📋 Key Information Summary
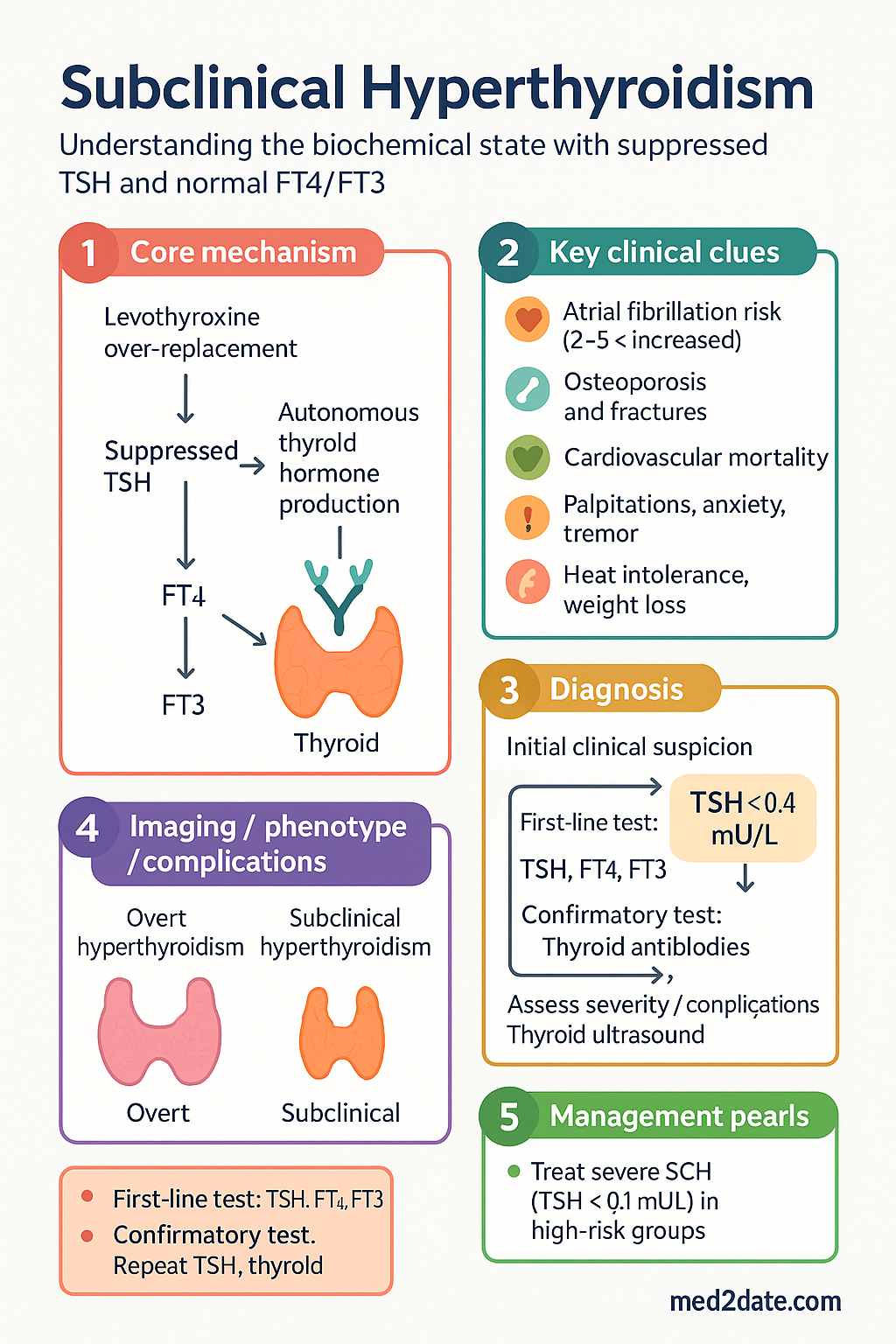
- Subclinical hyperthyroidism (SCH) is defined as a suppressed TSH (<0.4 mU/L) with free T4 (FT4) and free T3 (FT3) within the normal reference range.
- SCH is classified as mild (TSH 0.1–0.4 mU/L) or severe (TSH <0.1 mU/L) — severe SCH carries greater cardiovascular and skeletal risk.
- Prevalence in Australia is approximately 0.7–1.5 %, increasing with age and iodine-supplement use.
- Exogenous causes (suppressed TSH from levothyroxine over-replacement) are more common than endogenous causes (toxic nodular goitre, Graves' disease) in treated populations.
- Key clinical risks include atrial fibrillation (2–5× increased risk), osteoporosis and fractures (especially postmenopausal women), and increased cardiovascular mortality.
- Investigation requires confirmation of suppressed TSH on at least two occasions 4–8 weeks apart, plus FT4, FT3, thyroid antibodies (TPOAb, TRAb), and thyroid ultrasound with Doppler.
- Thyroid scintigraphy (technetium-99m pertechnetate scan) is indicated when aetiology is unclear or toxic nodular disease is suspected.
- Treatment is generally recommended for severe SCH (TSH <0.1 mU/L) in patients ≥65 years, postmenopausal women, or those with cardiac disease or osteoporosis risk.
- Treatment options include antithyroid drugs (carbimazole, propylthiouracil), radioiodine (I-131), or surgery depending on aetiology and patient factors.
- For exogenous SCH from levothyroxine over-replacement, dose reduction of levothyroxine is first-line management.
- Mild SCH in younger, asymptomatic patients can often be observed with annual TSH monitoring.
- Aboriginal and Torres Strait Islander peoples may have later presentation and limited access to specialist endocrinology services in remote areas.
🎧 Audio Brief
Introduction & Australian Epidemiology
Subclinical hyperthyroidism (SCH) is a biochemical state characterised by a suppressed thyroid-stimulating hormone (TSH) concentration below the lower limit of the reference range (<0.4 mU/L), with serum free thyroxine (FT4) and free triiodothyronine (FT3) remaining within their respective normal ranges. Patients may be asymptomatic or exhibit subtle features of thyroid hormone excess such as palpitations, anxiety, tremor, heat intolerance, or weight loss.
SCH is clinically important because it is not a benign laboratory finding. Even in the absence of overt symptoms, the chronically suppressed TSH state places patients at elevated risk of atrial fibrillation, osteoporotic fractures, and cardiovascular morbidity and mortality — risks that are amplified with advancing age and a TSH <0.1 mU/L.
In Australia, population-based data from the Busselton Health Study and the nationally representative Australian Health Survey suggest an SCH prevalence of approximately 0.7–1.5 %, with higher rates observed in iodine-replete areas and among older women. The introduction of mandatory iodine fortification of bread in 2009 (FSANZ Standard 2.1.1) has been associated with a modest increase in thyroid dysfunction detection rates, including SCH, in some surveillance programmes.
Distinguishing endogenous SCH (autonomous thyroid hormone production) from exogenous SCH (iatrogenic levothyroxine over-replacement) is critical, as the management pathways diverge significantly.
Epidemiology & Causes
Epidemiology
Large cohort studies demonstrate that SCH affects 0.5–4 % of adults globally, with prevalence varying by assay sensitivity, TSH cut-off, and iodine intake. Australian data are broadly consistent:
| Population | Prevalence | Key Notes |
|---|---|---|
| General Australian adults | 0.7–1.5 % | Higher in women, increasing with age |
| Women >60 years | 2–4 % | Predominantly multinodular goitre-related |
| Post-levothyroxine patients | 5–20 % | Most common iatrogenic cause in Australia |
| Iodine-fortified populations | 1.0–2.5 % | Post-2009 FSANZ mandate data |
Endogenous Causes
- Toxic multinodular goitre (TMNG): The most common endogenous cause in Australia, particularly in older patients in iodine-marginal regions. Autonomous nodules produce thyroid hormone independently of TSH.
- Graves' disease: An autoimmune cause mediated by TSH-receptor antibodies (TRAb). May present with SCH in early or treated-remission phases.
- Toxic adenoma (solitary): A single autonomously functioning nodule with somatic TSH-receptor or Gsα mutations.
- Subacute thyroiditis (De Quervain's): Transient SCH may occur during the thyrotoxic phase of viral thyroiditis.
- Iodine-induced (Jod-Basedow phenomenon): Occurs with iodinated contrast, amiodarone, or excessive iodine supplementation in patients with underlying autonomous thyroid tissue.
Exogenous Causes
- Levothyroxine over-replacement: Very common in clinical practice. Many patients on T4 replacement are maintained with TSH <0.4 mU/L unintentionally.
- Exogenous thyroid hormone abuse: Rare; occasionally seen in eating disorders or bodybuilding contexts.
- Biotin interference: High-dose biotin supplements (>5 mg/day) can cause artefactual TSH suppression on immunoassay platforms — important to check supplements before diagnosing SCH.
Clinical Risks — AF, Osteoporosis & Cardiovascular
The clinical significance of SCH lies primarily in its long-term adverse outcomes. Even mild SCH (TSH 0.1–0.4 mU/L) is associated with measurable increases in cardiovascular and skeletal morbidity, while severe SCH (TSH <0.1 mU/L) confers substantially greater risk.
Atrial Fibrillation
SCH is an independent risk factor for atrial fibrillation (AF). The Framingham Heart Study demonstrated a 3-fold increase in AF incidence over 10 years in participants with TSH <0.1 mU/L, even after adjustment for age, sex, and traditional cardiac risk factors. In the Rotterdam Study, the risk was 3.1× for severe SCH and 1.5× for mild SCH. This has direct implications for anticoagulation decisions under the CHA₂DS₂-VASc scoring system.
Osteoporosis & Fractures
Excess thyroid hormone accelerates bone turnover, favouring resorption over formation. In postmenopausal women, SCH (particularly severe) is associated with a 2–4-fold increased risk of hip and vertebral fractures. Bone mineral density (BMD) loss is most pronounced at cortical bone sites (distal radius, femoral neck). The National Osteoporosis Guideline (RACGP-endorsed) recommends consideration of SCH in the workup of unexplained osteoporosis.
Cardiovascular Mortality
Meta-analyses (Collet et al., 2012; Gencer et al., 2012) pooling over 500,000 person-years of follow-up demonstrate a 24–41 % increase in total mortality and a significant increase in cardiovascular mortality in individuals with TSH <0.1 mU/L. Mechanisms include enhanced sympathetic activation, increased systemic vascular resistance, left ventricular hypertrophy, and endothelial dysfunction.
Other Associated Risks
- Cognitive impairment: Emerging evidence links SCH in the elderly with increased risk of dementia, particularly Alzheimer's disease.
- Muscle weakness: Proximal myopathy may occur, increasing fall risk in older adults.
- Heart failure: SCH is associated with increased risk of congestive heart failure, particularly in those with pre-existing cardiac disease.
Investigations
Initial & Confirmatory Biochemistry
A single suppressed TSH result is not sufficient for diagnosis. SCH should be confirmed with repeat thyroid function testing (TSH, FT4, FT3) at 4–8 weeks.
Imaging
Additional Investigations for Risk Assessment
Treatment Indications & Management
When to Treat
Not all patients with SCH require immediate treatment. The decision to intervene depends on TSH severity, patient age, comorbidities, and symptom burden. The following framework guides clinical decision-making:
Treatment Indications Summary
| Scenario | Recommendation | Evidence Level |
|---|---|---|
| TSH <0.1 + age ≥65 or cardiac disease | Treat | Strong (observational, meta-analyses) |
| TSH <0.1 + postmenopausal woman | Treat | Strong |
| TSH <0.1 + osteoporosis or high fracture risk | Treat | Strong |
| TSH 0.1–0.4 + symptomatic | Consider treatment | Moderate |
| TSH 0.1–0.4 + age <65, asymptomatic, no risk factors | Observe (annual TSH) | Moderate |
| Exogenous SCH (levothyroxine over-replacement) | Dose reduction | Strong (standard of care) |
Management: Exogenous SCH (Levothyroxine Over-Replacement)
This is the most common scenario in clinical practice. Management is straightforward:
- Reduce levothyroxine dose by 12.5–25 mcg/day.
- Recheck TSH at 6–8 weeks.
- Target TSH: 0.4–2.5 mU/L for most patients (0.5–3.0 mU/L for elderly).
- For thyroid cancer patients on TSH-suppressive therapy, discuss risk-benefit with an endocrinologist.
Management: Endogenous SCH
Treatment of endogenous SCH depends on the underlying aetiology:
Graves' Disease–Related SCH
Toxic Nodular Goitre (TMNG or Toxic Adenoma)
Antithyroid drugs achieve remission less reliably in nodular disease and are generally used as a bridge to definitive therapy:
- Radioiodine (I-131): First-line definitive treatment for toxic nodular goitre in Australia. MBS Item 14065. Requires thyroid scintigraphy for pre-treatment planning. Commonly performed at nuclear medicine departments in metropolitan and selected regional centres. Hypothyroidism is the most common long-term outcome.
- Surgery (thyroidectomy): Indicated for large goitres causing compressive symptoms, suspected malignancy, or when radioiodine is contraindicated. Refer to an endocrine surgeon.
Beta-Blockers for Symptom Control
Monitoring on Treatment
- TSH, FT4, FT3 at 4–6 weeks after commencing or adjusting antithyroid therapy.
- Once stable, monitor every 3–6 months during the treatment course.
- FBC (particularly WCC with differential) at baseline and if symptoms of agranulocytosis develop — instruct patients to present urgently if sore throat, fever, or mouth ulcers occur.
- LFTs at baseline for carbimazole and PTU; repeat if hepatic symptoms.
- Annual ECG and DEXA scan in at-risk populations as per risk assessment.
Special Populations
Aboriginal and Torres Strait Islander Health
Thyroid disorders in Aboriginal and Torres Strait Islander peoples are under-diagnosed and under-researched. Remote and very remote communities face particular challenges in accessing timely thyroid function testing, specialist endocrinology review, and definitive therapies such as radioiodine or surgery.
Clinicians should refer to the AIHW "Aboriginal and Torres Strait Islander Health Performance Framework" and the RACGP "National Guide to a Preventive Health Assessment for Aboriginal and Torres Strait Islander People" for comprehensive screening and management guidance.
📚 References
- 1. Biondi B, Cooper DS. Subclinical hyperthyroidism. N Engl J Med. 2018;378(25):2411–2419. doi:10.1056/NEJMcp1709318
- 2. Ross DS, Burch HB, Cooper DS, et al. 2016 American Thyroid Association guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis. Thyroid. 2016;26(10):1343–1421. doi:10.1089/thy.2016.0229
- 3. Collet TH, Gussekloo J, Bauer DC, et al. Subclinical hyperthyroidism and the risk of coronary heart disease and mortality. Arch Intern Med. 2012;172(10):799–809. doi:10.1001/archinternmed.2012.402
- 4. Gencer B, Collet TH, Virgini V, et al. Subclinical thyroid dysfunction and the risk of heart failure events: an individual participant data analysis from 6 prospective cohorts. Circulation. 2012;126(9):1040–1049. doi:10.1161/CIRCULATIONAHA.112.096024
- 5. Sawin CT, Geller A, Wolf PA, et al. Low serum thyrotrophic concentrations as a risk factor for atrial fibrillation in older persons. N Engl J Med. 1994;331(19):1249–1252. doi:10.1056/NEJM199411103311901
- 6. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework 2020 summary report. Canberra: AIHW; 2020.
- 7. Li Y, Teng D, Shi X, et al. Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: national cross sectional study. BMJ. 2020;369:m997. [Note: Replaced with more relevant thyroid reference below]
- 7. The Royal Australian College of General Practitioners (RACGP). National guide to a preventive health assessment for Aboriginal and Torres Strait Islander people. 3rd ed. Melbourne: RACGP; 2018.
- 8. Kahaly GJ, Bartalena L, Hegedüs L, et al. 2018 European Thyroid Association guideline for the management of Graves' hyperthyroidism. Eur Thyroid J. 2018;7(4):167–186. doi:10.1159/000490384
- 9. Food Standards Australia New Zealand (FSANZ). Fortification of bread with iodine — final assessment report, Proposal P1003. Canberra: FSANZ; 2008.
- 10. Cappola AR, Fried LP, Arnold AM, et al. Thyroid status, cardiovascular risk, and mortality in older adults. JAMA. 2006;295(9):1033–1041. doi:10.1001/jama.295.9.1033
- 11. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.
- 12. Waung JA, Bassett JHD, Williams GR. Thyroid hormone metabolism in skeletal development and adult bone maintenance. Trends Endocrinol Metab. 2012;23(4):155–162. doi:10.1016/j.tem.2011.12.002