📋 Key Information Summary
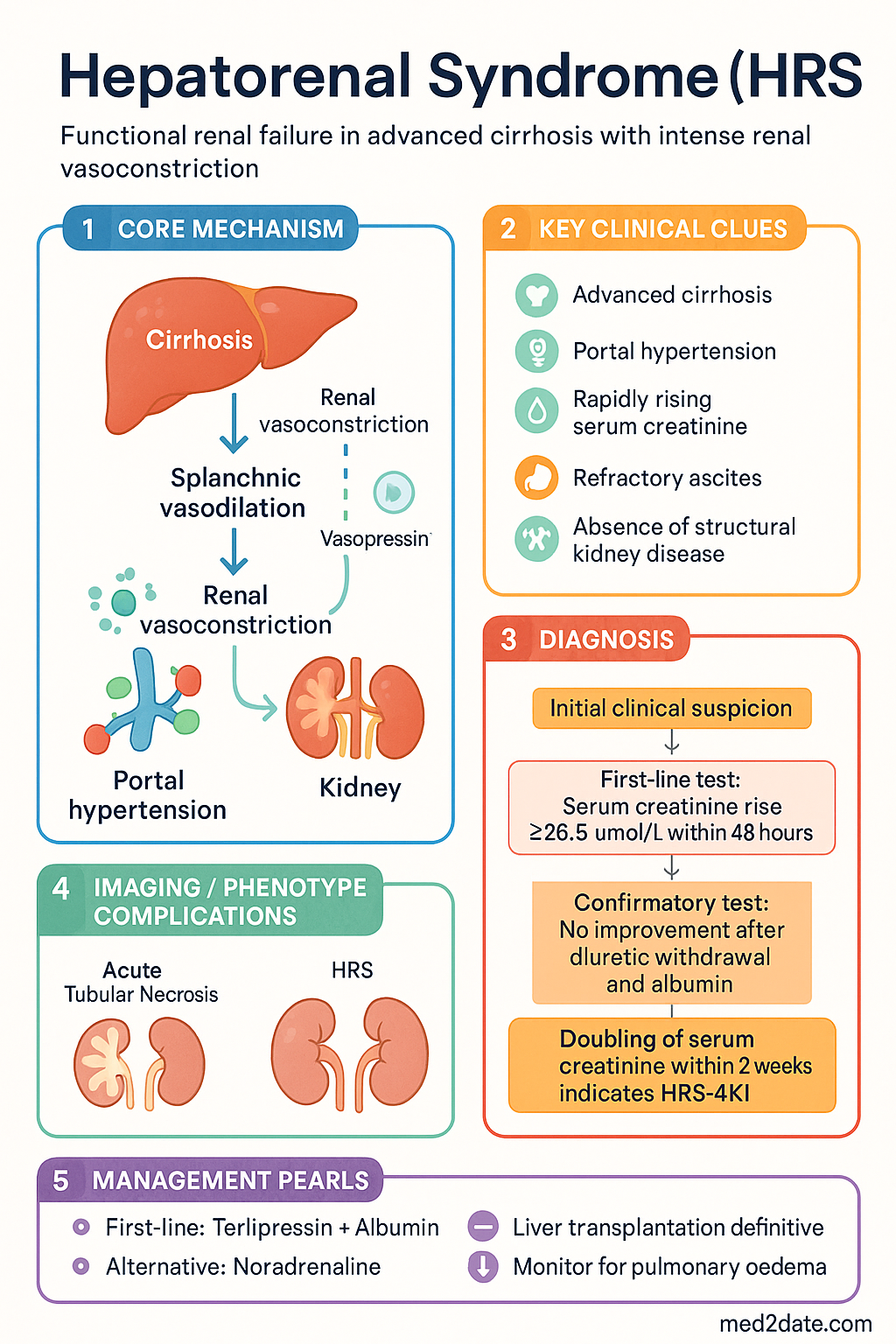
- Hepatorenal syndrome (HRS) is a functional renal failure occurring in patients with advanced cirrhosis and portal hypertension, characterised by intense renal vasoconstriction in the absence of structural kidney disease.
- Diagnosis requires ICA-AKI criteria: serum creatinine rise ≥26.5 µmol/L within 48 hours or ≥50% increase within 7 days, after exclusion of shock, nephrotoxic drugs, hypovolaemia, and structural kidney injury.
- A mandatory 48-hour diagnostic trial of diuretic withdrawal and volume expansion with albumin (1 g/kg/day, max 100 g/day for 2 days) is required before confirming HRS; failure to improve confirms functional renal failure.
- HRS-AKI (formerly type 1) is rapidly progressive with doubling of serum creatinine within 2 weeks; HRS-NAKI (formerly type 2) is slower and associated with refractory ascites.
- First-line vasoconstrictor therapy is terlipressin (bolus 1–2 mg IV 4–6 hourly, or continuous infusion 2–12 mg/day) combined with intravenous albumin (20–40 g/day after initial challenge); this is PBS-listed (Authority Required).
- Where terlipressin is unavailable or contraindicated, noradrenaline 0.5–3 mg/hr continuous IV infusion plus albumin in an ICU setting is an evidence-based alternative.
- Midodrine 7.5–12.5 mg PO TDS + octreotide 100–200 µg SC TDS + albumin is a second-line option where intravenous vasoconstrictors cannot be used.
- NSAIDs, ACE inhibitors, ARBs, and aminoglycosides must be avoided as they precipitate or worsen HRS.
- Liver transplantation is the only definitive treatment; simultaneous liver–kidney transplant is considered for patients with dialysis dependence ≥6 weeks or pre-existing CKD stage 4–5.
- Renal replacement therapy is indicated only as a bridge to transplantation in suitable candidates; outcomes are significantly worse if transplanted while on RRT.
- Aboriginal and Torres Strait Islander Australians have a disproportionately higher burden of liver disease and cirrhosis; timely specialist referral and culturally safe care pathways are essential.
- Terlipressin carries risk of pulmonary oedema (especially in patients with cardiac dysfunction) and digital/peripheral ischaemia; careful volume status monitoring is mandatory.
- Serum lactate, serum sodium, and bilirubin are important prognostic markers and guide transplant listing urgency.
🎧 Audio Brief
Introduction & Australian Epidemiology
Hepatorenal syndrome (HRS) is a life-threatening complication of end-stage liver disease, defined as functional renal failure due to profound renal vasoconstriction in the setting of portal hypertension and splanchnic vasodilation. The kidneys in HRS are structurally normal; dysfunction is haemodynamic, and renal histology is typically unremarkable on biopsy.
HRS develops in approximately 18–40% of patients hospitalised with decompensated cirrhosis. In Australia, cirrhosis is the 11th leading cause of death overall, with rising incidence driven by increasing rates of metabolic dysfunction-associated steatohepatitis (MASH), harmful alcohol use, and chronic hepatitis B and C. The AIHW reports that liver disease mortality has increased by approximately 28% over the past decade, disproportionately affecting Aboriginal and Torres Strait Islander peoples and rural communities.
In Australian tertiary centres, HRS-AKI carries an untreated 2-week mortality exceeding 80%. Even with vasoconstrictor therapy, 30-day mortality remains 20–50%, underscoring the urgency of early recognition and the critical role of timely liver transplant assessment.
Diagnosis
ICA-AKI Criteria in Cirrhosis
The International Club of Ascites (ICA) revised criteria require AKI staging based on serum creatinine changes from baseline:
| AKI Stage | Serum Creatinine Criteria |
|---|---|
| Stage 1 | Increase ≥26.5 µmol/L within 48 hours or ≥50% increase from baseline within 7 days |
| Stage 2 | Increase ≥2× baseline creatinine |
| Stage 3 | Increase ≥3× baseline or serum creatinine ≥353.6 µmol/L or initiation of RRT |
Diagnostic Criteria for HRS
Diagnosis of HRS is one of exclusion. All of the following must be fulfilled:
- Cirrhosis with ascites (documented by imaging or paracentesis)
- AKI per ICA-AKI Stage 1 or above
- No improvement of serum creatinine after at least 2 days of diuretic withdrawal and volume expansion with albumin (1 g/kg/day IV, maximum 100 g/day, for 2 days)
- Absence of shock (no haemodynamic instability requiring vasopressors)
- No current or recent nephrotoxic drug exposure (NSAIDs, aminoglycosides, IV contrast within prior 48–72 hours)
- No macroscopic signs of structural kidney disease:
- Urine red blood cells <50 per high-power field
- Urine protein <500 mg/day (or urine protein:creatinine ratio <500 mg/g)
- Normal renal ultrasound (no hydronephrosis, no cortical thinning)
- No sustained reversal with volume expansion alone
Differential Diagnosis of AKI in Cirrhosis
| Aetiology | Distinguishing Features | Response to Volume |
|---|---|---|
| Pre-renal (hypovolaemia) | Diarrhoea, haemorrhage, over-diuresis; low CVP | Yes — improves with albumin/crystalloid |
| Acute tubular necrosis (ATN) | Muddy brown granular casts, high FeNa (>2%), prior shock/ischaemia | No |
| Hepatorenal syndrome | Low urine sodium (<10 mEq/L), low FeNa (<1%), bland urine sediment | No — functional renal failure |
| Nephrotoxic injury | NSAIDs, aminoglycosides, IV contrast history | No |
| Intrinsic glomerulonephritis | Active urine sediment, proteinuria >500 mg/day, haematuria | No — requires renal biopsy |
Investigations
Classification & Treatment
Classification
First-Line Vasoconstrictor Therapy: Terlipressin + Albumin
Alternative Vasoconstrictor Regimens
Medications to Avoid in Cirrhosis with Suspected/Acute HRS
- NSAIDs (ibuprofen, naproxen, diclofenac) — inhibit renal prostaglandin synthesis, precipitate AKI
- ACE inhibitors and ARBs — abolish compensatory angiotensin-II-mediated renal efferent arteriolar tone, causing precipitous GFR decline
- Aminoglycosides (gentamicin, tobramycin) — high nephrotoxicity risk in cirrhosis; avoid if any alternative exists
- IV contrast — minimise exposure; if essential, pre-hydrate with normal saline and use low-osmolar or iso-osmolar agents only
- Lactulose in excessive doses — can cause volume depletion and prerenal azotaemia
Definitive Therapy
Liver Transplantation
Liver transplantation is the only definitive treatment for HRS, restoring portal haemodynamics and reversing the splanchnic vasodilation that drives renal vasoconstriction. All patients with confirmed HRS should be assessed for transplant candidacy at the earliest opportunity.
- HRS with recovery on vasoconstrictors: Transplant outcomes approach those of non-HRS patients; renal function often recovers fully post-transplant.
- HRS without recovery (persistent AKI on RRT): Consider simultaneous liver–kidney transplant (SLK) if renal failure duration ≥6 weeks on RRT, or pre-existing CKD stage 4–5 (eGFR <30 mL/min for ≥90 days).
- SLK rates in Australia are determined by state-based organ allocation services (DonateLife, Transplant Australia). Transplant centres include Royal Prince Alfred (Sydney), Austin Health (Melbourne), Princess Alexandra (Brisbane), Sir Charles Gairdner (Perth), and Flinders Medical Centre (Adelaide).
- MELD and MELD-Na scores drive transplant listing priority. HRS patients with hyponatraemia often have very high MELD-Na scores, supporting earlier listing.
Renal Replacement Therapy (RRT)
Key considerations for RRT in HRS:
- Continuous renal replacement therapy (CRRT) is preferred over intermittent haemodialysis due to better haemodynamic tolerance in cirrhotic patients.
- Anticoagulation: regional citrate anticoagulation is preferred; avoid systemic heparin in patients with coagulopathy or active variceal risk.
- Outcomes are significantly worse for patients transplanted while on RRT compared to those transplanted before RRT initiation — this underscores the importance of early vasoconstrictor therapy to prevent progression to dialysis dependence.
- Peritoneal dialysis is occasionally used in stable patients but carries high infection risk in ascitic patients.
Emerging Therapies & Evolving Evidence
The therapeutic landscape for HRS is evolving rapidly:
- Terlipressin — CONFIRM trial (2021): Established terlipressin + albumin superiority over albumin alone for HRS-AKI reversal, but with a signal of increased respiratory failure risk. Subsequent real-world analyses have refined patient selection (avoid in patients with significant pulmonary or cardiac comorbidities).
- Serelaxin: A recombinant relaxin-2 analogue showing promise in early-phase trials for HRS via renal vasodilation; Phase III data pending.
- Iptacopan and other complement inhibitors: Under investigation for complement-mediated kidney injury in ACLF-associated HRS; early-phase only.
- Artificial liver support systems (e.g., MARS, Prometheus): May reduce bilirubin and ammonia but have not demonstrated survival benefit in HRS specifically; used as bridging in some European and select Australian centres.
- Refined SLK criteria: Ongoing debate regarding the duration of RRT required before SLK listing (6-week rule); some centres now advocate earlier SLK for patients with irreversible kidney injury markers (e.g., kidney biopsy showing >30% interstitial fibrosis).
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Angeli P, Ginès P, Wong F, et al. Diagnosis and management of acute kidney injury in patients with cirrhosis: revised consensus recommendations of the International Club of Ascites. Gut. 2015;64(4):531–537.
- 2. European Association for the Study of the Liver. EASL Clinical Practice Guidelines on the management of decompensated cirrhosis. J Hepatol. 2023;79(2):406–460.
- 3. Wong F, Pappas SC, Curry MP, et al. Terlipressin plus albumin for the treatment of type 1 hepatorenal syndrome (CONFIRM trial). N Engl J Med. 2021;384(9):818–828.
- 4. Nadim MK, Kellum JA, Davenport A, et al. Hepatorenal syndrome: the 8th International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care. 2012;16(1):R23.
- 5. Piano S, Schmidt HH, Ariza X, et al. Association between grade of acute on chronic liver failure and response to terlipressin and albumin in patients with hepatorenal syndrome. Clin Gastroenterol Hepatol. 2018;16(11):1792–1800.e3.
- 6. Singh V, Ghosh S, Singh B, et al. Noradrenaline vs terlipressin in the treatment of hepatorenal syndrome: a randomized study. J Hepatol. 2012;56(6):1293–1298.
- 7. Australian Institute of Health and Welfare. Liver and biliary disease in Australia. AIHW; 2023. Cat. no. PHE 319.
- 8. Biggins SW, Angeli P, Garcia-Tsao G, et al. Diagnosis, evaluation, and management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome: 2021 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology. 2021;74(2):1014–1048.
- 9. Nadim MK, Durand F, Kellum JA, et al. Management of the critically ill patients with cirrhosis: a multidisciplinary perspective. J Hepatol. 2016;64(3):717–735.
- 10. RHDAustralia (Northern Territory Department of Health). Australian guidelines for the management of hepatitis B in Aboriginal and Torres Strait Islander peoples. 3rd ed. Darwin: RHDAustralia; 2022.
- 11. Kribben A, Gerken G, Haag S, et al. Effects of fractionated plasma separation and adsorption on survival in patients with acute-on-chronic liver failure (HELIOS study): a randomised controlled trial. Lancet. 2012;379(9816):309–316.
- 12. Australian Commission on Safety and Quality in Health Care. National Safety and Quality Health Service Standards. 2nd ed. ACSQHC; 2021.