 mm²) and temporal hair recession
- Assess galactorrhoea (hyperprolactinaemia)
Investigations
• Total testosterone >5 nmol/L
• DHEA-S >twice the upper limit of normal
• Rapid onset or rapidly progressive hirsutism (<1 year)
• Any virilisation (clitoromegaly, voice deepening, temporal recession)
• Postmenopausal new-onset hirsutism
Differential Diagnosis
It is essential to distinguish hirsutism from hypertrichosis (generalised non-androgen-dependent hair growth) and to identify the underlying cause of true hirsutism.
Hirsutism vs Hypertrichosis
| Feature | Hirsutism | Hypertrichosis |
|---|---|---|
| Hair type | Terminal (dark, coarse) | Vellus or lanugo (fine, may be pigmented) |
| Distribution | Androgen-dependent (male pattern) | Non-androgen-dependent areas (forearms, legs, back) |
| Cause | Androgen excess or increased sensitivity | Drugs (phenytoin, ciclosporin, minoxidil), thyroid, anorexia, porphyria, familial |
| Androgens | Often elevated | class="guideline-td">Normal
Differential Diagnosis by Androgen Level
| Pattern | Differential | Key Distinguishing Features |
|---|---|---|
| Normal androgens | Idiopathic hirsutism | Normal menses, normal androgens, diagnosis of exclusion; familial |
| Hypertrichosis | Non-androgen distribution; consider drug causes | |
| Mild androgen elevation | PCOS | Oligomenorrhoea, polycystic ovaries, insulin resistance, acanthosis nigricans |
| NCCAH | Elevated 17-OHP, similar phenotype to PCOS, family history of consanguinity | |
| Moderate elevation | Cushing syndrome | Central obesity, striae, proximal myopathy, moon face, easy bruising |
| Classic CAH (late-onset) | Very high 17-OHP, ambiguous genitalia in neonates (if severe) | |
| Marked elevation | Ovarian tumour (thecoma, Sertoli–Leydig) | Rapid onset, virilisation, pelvic mass on examination or imaging |
| Adrenal carcinoma | Very high DHEA-S, abdominal mass, rapid onset virilisation, Cushingoid features | |
| Ovarian hyperthecosis | Postmenopausal, marked hyperandrogenism, insulin resistance |
Investigations to Exclude Differential Diagnoses
- Cushing syndrome: 24-hour urinary free cortisol, late-night salivary cortisol, or 1 mg overnight dexamethasone suppression test. If positive, proceed to low-dose dexamethasone suppression and ACTH level.
- Prolactinoma: Serum prolactin; if elevated, MRI pituitary with contrast.
- Acromegaly: IGF-1 level if clinical features present (coarse features, prognathism, carpal tunnel).
- Thyroid dysfunction: TSH and free T4.
- Drug-induced: Comprehensive medication review including supplements and over-the-counter products.
Treatment
Treatment of hirsutism involves a dual approach: (1) pharmacological suppression of androgen production/action, and (2) mechanical/cosmetic hair removal. Optimal outcomes require both modalities. Patients must understand that pharmacotherapy takes a minimum of 6 months to demonstrate effect due to the hair growth cycle.
Pharmacological Therapy — First-Line
Pharmacological Therapy — Second-Line / Adjunctive
Treatment Algorithm
Mechanical & Cosmetic Therapies
Cosmetic measures should be offered to all patients alongside pharmacotherapy, as they provide immediate improvement while drug therapy takes effect.
| Method | Mechanism | Suitable Areas | Notes |
|---|---|---|---|
| Laser hair removal | Selective photothermolysis of melanin in hair follicle | All areas; most effective on dark hair / lighter skin (Fitzpatrick I–III) | Multiple sessions (6–10) required. Nd:YAG laser preferred for darker skin types. Not PBS-funded. Reduces hair by 50–80%. |
| Electrolysis | Thermolysis or galvanic current destroys individual follicles | Small areas (face, chin) | Only truly permanent method. Slow (individual follicles). Operator-dependent. Not PBS-funded. |
| Waxing / Threading | Mechanical epilation | Face, body | Temporary; regrowth in 2–6 weeks. May cause folliculitis or irritation. |
| Shaving | Cuts hair at skin surface | All areas | Does not worsen hair growth (myth). Convenient but requires daily maintenance. |
| Depilatory creams | class="guideline-td">Chemical dissolution of hair shaft (thioglycolate)Body (avoid face if sensitive) | Temporary; may cause irritation. Trial on small area first. | |
| Bleaching | Lightens hair colour | Face, arms | Does not reduce growth; reduces visibility. Simple and inexpensive. |
Special Populations
Aboriginal and Torres Strait Islander Health
Aboriginal and Torres Strait Islander women have a higher prevalence of PCOS, metabolic syndrome, type 2 diabetes, and cardiovascular disease compared to non-Indigenous Australians. Hirsutism in this population may be more common and more severe, with earlier onset and greater metabolic comorbidity. Culturally safe, patient-centred care is essential.
Monitoring & Follow-Up
Monitoring Schedule
When to Refer
- Urgent endocrine referral: Total testosterone >5 nmol/L, DHEA-S >twice ULN, virilisation features, rapid-onset hirsutism
- Routine endocrine referral: Suspected NCCAH (equivocal 17-OHP), suspected Cushing syndrome, failed first-line therapy at 12 months
- Gynaecology referral: Fertility concerns in PCOS, ultrasound findings suggesting ovarian pathology
- Dermatology referral: Specialist laser or electrolysis, complex skin-type considerations, refractory hirsutism
- Psychology referral: Significant psychological distress, body dysmorphic features, depression/anxiety related to hirsutism
Quick Reference — Investigation Interpretation
📚 References
- 1. Azziz R, Carmina E, Chen Z, et al. Polycystic ovary syndrome. Nature Reviews Disease Primers. 2016;2:16057.
- 2. Martin KA, Anderson RR, Chang RJ, et al. Evaluation and treatment of hirsutism in premenopausal women: an Endocrine Society Clinical Practice Guideline. Journal of Clinical Endocrinology & Metabolism. 2018;103(4):1233–1257.
- 3. Teede HJ, Misso ML, Costello MF, et al. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Human Reproduction. 2018;33(9):1602–1618.
- 4. Royal Australian College of General Practitioners (RACGP). General practice management of type 2 diabetes: 2016–2018. East Melbourne: RACGP; 2016.
- 5. Australian Institute of Health and Welfare (AIHW). Polycystic ovary syndrome (PCOS) in Australia. Cat. no. PHE 277. Canberra: AIHW; 2020.
- 6. Escobar-Morreale HF. Polycystic ovary syndrome: definition, aetiology, diagnosis and treatment. Nature Reviews Endocrinology. 2018;14(5):270–284.
- 7. Somani N, Turvy D. Hirsutism: an evidence-based treatment update. American Journal of Clinical Dermatology. 2014;15(3):229–239.
- 8. Yildiz BO, Bolour S, Woods K, et al. Visually scoring hirsutism. Human Reproduction Update. 2010;16(1):51–64.
- 9. Australasian College of Dermatologists. Position statement: laser and light-based therapies. Sydney: ACD; 2022.
- 10. National Aboriginal Community Controlled Health Organisation (NACCHO). Framework for the delivery of Aboriginal and Torres Strait Islander primary health care. Canberra: NACCHO; 2023.
- 11. Pharmaceuticals Benefits Scheme (PBS). PBS Schedule: spironolactone, eflornithine, combined oral contraceptives. Australian Government Department of Health. Accessed 2024. Available at: pbs.gov.au.
- 12. McCartney CR, Marshall JC. Polycystic ovary syndrome. New England Journal of Medicine. 2016;375(1):54–64.