📋 Key Information Summary
- PCOS affects approximately 8–13% of reproductive-age women in Australia, depending on the diagnostic criteria applied; prevalence rises to 20–30% when ultrasonography alone is used to define polycystic ovarian morphology.
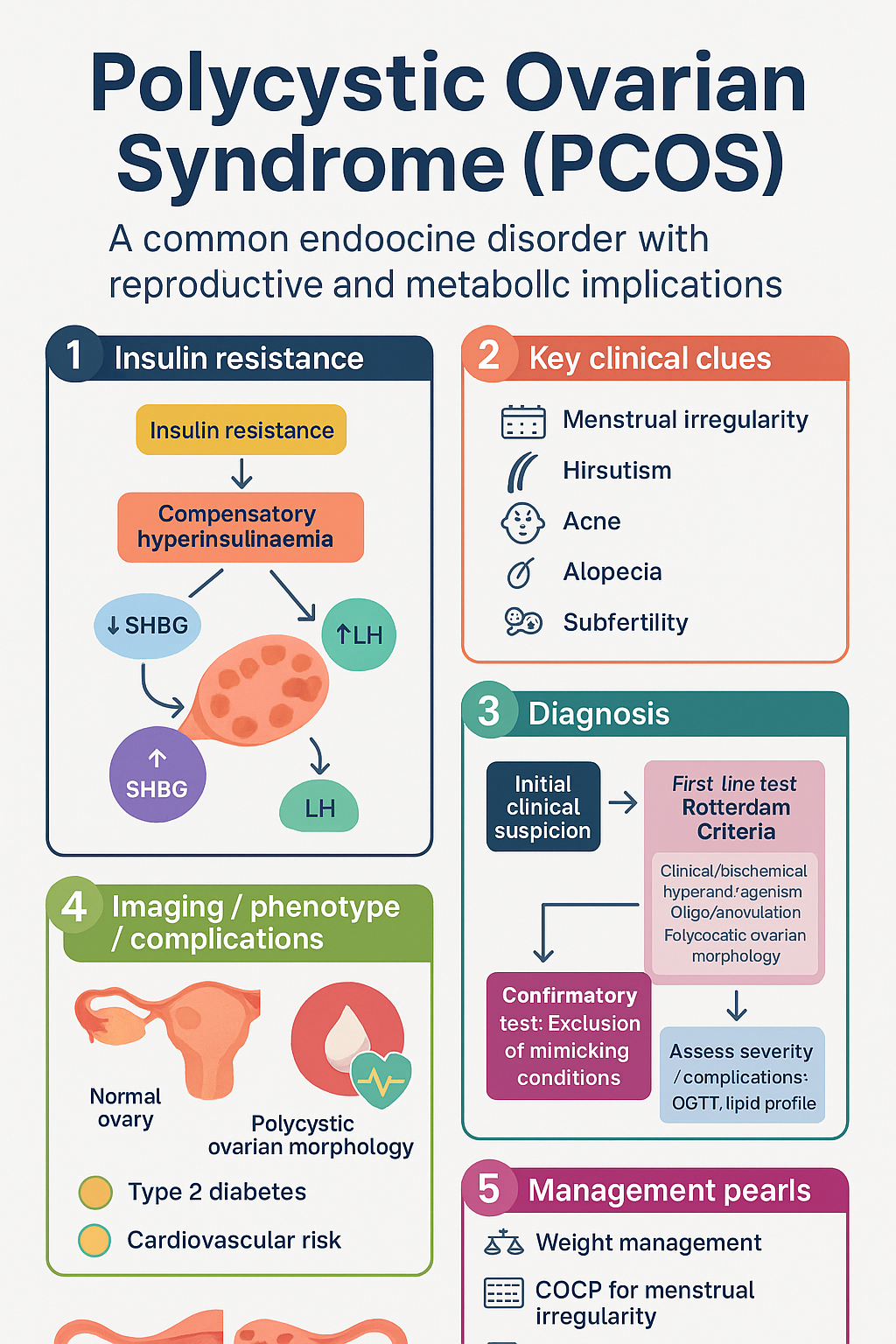
- Diagnosis requires ≥2 of the following Rotterdam Criteria: clinical/biochemical hyperandrogenism, oligo-anovulation (≤9 menses/year or cycles >35 days), and polycystic ovarian morphology on ultrasound (≥20 follicles per ovary or ovarian volume >10 mL).
- Exclusion of mimicking conditions (thyroid disease, hyperprolactinaemia, Cushing syndrome, late-onset congenital adrenal hyperplasia, androgen-secreting tumours) is mandatory before diagnosing PCOS.
- Insulin resistance and compensatory hyperinsulinaemia are central to PCOS pathophysiology and drive ovarian androgen excess.
- Clinical features include menstrual irregularity, hirsutism, acne, alopecia, and subfertility; metabolic complications include type 2 diabetes, dyslipidaemia, and cardiovascular risk.
- Screening for dysglycaemia (OGTT) is recommended every 1–3 years from age 30 (or at diagnosis if BMI >25) and annually if impaired glucose tolerance is present.
- Weight management with lifestyle modification is the first-line treatment regardless of presenting complaint; even 5–10% weight loss significantly improves metabolic and reproductive outcomes.
- Combined oral contraceptive pill (COCP) is first-line pharmacotherapy for menstrual irregularity and hyperandrogenism; levonorgestrel-ethinylestradiol preparations (such as Lenette-30ED®) are commonly used in Australia.
- Metformin (PBS-Listed) is considered second-line for metabolic features or when COCP is contraindicated; standard dose 500–2000 mg daily.
- Counselling regarding long-term metabolic and endometrial health is essential; unopposed oestrogen in oligomenorrhoeic women increases endometrial hyperplasia risk.
- Clomiphene citrate or letrozole are first-line ovulation induction agents for women with PCOS-related anovulatory subfertility; letrozole has superior live-birth rates per the NICE and ASRM guidelines.
- PCOS prevalence is higher in Aboriginal and Torres Strait Islander women, with greater metabolic complications and limited access to specialist care in remote settings.
🎧 Audio Brief
Introduction & Australian Epidemiology
Polycystic Ovarian Syndrome (PCOS) is the most common endocrine disorder in women of reproductive age, characterised by a triad of hyperandrogenism, oligo-anovulation, and polycystic ovarian morphology. The disorder is now recognised as a lifelong condition with metabolic, reproductive, and psychological implications that extend well beyond the reproductive years.
In Australia, prevalence estimates vary with the diagnostic criteria applied. Using the Rotterdam criteria, prevalence is approximately 8–13%, while the NIH 1990 criteria (which require both hyperandrogenism and oligo-anovulation) yield a lower prevalence of 6–8%. When ultrasonographic criteria alone are applied, prevalence may reach 20–30%, though many of these women may be asymptomatic. The Australian Longitudinal Study on Women's Health identified PCOS as a significant contributor to quality-of-life impairment, with affected women reporting higher rates of depression, anxiety, and body-image dissatisfaction.
PCOS carries substantial public-health significance: affected women have a 2–3-fold increased risk of type 2 diabetes mellitus (T2DM), up to 7-fold increased risk of impaired glucose tolerance, and elevated cardiovascular risk markers. Endometrial hyperplasia and endometrial carcinoma risk is increased 2.7–4-fold due to chronic unopposed oestrogen exposure in anovulatory women. PCOS is also the leading cause of anovulatory subfertility in Australia, accounting for approximately 70% of cases of ovulatory dysfunction.
This guideline follows the 2023 International Evidence-Based Guideline for the Assessment and Management of PCOS, adapted for Australian primary-care practice, and aligns with RACGP Red Book screening recommendations, Therapeutic Guidelines (eTG) pharmacological management, and PBS-listed medications.
Pathophysiology & Diagnosis (Rotterdam Criteria)
Pathophysiology
PCOS is a polygenic, multifactorial disorder with a complex interplay of genetic predisposition, epigenetic modifications, and environmental influences. The central pathophysiological driver is insulin resistance, present in 50–80% of women with PCOS (lean and overweight), leading to compensatory hyperinsulinaemia.
- Ovarian steroidogenesis: Hyperinsulinaemia acts synergistically with luteinising hormone (LH) to stimulate theca-cell production of androgens (androstenedione and testosterone). Insulin also suppresses hepatic sex hormone–binding globulin (SHBG), increasing bioavailable free testosterone.
- Hypothalamic–pituitary axis: Increased GnRH pulse frequency favours LH over FSH secretion (elevated LH:FSH ratio), perpetuating androgen excess and impairing folliculogenesis.
- Adipose tissue dysfunction: Visceral adiposity amplifies insulin resistance through adipokine dysregulation (increased TNF-α, IL-6; decreased adiponectin), contributing to chronic low-grade inflammation.
- Genetic & epigenetic factors: Twin studies demonstrate heritability of 50–70%. Candidate genes involve steroidogenesis (CYP11A1, CYP17), insulin signalling (INSR, IRS1), and androgen metabolism. In-utero androgen exposure may programme offspring to develop PCOS features through epigenetic mechanisms.
- Gut microbiome: Emerging evidence suggests reduced microbial diversity in PCOS, with altered bile-acid metabolism contributing to insulin resistance and inflammation.
Diagnostic Criteria — 2003 Rotterdam Consensus
Diagnosis requires the presence of at least 2 of 3 criteria, after excluding other causes of androgen excess or oligomenorrhoea:
| Rotterdam Criterion | Definition | Diagnostic Threshold |
|---|---|---|
| 1. Oligo-anovulation | Infrequent or absent ovulation | ≤9 menstrual cycles/year, or cycles >35 days |
| 2. Clinical and/or biochemical hyperandrogenism | Excess androgen signs or levels | Hirsutism (Ferriman–Gallwey ≥6), acne, alopecia; or total testosterone >2.0 nmol/L, free testosterone >35 pmol/L (lab-specific) |
| 3. Polycystic ovarian morphology (PCOM) | Characteristic ultrasound findings | ≥20 follicles per ovary (2–9 mm), or ovarian volume >10 mL (transvaginal ultrasound preferred) |
PCOS Phenotypes (AE-PCOS Society)
| Phenotype | Hyperandrogenism | Oligo-anovulation | PCOM | Metabolic Severity |
|---|---|---|---|---|
| A (Classic) | ✔ | ✔ | ✔ | Most severe |
| B (Classic) | ✔ | ✔ | – | Severe |
| C (Ovulatory) | ✔ | – | ✔ | Moderate |
| D (Non-hyperandrogenic) | – | ✔ | ✔ | Mildest |
Clinical Features & Complications
Reproductive Features
- Menstrual irregularity: Presenting symptom in 70–80% of adolescents and adults. Oligomenorrhoea (cycles >35 days) is most common; primary amenorrhoea may occur in severe phenotypes.
- Subfertility: Anovulation is the principal cause; cumulative fecundity per cycle without treatment is ~2% vs 15–20% in ovulatory women.
- Pregnancy complications: Increased rates of gestational diabetes (3-fold), pre-eclampsia, preterm birth, small- and large-for-gestational-age infants. Preconception counselling is essential.
Dermatological Features
- Hirsutism: Terminal hair growth in androgen-dependent areas (upper lip, chin, chest, abdomen, back, thighs). Assessed using the Ferriman–Gallwey modified score; ≥6 is abnormal. Affects 60–80% of women with PCOS.
- Acne: Inflammatory or comedonal acne, particularly adult-onset or treatment-resistant. Present in 20–35%.
- Androgenic alopecia: Female-pattern hair loss (frontal/vertex thinning); less common (5–15%) but psychologically impactful.
- Acanthosis nigricans: Hyperpigmented velvety plaques at neck, axillae, groin — a clinical marker of insulin resistance.
Metabolic Complications
Psychosocial & Psychological
- Depression (OR 3.8) and anxiety (OR 5.6) significantly more prevalent than age-matched controls.
- Body image disturbance, disordered eating (binge eating disorder prevalence ~10%), and sexual dysfunction.
- Routine psychological screening using PHQ-9 and GAD-7 is recommended at diagnosis and periodically thereafter.
Endometrial Hyperplasia & Carcinoma
Chronic anovulation leads to unopposed oestrogen stimulation of the endometrium, increasing risk of endometrial hyperplasia (up to 4-fold) and endometrial carcinoma (2.7-fold). Young women (<40 years) with endometrial cancer are disproportionately represented by PCOS. Progesterone withdrawal bleeds (e.g., cyclic medroxyprogesterone acetate 10 mg for 10–14 days each cycle) or COCP use is recommended to achieve at least 4 withdrawal bleeds per year.
Investigations
Investigations serve dual purposes: excluding differential diagnoses and assessing metabolic/complication burden. The following workup is recommended for all women with suspected PCOS.
Baseline Diagnostic Workup
Metabolic Surveillance Schedule
| Test | Frequency | When to Start |
|---|---|---|
| OGTT | Every 1–3 years | At diagnosis if BMI >25; otherwise from age 30 |
| Fasting lipids | Every 1–2 years | At diagnosis |
| HbA1c | Every 1–2 years | If OGTT impractical; not a substitute for OGTT if IGT screening is needed |
| BP & weight/BMI/waist | Annually | At every consultation |
| Liver function (NAFLD screening) | Every 1–2 years | If BMI >25 |
| Psychological screening (PHQ-9, GAD-7) | At diagnosis, then PRN | All patients at diagnosis |
Management
Management of PCOS is individualised based on the patient's presenting concerns, phenotype, metabolic risk, and fertility goals. A holistic, multidisciplinary approach addressing lifestyle, pharmacotherapy, and psychological wellbeing is recommended.
1. Lifestyle Modification (First-Line for All)
- Physical activity: ≥150 minutes moderate-intensity or ≥75 minutes vigorous-intensity activity per week, with muscle-strengthening activities on ≥2 days (aligns with Australian Physical Activity Guidelines).
- Dietary intervention: No single optimal diet is superior. Emphasis on sustainable caloric deficit if overweight/obese, Mediterranean-style dietary pattern, glycaemic index awareness, and dietary quality improvement. Referral to an Accredited Practising Dietitian is recommended.
- Behavioural strategies: Motivational interviewing, cognitive-behavioural approaches, and multidisciplinary team support improve adherence.
2. Pharmacotherapy for Menstrual Irregularity & Hyperandrogenism
First-Line: Combined Oral Contraceptive Pill (COCP)
Second-Line: Metformin
Adjunctive Anti-Androgen Therapy
3. Management of Hirsutism & Acne (Non-Hormonal)
- Eflornithine 13.9% cream (Vaniqa®): Topical application to face twice daily; reduces facial hair growth within 4–8 weeks. PBS Not Listed.
- Physical hair removal: Laser hair removal (alexandrite 755 nm or diode 810 nm) or IPL effective for terminal hair. 6–8 sessions required. Not PBS-listed.
- Topical retinoids & benzoyl peroxide: First-line for PCOS-related comedonal/inflammatory acne.
- Oral antibiotics: Doxycycline 50–100 mg PO daily or minocycline 50–100 mg PO daily for 3–6 months as bridge therapy for inflammatory acne while awaiting COCP effect.
4. Fertility & Ovulation Induction
Preconception optimisation (BMI <30 if possible, folic acid 5 mg daily, glycaemic control) should precede ovulation induction.
5. Endometrial Protection
Women with oligomenorrhoea or amenorrhoea not using COCP should achieve at least 4 withdrawal bleeds per year to reduce endometrial hyperplasia risk:
6. Intrauterine Device Option
Levonorgestrel intrauterine system (Mirena®) provides excellent endometrial protection and contraception without the systemic oestrogen exposure of COCP. Suitable for women with contraindications to oestrogen, obesity, or those who have completed fertility. Not recommended as first-line for hirsutism/acne management.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. International PCOS Network. 2023 International Evidence-Based Guideline for the Assessment and Management of Polycystic Ovary Syndrome. Human Reproduction. 2023;38(9):1655–1674.
- 2. Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertility and Sterility. 2004;81(1):19–25.
- 3. Boyle JA, Cunningham J, O'Dea K, Dunbar T, Norman RJ. Prevalence of polycystic ovary syndrome in a sample of Indigenous women from Darwin, Australia. Medical Journal of Australia. 2012;196(1):62–66.
- 4. Moran LJ, Hutchison SK, Norman RJ, Teede HJ. Lifestyle changes in women with polycystic ovary syndrome. Cochrane Database of Systematic Reviews. 2011;(2):CD007506.
- 5. Legro RS, Barnhart HX, Schlaff WD, et al. Clomiphene, metformin, or both for infertility in the polycystic ovary syndrome. New England Journal of Medicine. 2007;356(6):551–566.
- 6. Legro RS, Brzyski RG, Diamond MP, et al. Letrozole versus clomiphene for infertility in the polycystic ovary syndrome. New England Journal of Medicine. 2014;371(2):119–129.
- 7. National Institute for Health and Care Excellence (NICE). Fertility problems: assessment and treatment. NICE Guideline CG156. Updated 2017.
- 8. Royal Australian College of General Practitioners (RACGP). Guidelines for Preventive Activities in General Practice (Red Book). 9th edition. East Melbourne: RACGP; 2016.
- 9. Australian Institute of Health and Welfare (AIHW). Diabetes: Australian facts. Cat. no. CVD 54. Canberra: AIHW; 2014.
- 10. Teede HJ, Misso ML, Costello MF, et al. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Fertility and Sterility. 2018;110(3):364–379.
- 11. Azziz R, Carmina E, Dewailly D, et al. The Androgen Excess and PCOS Society (AES) position statement: assessment of the polycystic ovary syndrome in clinical practice. Fertility and Sterility. 2009;92(2):e27.
- 12. Lim SS, Davies MJ, Norman RJ, Moran LJ. Overweight, obesity and central obesity in women with polycystic ovary syndrome: a systematic review and meta-analysis. Human Reproduction Update. 2012;18(6):618–637.
- 13. Australian Government Department of Health. Physical Activity and Sedentary Behaviour Guidelines. Canberra: Commonwealth of Australia; 2019.
- 14. McCartney CR, Marshall JC. Polycystic ovary syndrome. New England Journal of Medicine. 2016;375(1):54–64.