📋 Key Information Summary
- Amiodarone-induced thyrotoxicosis (AIT) develops in 2–12% of patients on amiodarone in iodine-replete populations such as Australia.
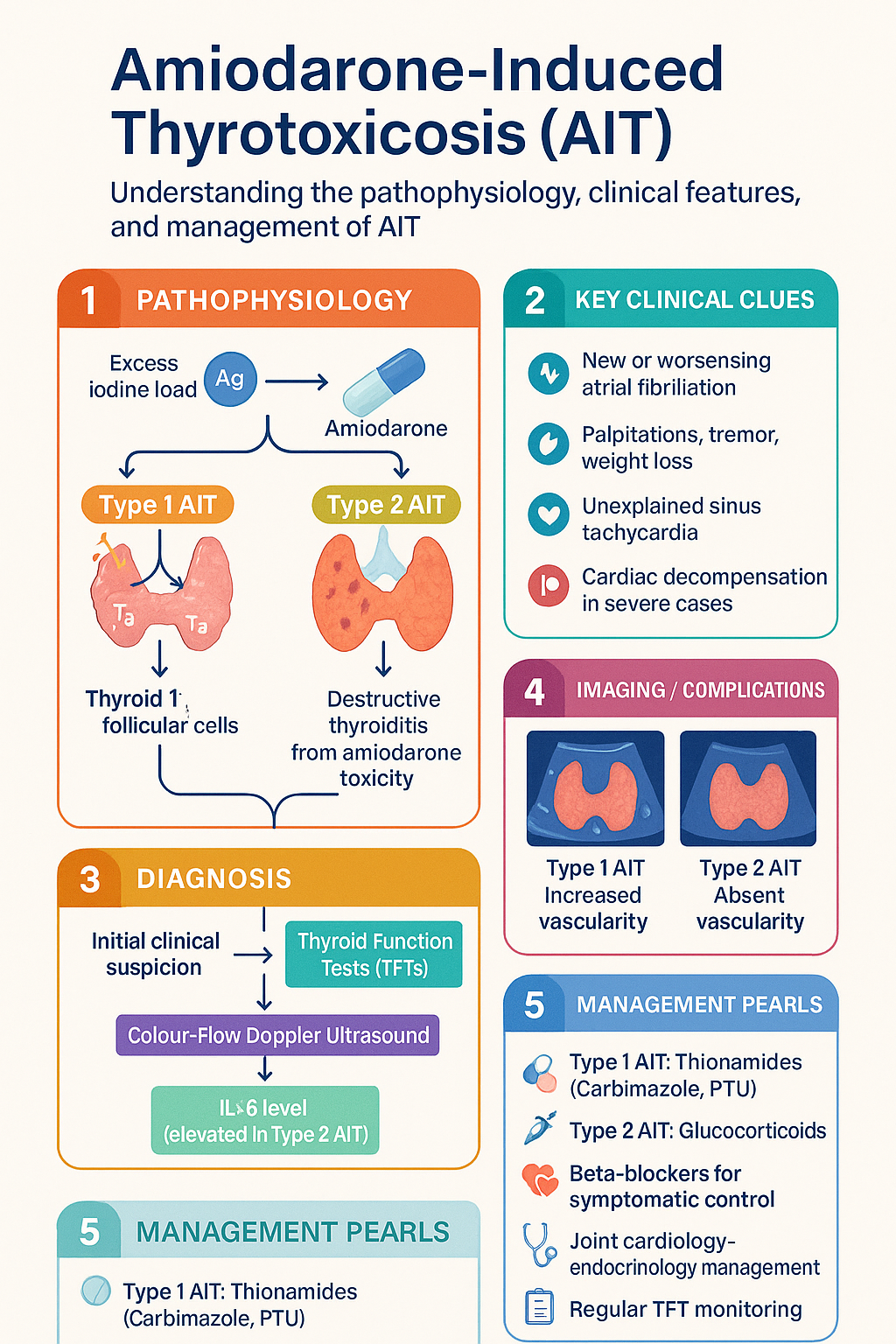
- Two distinct subtypes: Type 1 AIT (excess iodine-driven synthesis in a pre-existing thyroid abnormality) and Type 2 AIT (destructive thyroiditis from direct amiodarone toxicity).
- Type 1 AIT is more common in iodine-deficient regions; Type 2 AIT predominates in iodine-sufficient countries including Australia.
- Mixed-type AIT exists and can be difficult to classify; treat with combination thionamide plus glucocorticoid therapy.
- Colour-flow Doppler ultrasound and interleukin-6 (IL-6) levels are the most useful adjunctive investigations to differentiate Type 1 from Type 2 AIT.
- Thionamides (carbimazole or propylthiouracil) are first-line for Type 1 AIT; glucocorticoids are first-line for Type 2 AIT.
- High-dose potassium perchlorate (short-term ≤6 weeks) may be added to thionamides in Type 1 AIT to block iodide uptake.
- Radioactive iodine (RAI) uptake is generally too low in AIT to be effective; RAI is rarely used.
- Thyroidectomy may be required in refractory cases but carries high peri-operative risk; expert multidisciplinary planning is essential.
- Beta-blockers (preferably propranolol) should be initiated early for symptomatic rate control unless contraindicated.
- Continuation of amiodarone must be weighed against the haemodynamic risk of stopping anti-arrhythmic therapy — a joint cardiology–endocrinology decision.
- All patients commencing amiodarone should have baseline TFTs and 6-monthly monitoring for at least 12 months after cessation (amiodarone has a half-life of 40–55 days).
- Aboriginal and Torres Strait Islander patients face barriers to specialist endocrinology access in remote areas; telehealth and RFDS-supported pathways should be utilised.
🎧 Audio Brief
Introduction & Australian Epidemiology
Amiodarone is a Class III anti-arrhythmic agent widely prescribed in Australia for atrial fibrillation, ventricular tachycardia and heart failure with reduced ejection fraction. Despite its efficacy, amiodarone carries a significant burden of thyroid-related adverse effects owing to two unique pharmacological properties: an exceptionally high iodine content (37% by weight; a single 200 mg tablet delivers approximately 7 mg of inorganic iodide, roughly 45 times the recommended daily intake) and a direct cytotoxic effect on thyroid follicular cells.
Thyroid dysfunction develops in 14–18% of amiodarone-treated patients, split broadly into hypothyroidism (5–10%) and thyrotoxicosis (2–12%). In Australia, where dietary iodine intake is generally adequate (median urinary iodine concentration 100–199 µg/L), amiodarone-induced thyrotoxicosis (AIT) is encountered less frequently than in iodine-deficient regions but remains an important clinical problem because it can precipitate or worsen life-threatening arrhythmias and heart failure.
AIT may present months to years after commencing amiodarone, and may even arise after drug cessation due to the prolonged tissue half-life of 40–55 days (up to 100 days in adipose tissue). Recognition and appropriate subtype classification are critical because the two forms of AIT require fundamentally different treatment strategies. Misclassification can lead to clinical deterioration and excess mortality, which ranges from 3–10% in published series.
Mechanisms: Type 1 vs Type 2 AIT
Understanding the pathophysiological distinction between Type 1 and Type 2 AIT is essential for selecting appropriate therapy. The two subtypes arise from fundamentally different mechanisms, although overlap (mixed-type AIT) is recognised.
Type 1 AIT — Jod–Basedow Phenomenon
Type 1 AIT results from the iodine load provided by amiodarone acting upon a thyroid gland with a pre-existing abnormality — most commonly multinodular goitre, latent Graves' disease or autonomous nodules. The high iodine supply overwhelms the normal Wolff–Chaikoff autoregulatory escape mechanism, permitting autonomous synthesis and release of thyroid hormones. This is termed the Jod–Basedow (iodine-induced) effect.
- More prevalent in areas of prior iodine deficiency (central Europe, parts of South-East Asia).
- Thyroid gland may be enlarged or nodular on examination.
- Radioactive iodine uptake (RAIU) may be low-normal or reduced, but typically >4% (unlike Type 2).
- Colour-flow Doppler ultrasound shows increased vascularity.
- Responds to thionamides, which block new hormone synthesis.
Type 2 AIT — Destructive Thyroiditis
Type 2 AIT is a drug-induced destructive thyroiditis caused by direct cytotoxic effects of amiodarone and its metabolite desethylamiodarone on thyroid follicular cells. Stored pre-formed thyroid hormones are released into the circulation as cells undergo necrosis and apoptosis. There is no new hormone synthesis.
- More prevalent in iodine-sufficient regions, including Australia.
- Thyroid gland is typically normal-sized and non-tender.
- RAIU is markedly suppressed (typically <4%) due to maximal Wolff–Chaikoff effect.
- Colour-flow Doppler ultrasound shows absent or markedly reduced vascularity.
- Responds to glucocorticoids, which suppress inflammation and hormone release.
Summary Comparison
| Feature | Type 1 AIT | Type 2 AIT |
|---|---|---|
| Mechanism | Excess iodine → new hormone synthesis | Destructive thyroiditis → hormone release |
| Pre-existing thyroid disease | Usually present (MNG, latent Graves') | Usually absent |
| Thyroid gland size | Normal or enlarged / nodular | Normal |
| Colour-flow Doppler | Increased vascularity | Absent / markedly reduced vascularity |
| RAIU | Low-normal or reduced (>4%) | Markedly suppressed (<4%) |
| IL-6 | Normal or mildly elevated | Markedly elevated |
| First-line therapy | Thionamides | Glucocorticoids |
| Outcome after amiodarone withdrawal | May persist for months | Usually self-limited (weeks to months) |
Clinical Features & Investigations
Clinical Presentation
The presentation of AIT is often insidious and may be masked by the beta-blocking properties of amiodarone. Classical symptoms and signs of thyrotoxicosis may be attenuated or absent. A high index of clinical suspicion is therefore essential.
- New or worsening atrial fibrillation / flutter — the most common presenting arrhythmia.
- Recurrent ventricular tachycardia or worsening heart failure in a previously stable patient.
- Palpitations, tremor, heat intolerance, weight loss — may be blunted by amiodarone's adrenergic blockade.
- Unexplained sinus tachycardia or increased ventricular rate on telemetry.
- In severe cases: cardiac decompensation, angina, myocardial infarction.
- Type 2 AIT may present with mild neck discomfort or tenderness; Type 1 is typically painless.
Investigations
Differentiation of AIT Types
Accurate subtype classification is critical because Type 1 and Type 2 AIT require different pharmacological approaches. No single investigation is diagnostic; a combination of clinical, biochemical and imaging features should be used.
Differentiating Algorithm
Severity Assessment
Management
Management of AIT requires a dual strategy: controlling the hyperthyroid state and addressing the underlying arrhythmia or cardiac indication for amiodarone. Joint cardiology–endocrinology input is strongly recommended for all cases.
General Measures (All AIT Types)
- Beta-blockade: Initiate propranolol for symptomatic control. If propranolol is contraindicated (severe asthma, decompensated heart failure), consider atenolol or metoprolol. Note: amiodarone's intrinsic beta-blocking effect may limit titration.
- Amiodarone continuation: A joint decision with cardiology. If the arrhythmia is life-threatening and no alternative anti-arrhythmic is suitable, amiodarone should be continued with aggressive treatment of the thyrotoxicosis. If safe to cease, amiodarone withdrawal alone will not rapidly resolve AIT due to prolonged tissue half-life.
- Anticoagulation: Reassess stroke risk if AF/Flutter is present. Treated as per standard AF guidelines (CHA₂DS₂-VASc score).
- Monitor closely: TFTs every 2–4 weeks until euthyroid, then 6–8 weekly during treatment. ECG monitoring in hospitalised patients.
Type 1 AIT — Pharmacotherapy
The goal is to block new thyroid hormone synthesis. High doses of thionamides are typically required because the iodine excess saturates the organification pathway.
Type 2 AIT — Pharmacotherapy
The goal is to suppress inflammation and reduce the release of pre-formed thyroid hormone. Glucocorticoids are the mainstay.
Propranolol — Symptomatic Control (All Types)
Mixed-Type / Refractory AIT
- Combined thionamide (carbimazole 40 mg/day) plus glucocorticoid (prednisone 40 mg/day) therapy is recommended when the subtype is unclear or features of both types are present.
- Reassess at 4 weeks. If FT4 is falling, continue current regimen. If not, consider addition of potassium perchlorate (Type 1 component) or escalation of glucocorticoid dose (Type 2 component).
- Plasmapheresis or plasma exchange has been reported in life-threatening refractory AIT to acutely lower circulating thyroid hormones. Available at major tertiary centres (e.g., Royal Melbourne, St Vincent's Sydney, Royal Adelaide). Consider in ICU patients with haemodynamic instability not responding to medical therapy.
Thyroidectomy
Thyroidectomy may be necessary for patients with refractory AIT who cannot be rendered euthyroid despite maximal medical therapy, or when amiodarone cannot be withdrawn and continued AIT poses unacceptable cardiac risk.
Quick Reference — Treatment by AIT Type
Monitoring
Monitoring during and after treatment of AIT is essential due to the prolonged tissue half-life of amiodarone and the risk of relapse or transition to hypothyroidism.
Special Populations
Aboriginal and Torres Strait Islander Health
📚 References
- 1. Martino E, Bartalena L, Bogazzi F, Braverman LE. The effects of amiodarone on the thyroid. Endocrine Reviews. 2001;22(2):240–254.
- 2. Basaria S, Cooper DS. Amiodarone and the thyroid. The American Journal of Medicine. 2005;118(7):706–714.
- 3. Bartalena L, Brogioni S, Grasso L, Bogazzi F, Burelli A, Martino E. Treatment of amiodarone-induced thyrotoxicosis, a difficult challenge: results of a prospective study. Journal of Clinical Endocrinology & Metabolism. 1996;81(8):2930–2933.
- 4. Bogazzi F, Bartalena L, Martino E. Approach to the patient with amiodarone-induced thyrotoxicosis. Journal of Clinical Endocrinology & Metabolism. 2011;96(5):1207–1213.
- 5. Ross DS, Burch HB, Cooper DS, et al. 2016 American Thyroid Association guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis. Thyroid. 2016;26(10):1343–1421.
- 6. Kahaly GJ, Bartalena L, Hegedüs L, Leenhardt L, Poppe K, Pearce SH. 2018 European Thyroid Association guideline for the management of Graves' hyperthyroidism. European Thyroid Journal. 2018;7(4):167–186.
- 7. Australian Institute of Health and Welfare (AIHW). Cardiovascular disease in Aboriginal and Torres Strait Islander people. Cat. no. CVD 88. Canberra: AIHW; 2022.
- 8. Tomisti L, Rossi G, Bartalena L, et al. The onset time of amiodarone-induced thyrotoxicosis (AIT) depends on AIT type. European Journal of Endocrinology. 2014;171(3):363–368.
- 9. Royal Australian College of General Practitioners (RACGP). Management of thyroid disorders in general practice. Australian Family Physician. 2017;46(11):810–816.
- 10. Tsang W, Houlden RL. Amiodarone-induced thyrotoxicosis: a review. Canadian Journal of Cardiology. 2009;25(8):421–424.
- 11. Eskes SA, Endert E, Fliers E, et al. Treatment of amiodarone-induced thyrotoxicosis with plasmapheresis. Annals of Internal Medicine. 2012;156(10):725–726.
- 12. National Health and Medical Research Council (NHMRC). Iodine supplementation for pregnant and breastfeeding women. NHRMC Public Statement. Canberra: NHMRC; 2010.