📋 Key Information Summary
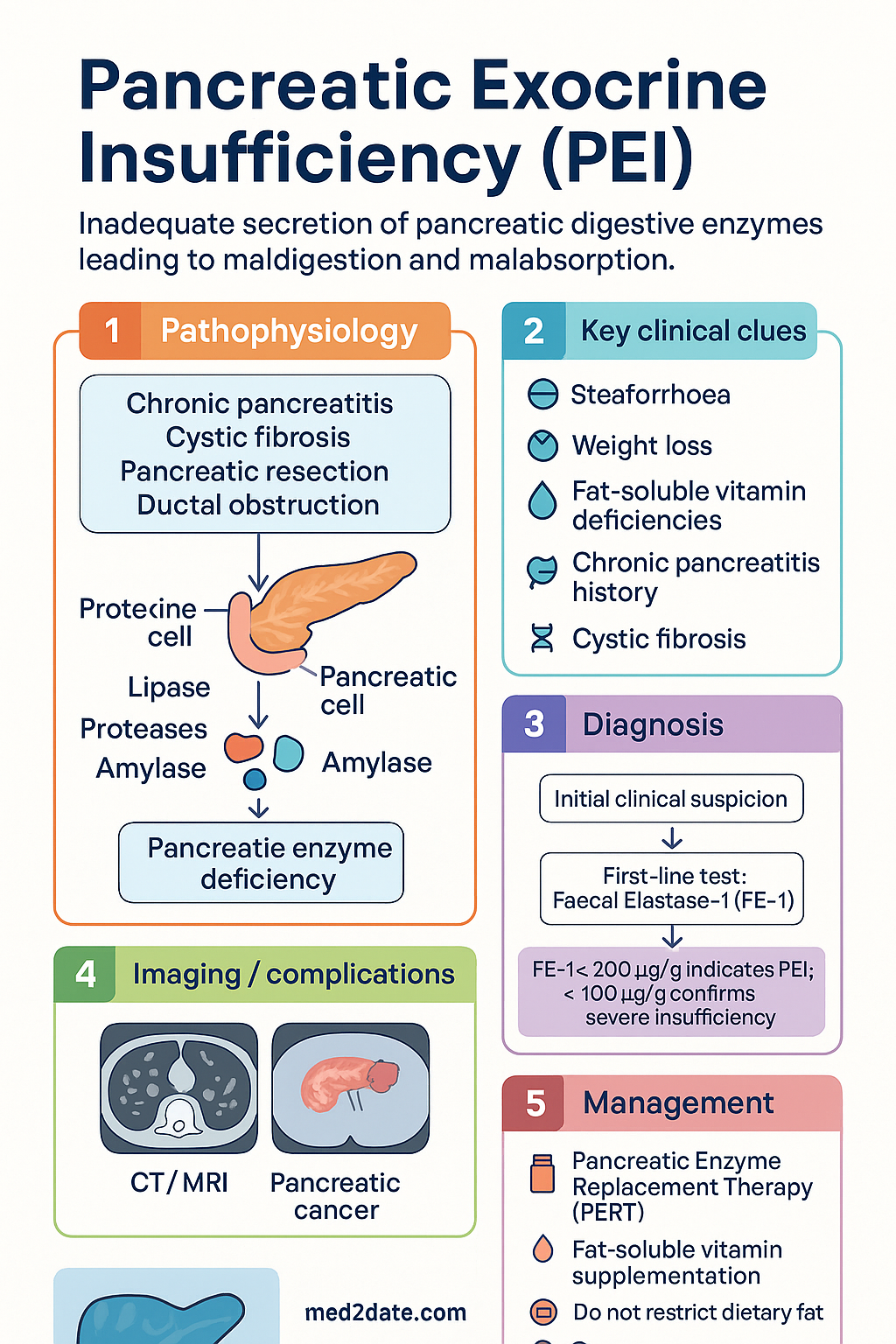
- Definition: Pancreatic exocrine insufficiency (PEI) is the inadequate secretion of pancreatic digestive enzymes, leading to maldigestion, malabsorption, and steatorrhoea.
- Key Causes: Chronic pancreatitis (alcohol-induced most common), cystic fibrosis, pancreatic resection, and pancreatic ductal obstruction from malignancy.
- Diagnostic Gold Standard: Faecal elastase-1 (FE-1) <200 µg/g is indicative; <100 µg/g confirms severe insufficiency.
- Primary Treatment: Pancreatic Enzyme Replacement Therapy (PERT) is cornerstone; initial dose 50,000 units lipase with main meals, 25,000 with snacks.
- Critical Co-therapy: Mandatory fat-soluble vitamin (A, D, E, K) supplementation due to malabsorption; monitor levels and bone density.
- Dietary Principle: Do not restrict dietary fat; ensure adequate energy and protein intake with dietitian support.
- Treatment Goal: Titrate PERT to abolish steatorrhoea, normalise stools, and achieve weight stability.
- Pertinent Investigations: Cross-sectional imaging (CT/MRI) is essential to identify underlying structural pathology (e.g., chronic pancreatitis, cancer).
- Special Populations: High prevalence in cystic fibrosis; dose adjustments may be required in patients post-gastrectomy.
- ATSI Consideration: Increased prevalence linked to alcohol-related chronic pancreatitis; ensure accessible healthcare and dietitian services in remote communities.
Introduction & Australian Epidemiology
Pancreatic exocrine insufficiency (PEI) results from the insufficient synthesis, secretion, or delivery of pancreatic digestive enzymes (lipase, proteases, amylase) into the duodenum. This leads to the maldigestion of macronutrients, particularly fat, causing steatorrhoea, weight loss, and fat-soluble vitamin deficiencies.
In Australia, the most common aetiology is chronic pancreatitis, often secondary to alcohol misuse. The condition is also highly prevalent in cystic fibrosis (CF), affecting over 90% of individuals with CF by adulthood. With rising rates of pancreatic cancer and improved survival in CF, the prevalence of PEI in Australian clinical practice is significant. Early diagnosis and management are crucial to prevent malnutrition-related complications, including osteoporosis.
Aetiology
PEI arises from diverse pathological processes that reduce functional pancreatic parenchyma or obstruct ductal outflow. Identifying the underlying cause guides management and prognosis.
Key Aetiologies
| Aetiology | Pathophysiological Mechanism | Australian Context |
|---|---|---|
| Chronic Pancreatitis | Progressive inflammatory and fibrotic destruction of the exocrine gland. Alcohol is the primary cause (~70%). Other causes include autoimmune pancreatitis, hereditary forms (PRSS1, SPINK1, CFTR mutations), and idiopathic. | Leading cause in adults. High burden associated with alcohol consumption patterns. |
| Cystic Fibrosis | Viscid secretions cause ductal obstruction, acinar cell damage, and progressive pancreatic fibrosis from birth. | Universal screening and PERT initiation in infancy is standard in Australian CF care. |
| Post-Pancreatic Resection | Surgical removal of pancreatic tissue (e.g., Whipple's procedure for cancer, distal pancreatectomy) directly reduces enzyme-producing capacity. | Common after surgery for pancreatic neoplasms or severe trauma. |
| Pancreatic Ductal Obstruction | Tumours (e.g., pancreatic adenocarcinoma, ampullary tumours) or strictures obstruct the main pancreatic duct. | A frequent presentation of advanced pancreatic cancer. |
| Coeliac Disease (Secondary) | Functional insufficiency due to reduced cholecystokinin (CCK) secretion from duodenal mucosal atrophy, leading to inadequate pancreatic stimulation. | Usually reversible with strict gluten-free diet. |
Diagnosis
Diagnosis is clinical, supported by laboratory and imaging findings. It requires a high index of suspicion, as symptoms (steatorrhoea, bloating, weight loss) are non-specific.
Diagnostic Investigations
Treatment
Management is multi-faceted, focusing on enzyme replacement, nutritional support, and treating the underlying cause.
1. Pancreatic Enzyme Replacement Therapy (PERT)
PERT is the cornerstone of therapy. It must be taken with food to ensure mixing with the meal.
2. Nutritional Support & Monitoring
- Fat-Soluble Vitamin (ADEK) Supplementation: Mandatory. Dose is individualised based on serum levels.
- Vitamin D: 1000–2000 IU daily (often higher doses required).
- Vitamin A: 5,000–10,000 IU daily.
- Vitamin E: 100–400 IU daily.
- Vitamin K: 5–10 mg weekly, or adjusted based on INR.
- Bone Density: High risk of osteoporosis. Recommend DEXA scan at diagnosis and every 2–3 years.
- Dietary Counselling: Referral to a specialist gastroenterology dietitian is essential. Key principles:
- DO NOT RESTRICT DIETARY FAT. A low-fat diet exacerbates malnutrition and energy deficit.
- Ensure adequate energy and protein intake.
- Small, frequent meals may be better tolerated.
- Acid Suppression: Proton pump inhibitors (e.g., esomeprazole) may be added in patients with concomitant gastrectomy, Zollinger-Ellison syndrome, or inadequate response to high-dose PERT, to protect enzymes from gastric acid.
3. Management of Underlying Cause
Treat the primary condition where possible: alcohol cessation, pancreatic duct stenting for obstruction, immunotherapy for autoimmune pancreatitis, and enzyme initiation in CF.
Special Populations
Aboriginal and Torres Strait Islander peoples experience a higher burden of alcohol-related chronic pancreatitis, a leading cause of PEI. Management must be culturally safe and address systemic barriers.
📚 References
- 1. Australasian Pancreatic Club. Australasian guidelines for the management of pancreatic exocrine insufficiency. Sydney: APC; 2021.
- 2. Royal Australian College of General Practitioners (RACGP). Chronic pancreatitis in general practice. East Melbourne: RACGP; 2022.
- 3. Australian Institute of Health and Welfare (AIHW). Alcohol, tobacco & other drugs in Australia. Canberra: AIHW; 2023.
- 4. Domínguez-Muñoz JE. Pancreatic exocrine insufficiency: diagnosis and treatment. J Gastroenterol Hepatol. 2011;26 Suppl 2:12-16.
- 5. Struyvenberg MR, Martin CR, Freedman SD. Practical guide to exocrine pancreatic insufficiency - Breaking the myths. BMC Med. 2017;15(1):29.
- 6. Australian Cystic Fibrosis Data Registry. Annual Report, 2022. Sydney: Cystic Fibrosis Australia; 2023.
- 7. National Health and Medical Research Council (NHMRC). Australian Guidelines to Reduce Health Risks from Drinking. Canberra: NHMRC; 2020.
- 8. Phillips ME, Hopper AD, Leeds JS, et al. Consensus for the management of pancreatic exocrine insufficiency: UK practical guidelines. Frontline Gastroenterol. 2021;12(6):492-500.
- 9. RhDAustralia (Remote Area Health Corps). Clinical Manual for Remote Area Nurses. Darwin: RHDAustralia; 2022.
- 10. Lim S, Liang E, Kaffes A, et al. The burden of pancreatic exocrine insufficiency in a tertiary hospital. Intern Med J. 2022;52(Suppl 2):15.