📋 Key Information Summary
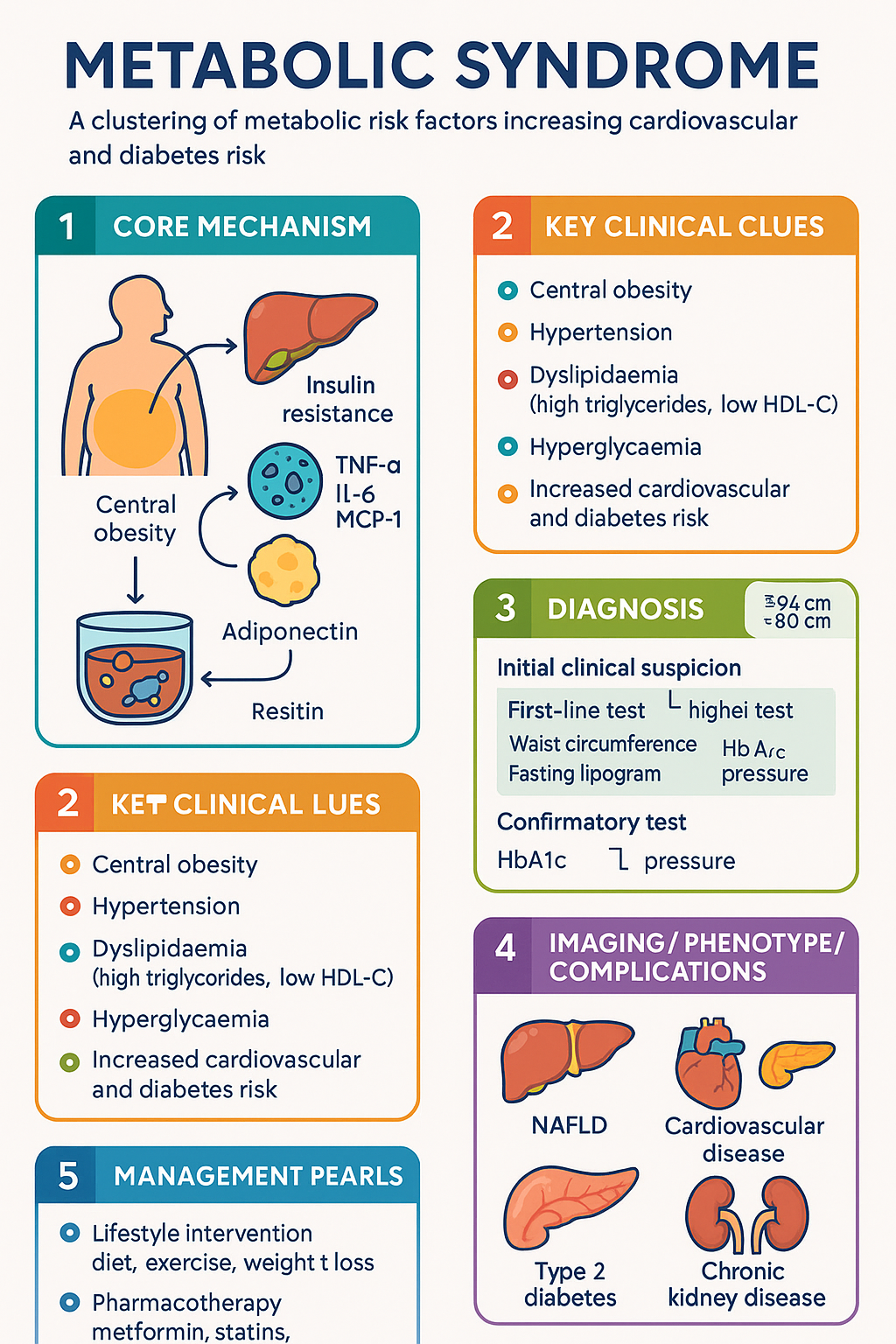
- Metabolic syndrome (MetS) is a clustering of central obesity, hypertension, dyslipidaemia, and hyperglycaemia that synergistically amplifies cardiovascular disease (CVD) and type 2 diabetes mellitus (T2DM) risk.
- Prevalence in Australia is approximately 30–35% of adults aged ≥25 years; higher in rural, socioeconomically disadvantaged, and Aboriginal and Torres Strait Islander populations.
- Diagnosis requires ≥3 of 5 criteria using the harmonised definition (IDF/AHA/NHLBI 2009): waist circumference, triglycerides, HDL-C, blood pressure, and fasting glucose.
- Central insulin resistance with compensatory hyperinsulinaemia is the principal pathophysiological driver, linking all five components.
- MetS doubles the risk of CVD events and increases T2DM risk five-fold within 5–10 years.
- Waist circumference thresholds differ by ethnicity; for Australian adults, ≥94 cm (men) and ≥80 cm (women) are recommended.
- Lifestyle intervention — structured diet, ≥150 min/week moderate-intensity exercise, and 5–7% weight loss — is the cornerstone first-line therapy.
- Pharmacotherapy targets individual components: metformin for glycaemic control and modest weight reduction; statins for atherogenic dyslipidaemia; antihypertensives (ACE inhibitors or ARBs preferred) for blood pressure.
- GLP-1 receptor agonists (e.g., semaglutide, liraglutide) and SGLT2 inhibitors offer metabolic, cardiovascular, and renal benefits beyond glycaemic control and are increasingly used early.
- Bariatric surgery should be considered for BMI ≥40 kg/m² or ≥35 kg/m² with metabolic comorbidities when lifestyle and pharmacotherapy are insufficient.
- Assessment must include fasting lipogram, fasting glucose or HbA1c, liver function (NAFLD screening), urine albumin-to-creatinine ratio, and Framingham or QRISK cardiovascular risk score.
- Annual monitoring of metabolic parameters, weight, blood pressure, and renal function is essential; more frequent review if on pharmacotherapy.
- Aboriginal and Torres Strait Islander peoples experience MetS at younger ages and higher rates; culturally safe, community-led programmes improve engagement and outcomes.
🎧 Audio Brief
Introduction & Australian Epidemiology
Metabolic syndrome (MetS) describes a constellation of interrelated metabolic risk factors — central obesity, elevated blood pressure, atherogenic dyslipidaemia (raised triglycerides and low HDL-cholesterol), and impaired fasting glucose — that, when co-existing, confer substantially greater cardiovascular and type 2 diabetes mellitus (T2DM) risk than any single component alone. The concept emerged from early observations by Reaven (1988) linking insulin resistance to hypertension and dyslipidaemia, subsequently codified by the World Health Organization (1998), the European Group for the Study of Insulin Resistance (EGIR, 1999), the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III, 2001), and most recently the harmonised Joint Interim Statement (IDF/AHA/NHLBI, 2009).
In Australia, the AusDiab study (Dunstan et al., 2001) and the more recent Australian Bureau of Statistics National Health Survey (2017–18) indicate that approximately one in three adults aged ≥25 years meets criteria for MetS. Prevalence increases markedly with age, reaching over 50% in those aged ≥65 years. Men tend to present earlier (45–54 years) while women's prevalence rises sharply post-menopause. Socioeconomic gradients are pronounced: rates are highest in the most disadvantaged quintiles and in regional and remote areas.
The economic burden is substantial: MetS-related hospitalisations, medications, and lost productivity cost the Australian healthcare system an estimated AUD $3.2 billion annually (Deloitte Access Economics, 2019). Importantly, MetS is modifiable — structured lifestyle programmes and targeted pharmacotherapy can reduce CVD events by 20–50% and T2DM incidence by up to 58% (Da Qing, Finnish DPS, DPP trials).
Definition & Diagnostic Criteria
Multiple definitions have been proposed. The harmonised Joint Interim Statement (2009) is recommended for Australian practice as it retains ethnic-specific waist-circumference thresholds while standardising the remaining four criteria.
| Criterion | Threshold | Notes |
|---|---|---|
| Waist circumference | Men ≥94 cm; Women ≥80 cm (Caucasian/European ethnicity) | Lower thresholds for South Asian, Chinese, Japanese populations. Performed at the midpoint between the iliac crest and lowest rib, at end-expiration. |
| Triglycerides | ≥1.7 mmol/L (or on treatment) | Fasting sample preferred; non-fasting ≥2.0 mmol/L is increasingly accepted. |
| HDL-cholesterol | Men <1.0 mmol/L; Women <1.3 mmol/L (or on treatment) | Low HDL-C is a strong independent predictor of atherogenic risk. |
| Blood pressure | Systolic ≥130 mmHg and/or diastolic ≥85 mmHg (or on antihypertensive Rx) | Confirm with ≥2 readings on ≥2 occasions; ambulatory BP monitoring if white-coat suspected. |
| Fasting glucose | ≥5.6 mmol/L (or on treatment for elevated glucose) | HbA1c ≥5.5% (38 mmol/mol) may identify additional at-risk individuals. |
Diagnosis requires ≥3 of these 5 criteria. A single fasting blood test (glucose, lipogram) plus clinical assessment (waist circumference, blood pressure) is usually sufficient. The MBS item 66832 (fasting lipogram) and 66841 (fasting glucose/HbA1c) are routinely used in Australian general practice.
Pathophysiology (Insulin Resistance)
Central (visceral) adiposity is the primary driver. Excess visceral fat undergoes lipolysis, releasing free fatty acids (FFAs) into the portal circulation. FFAs impair hepatic insulin signalling, promote hepatic gluconeogenesis and VLDL-triglyceride synthesis, and induce hepatic steatosis. Simultaneously, adipose tissue secretes an altered adipokine profile:
- ↑ Pro-inflammatory cytokines — TNF-α, IL-6, MCP-1 → chronic low-grade inflammation, endothelial dysfunction, and further insulin resistance.
- ↓ Adiponectin — reduced insulin-sensitising, anti-atherogenic, and anti-inflammatory effects.
- ↑ Resistin, retinol-binding protein 4 — additional mediators of insulin resistance.
Compensatory hyperinsulinaemia maintains euglycaemia initially but promotes: (1) renal sodium retention → hypertension; (2) hepatic lipogenesis → elevated triglycerides and small dense LDL; (3) suppression of lipoprotein lipase → low HDL-C; and (4) ovarian theca-cell androgen production → PCOS in women.
Over time, pancreatic β-cell exhaustion occurs, transitioning from impaired fasting glucose (IFG) through impaired glucose tolerance (IGT) to overt T2DM. The microbiome, epigenetic factors, sleep apnoea, physical inactivity, and genetic susceptibility (e.g., TCF7L2, FTO polymorphisms) modulate individual risk.
Clinical Implications & Cardiovascular Risk
MetS is independently associated with a 2–3-fold increased risk of cardiovascular events (myocardial infarction, stroke, cardiovascular death) and approximately 5-fold increased risk of developing T2DM (Ford et al., 2008; Mottillo et al., 2010). The relationship is continuous — even 1–2 components confer elevated risk, and the increment per additional component is non-linear.
| Outcome | Relative Risk (MetS vs. no MetS) | Population Attributable Fraction |
|---|---|---|
| CVD events (MI, stroke) | RR 2.0 (95% CI 1.5–2.7) | ~12% of CVD attributable to MetS |
| Type 2 diabetes | RR 5.0 (95% CI 3.6–7.1) | ~40% of T2DM cases preceded by MetS |
| NAFLD / NASH | RR 3.5 (95% CI 2.6–4.7) | >60% of MetS patients have NAFLD |
| CKD (eGFR <60 mL/min/1.73 m²) | RR 2.1 (95% CI 1.7–2.6) | Dose-response with number of components |
| Obstructive sleep apnoea | RR 2.8 (95% CI 2.1–3.7) | Bidirectional relationship with insulin resistance |
In Australian practice, use the Framingham Risk Score or Australian Absolute CVD Risk Calculator (NVDPA) to quantify 5-year and 10-year CVD risk. MetS should lower the threshold for initiating lipid-lowering and antihypertensive therapy. The RACGP Red Book recommends CVD risk assessment for all adults aged 45–74 years (35 years for Aboriginal and Torres Strait Islander peoples).
Management
Lifestyle Intervention (First-Line)
Structured lifestyle modification remains the most effective strategy, with NNT of 6.4 to prevent one case of T2DM over 3 years (Diabetes Prevention Programme). Components include:
- Weight loss: Target 5–10% of baseline body weight over 6–12 months. Even 3% loss significantly improves triglycerides and insulin sensitivity.
- Dietary pattern: Mediterranean-style or DASH diet preferred. Emphasise vegetables, fruits, wholegrains, legumes, nuts, olive oil, fish; reduce saturated fat (<10% energy), refined carbohydrates, sugary drinks, and excess alcohol (<10 standard drinks/week for women, <14 for men per NHMRC guidelines).
- Physical activity: ≥150 min/week moderate-intensity (brisk walking, cycling) or ≥75 min/week vigorous-intensity. Add resistance training ≥2 days/week.
- Behavioural support: Referral to dietitian (MBS 10954 — GPMP dietitian referral, up to 5 visits/year). Structured programmes such as Life! (Victoria) or My Health for Life (Queensland) are evidence-based.
- Smoking cessation: All patients who smoke should receive brief intervention and offer of NRT, varenicline, or bupropion.
Pharmacotherapy by Component
1. Hyperglycaemia / Insulin Resistance
2. Dyslipidaemia
3. Hypertension
Target <130/80 mmHg for patients with MetS and elevated CVD risk or diabetes (2016 Heart Foundation Guideline). For uncomplicated MetS: <140/90 mmHg.
Bariatric / Metabolic Surgery
Consider referral for bariatric surgery in patients with BMI ≥40 kg/m² or ≥35 kg/m² with MetS-related comorbidities (T2DM, obstructive sleep apnoea) who have not achieved adequate metabolic control with lifestyle and pharmacotherapy. Sleeve gastrectomy and Roux-en-Y gastric bypass both achieve 25–35% total body weight loss with durable MetS remission rates of 60–80% at 5 years. Assess suitability via a multidisciplinary metabolic clinic; waitlists are significant in the public system.
Monitoring & Follow-Up
Investigations
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Alberti KG, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation. 2009;120(16):1640-1645.
- 2. Dunstan DW, Zimmet PZ, Welborn TA, et al. The rising prevalence of diabetes and impaired glucose tolerance: the Australian Diabetes, Obesity and Lifestyle Study. Diabetes Care. 2002;25(5):829-834.
- 3. Ford ES, Li C, Sattar N. Metabolic syndrome and incident diabetes: current state of the evidence. Diabetes Care. 2008;31(9):1898-1904.
- 4. Mottillo S, Filion KB, Genest J, et al. The metabolic syndrome and cardiovascular risk: a systematic review and meta-analysis. J Am Coll Cardiol. 2010;56(14):1113-1132.
- 5. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework 2023 summary report. Canberra: AIHW; 2023.
- 6. National Vascular Disease Prevention Alliance (NVDPA). Absolute cardiovascular disease risk calculator. 2024. Available at: www.cvdcheck.org.au.
- 7. The Royal Australian College of General Practitioners (RACGP). Guidelines for preventive activities in general practice (Red Book). 10th ed. East Melbourne: RACGP; 2024.
- 8. Heart Foundation of Australia. Australian guideline for the diagnosis and management of hypertension in adults. Melbourne: National Heart Foundation of Australia; 2016.
- 9. Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes (EMPA-REG OUTCOME). N Engl J Med. 2015;373(22):2117-2128.
- 10. Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes (SUSTAIN-6). N Engl J Med. 2016;375(19):1834-1844.
- 11. Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and cardiovascular outcomes in obesity without diabetes (SELECT). N Engl J Med. 2024;390(24):2221-2232.
- 12. Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346(6):393-403.
- 13. KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. 2024;105(4S):S117-S314.
- 14. National Aboriginal Community Controlled Health Organisation (NACCHO). Framework for the delivery of Aboriginal and Torres Strait Islander primary health care services. Canberra: NACCHO; 2023.