📋 Key Information Summary
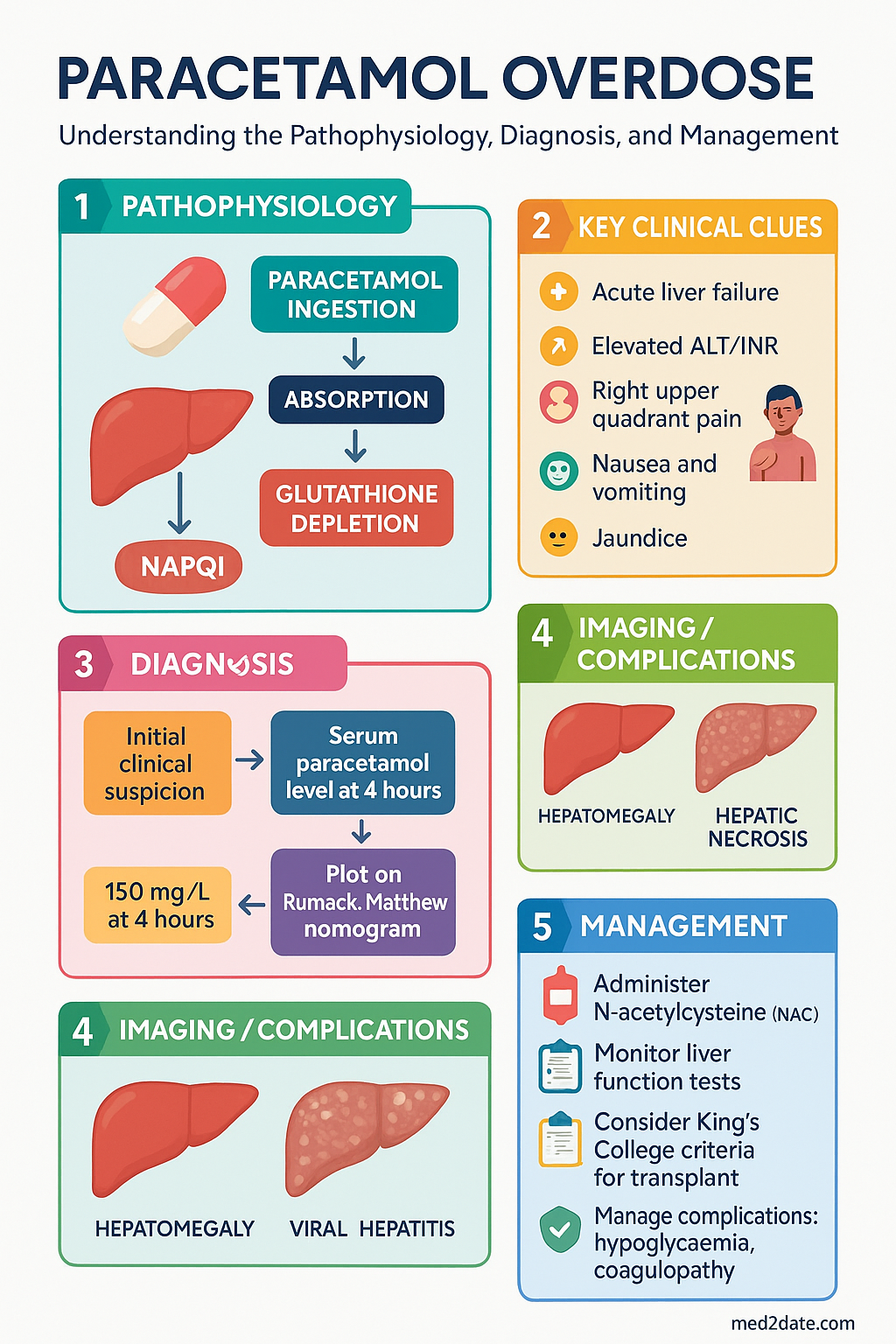
- Paracetamol remains the leading cause of acute liver failure (ALF) in Australia and the most common single agent poisoning presentation to hospital. Early risk stratification using the Rumack–Matthew nomogram guides NAC decisions.
- Single acute ingestion (<8 hours): Plot 4-hour paracetamol level on the Rumack–Matthew nomogram (treatment line: 150 mg/L at 4 h). NAC if level plots above the line.
- Late presentation (8–24 hours): Nomogram still applies but plasma paracetamol level may underestimate toxicity due to ongoing absorption. When in doubt, treat.
- Staggered overdose / unknown timing: Treat with NAC regardless of paracetamol level if ingested dose likely ≥150 mg/kg or ≥10 g (whichever is less), or if ALT/INR elevated.
- Modified-release paracetamol: Paracetamol level at 4 hours may be deceptively low. Re-measure at 8 hours; treat if either level plots above the treatment line on the modified nomogram.
- High-risk patients (chronic alcohol use, malnutrition/fasting >24 h, enzyme inducers e.g. carbamazepine, phenytoin, rifampicin, St John's wort; regular therapeutic paracetamol use >4 g/day) — treat at 100 mg/L on the nomogram rather than 150 mg/L.
- IV N-acetylcysteine (NAC) 3-bag regimen: 200 mg/kg over 4 h → 50 mg/kg over 8 h → 100 mg/kg over 16 h. Total dose 300 mg/kg over 28 hours. The SNAP 2-bag regimen is used in some Australian centres.
- Continue NAC beyond 21 hours if rising INR, ALT, encephalopathy, or persistent paracetamol level. Do not stop until all parameters are improving.
- Anaphylactoid reactions (urticaria, flushing, bronchospasm, hypotension) — stop infusion, treat symptoms (antihistamines, adrenaline if severe), then restart at half the previous rate.
- King's College criteria for transplant referral in paracetamol ALF: Arterial pH <7.3 after fluid resuscitation, OR all three of INR >6.5 + creatinine >300 µmol/L + grade III–IV encephalopathy. Lactate-modified criteria also used.
- Manage complications: Hypoglycaemia (IV dextrose), coagulopathy (avoid prophylactic FFP — masks INR trend; give vitamin K if INR elevated at 24 h with ongoing NAC), encephalopathy (head-up position, ICP monitoring in specialist centres), renal failure (CVVH if oliguric).
- Aboriginal and Torres Strait Islander patients have higher rates of intentional self-harm via paracetamol and face barriers to timely NAC administration in remote areas — activate retrieval services early.
🎧 Audio Brief
Introduction & Australian Epidemiology
Paracetamol (acetaminophen) is the most widely used analgesic and antipyretic in Australia and is available over the counter in multiple formulations. Despite its relative safety at therapeutic doses (up to 4 g/day in healthy adults), paracetamol overdose is the most common single-agent cause of poisoning presenting to Australian emergency departments and the leading cause of acute liver failure requiring liver transplantation.
According to the Australian Institute of Health and Welfare (AIHW), paracetamol-related hospitalisations have risen steadily over the past decade, with over 9,000 admissions per year nationally. The Poisons Information Centres (13 11 26) receive approximately 25,000 calls annually regarding paracetamol exposure. Intentional self-poisoning accounts for the majority of overdoses, with a female preponderance in the 15–24-year age group.
Australia was an early adopter of population-level interventions including blister-pack limits (16 g per pack without prescription in most states) and pharmacy-only sale of larger packs. Despite these measures, paracetamol remains the single most common agent involved in drug overdose presentations.
Risk Assessment
Accurate risk assessment is the cornerstone of paracetamol overdose management. The approach differs depending on the timing and pattern of ingestion. The following clinical scenarios must be systematically evaluated.
Single Acute Ingestion (<8 Hours)
The Rumack–Matthew nomogram is the validated tool for single acute ingestions. Obtain a serum paracetamol level at 4 hours post-ingestion (or as soon as possible thereafter, provided the level is obtained at least 4 hours after ingestion). Plot the result on the nomogram.
- Treatment line (standard risk): 150 mg/L at 4 hours on the nomogram. If the level plots above this line, commence IV NAC immediately.
- Treatment line (high-risk patients): 100 mg/L at 4 hours. High-risk factors are detailed below.
- Levels obtained before 4 hours cannot be reliably interpreted on the nomogram but should still be tested to confirm ingestion and repeated at 4 hours.
Single Acute Ingestion (8–24 Hours)
The nomogram still applies for ingestions up to 24 hours. However, plasma paracetamol levels may underestimate the degree of toxicity if there has been delayed absorption (e.g. co-ingestion of opioids or anticholinergics, modified-release formulations, or food in the stomach). Clinical judgment is essential.
- If time of ingestion is certain and within 24 hours, plot the level on the nomogram.
- If there is any doubt about the timing or amount, treat with NAC.
- Check ALT, INR, and creatinine in all presentations beyond 8 hours.
Late Presentation (>24 Hours)
The nomogram is no longer useful beyond 24 hours. Commence NAC if any of the following are present:
- Detectable paracetamol level (any concentration).
- Elevated ALT (>50 U/L) or rising ALT on serial measurements.
- Elevated INR (>1.3) or rising INR.
- Clinical features of liver injury (right upper quadrant pain, nausea, vomiting, jaundice, encephalopathy).
- History of significant ingestion (>150 mg/kg or >10 g, whichever is less) with no prior NAC treatment.
Staggered Overdose
A staggered overdose involves repeated supratherapeutic ingestion over a period greater than 8 hours. The nomogram does not apply. Treat with NAC if:
- Total ingested dose ≥150 mg/kg or ≥10 g (whichever is less) over the preceding 24 hours.
- Any evidence of hepatotoxicity (elevated ALT, INR, or clinical symptoms).
- When the exact dose or timing cannot be reliably established.
Unknown Timing
When the time of ingestion cannot be determined, the nomogram cannot be used reliably. Commence NAC if there is:
- Any detectable paracetamol level.
- Abnormal biochemistry (ALT, INR, creatinine). class="guideline-li">A plausible history of ingesting a significant dose (≥150 mg/kg).
Modified-Release Paracetamol Preparations
Modified-release (MR) paracetamol (e.g. Panadol Osteo®) has a prolonged absorption phase. A 4-hour paracetamol level may be deceptively low.
- Obtain levels at both 4 and 8 hours post-ingestion.
- Treat if either level plots above the treatment line on the modified nomogram for MR preparations.
- If the 8-hour level is still above 50 mg/L, treat with NAC regardless of the nomogram position.
High-Risk Factors — Lower the Nomogram Threshold to 100 mg/L
| Risk Factor | Mechanism | Clinical Notes |
|---|---|---|
| Chronic alcohol use (≥2 standard drinks/day) | CYP2E1 induction → increased NAPQI production; glutathione depletion | History may be unreliable; check GGT and MCV |
| Malnutrition / fasting >24 hours | Reduced glutathione stores | Anorexia nervosa, eating disorders, homelessness |
| Enzyme inducers | CYP enzyme induction → increased NAPQI | Carbamazepine, phenytoin, phenobarbital, rifampicin, St John's wort, isoniazid |
| Regular therapeutic paracetamol (≥4 g/day for >3 days) | Glutathione depletion from chronic use | Often overlooked; check recent medication history |
| Pre-existing liver disease | Reduced hepatic reserve and detoxification capacity | Chronic hepatitis B/C, cirrhosis, NAFLD |
| HIV infection | Possible altered metabolism; antiretroviral interactions | Treat at lower threshold |
N-Acetylcysteine (NAC) Therapy
Intravenous N-acetylcysteine (NAC) is the definitive antidote for paracetamol toxicity. It replenishes glutathione stores, enhances sulfation and glucuronidation, and provides direct antioxidant protection against NAPQI-mediated hepatocyte injury. NAC is most effective when started within 8 hours of ingestion but remains beneficial at any stage if liver injury is present or developing.
IV NAC — Standard 3-Bag Regimen
The standard Australian regimen (as per Poisons Information Centres and Therapeutic Guidelines) uses weight-based dosing. Always weigh the patient; use ideal body weight if obese (>30% above ideal).
Total dose: 300 mg/kg over 21 hours (loading phase 1 hour + second infusion 4 hours + third infusion 16 hours). Total NAC volume is approximately 1700 mL for an adult.
SNAP 2-Bag Regimen (Alternative)
Some Australian centres (particularly in Queensland and Western Australia) use the SNAP (Simplified NAC Protocol) 2-bag regimen to reduce infusion errors and infusion-related adverse events. The total NAC dose is identical (300 mg/kg) but delivered over two bags:
- Bag 1: 200 mg/kg NAC in 1000 mL 5% dextrose, infused over 12 hours.
- Bag 2: 100 mg/kg NAC in 1000 mL 5% dextrose, infused over 12 hours.
- Total duration: 24 hours. Total dose: 300 mg/kg.
- The SNAP protocol is supported by the Paracetamol Overdose NAC Evaluation (PONI) trial and adopted by several Australian Poisons Information Centres. Check local protocol.
Continuing NAC Beyond 21 Hours
Do not stop NAC at 21 hours if there is evidence of ongoing hepatic injury or risk. Continue infusion if any of the following are present at 21 hours:
- Rising INR (>1.5 or rising trend).
- Rising ALT (above the peak or not yet trending downward).
- Hepatic encephalopathy (any grade).
- Persistent detectable paracetamol level (>10 mg/L).
- Acidaemia (pH <7.35) or rising lactate.
- Significant renal impairment (creatinine rising >1.5× baseline).
Continue NAC at 100 mg/kg/day (Bag 3 rate) until INR is falling and ALT is improving. There is no maximum duration — NAC has been continued for several days in severe cases.
Oral NAC — Alternative Route
Oral NAC is an alternative in some Australian jurisdictions when IV access is problematic, in patients with known severe IV NAC anaphylactoid reactions, or in remote settings. The oral regimen is less commonly used due to GI side effects (nausea, vomiting) and slower onset of action:
- Loading dose: 140 mg/kg PO.
- Maintenance: 70 mg/kg PO every 4 hours × 17 doses.
- Total: 1330 mg/kg over 72 hours.
- Dilute the IV preparation in juice or soft drink to mask taste.
- If vomiting occurs within 1 hour of a dose, repeat the dose. Antiemetics (ondansetron) may be required.
Anaphylactoid Reactions to IV NAC
Anaphylactoid (non-IgE-mediated) reactions occur in approximately 5–20% of patients receiving IV NAC, most commonly during the rapid loading infusion (Bag 1). They are not true anaphylaxis but can be severe.
| Severity | Features | Management |
|---|---|---|
| Mild | Flushing, urticaria, pruritus | Slow infusion rate by 50%. Give oral antihistamine (chlorphenamine 4–10 mg PO/IV or promethazine 10–25 mg IV). Restart at previous rate once resolved. |
| Moderate | Widespread urticaria, angioedema, nausea, tachycardia | Stop infusion. IV antihistamine (chlorphenamine 10 mg IV). Consider hydrocortisone 100–200 mg IV. Restart NAC at half the previous rate once symptoms settle. |
| Severe (anaphylaxis-like) | Hypotension, bronchospasm, stridor, cardiovascular collapse | Stop infusion. Adrenaline 500 µg IM (repeat every 5 min). IV fluids. High-flow O₂. Once stabilised, restart NAC at very slow rate (e.g. over 2–4 hours for Bag 1). Pre-treat with antihistamine + hydrocortisone before restarting. |
Key principles: An anaphylactoid reaction does not contraindicate further NAC. Paradoxically, patients with severe reactions often have more significant paracetamol toxicity and need NAC urgently. If IV NAC cannot be continued, switch to the oral regimen.
Acute Liver Failure & Transplant Criteria
Paracetamol-induced acute liver failure (ALF) is defined as severe liver injury (INR ≥1.5) with hepatic encephalopathy in the absence of pre-existing chronic liver disease. Approximately 0.5–2% of paracetamol overdoses progress to ALF. Early identification and transplant assessment are critical, as the window for successful transplantation is narrow.
King's College Criteria for Liver Transplant Referral
The King's College Criteria remain the most widely used prognostic tool for paracetamol-related ALF. Meeting criteria triggers urgent referral to a liver transplant centre. Transplant referral should occur before criteria are met if clinical trajectory is concerning.
- INR >6.5
- Creatinine >300 µmol/L
- Grade III or IV hepatic encephalopathy
Lactate-Modified Criteria
Lactate provides an early marker of tissue hypoperfusion and mitochondrial dysfunction in paracetamol ALF. Lactate-modified criteria are used as an adjunct to King's College Criteria:
- After early resuscitation: Lactate >3.5 mmol/L.
- After full resuscitation: Lactate >3.0 mmol/L.
- These values are measured at admission and 12 hours post-resuscitation and have high positive predictive value for death without transplant.
Management of ALF Complications
Hypoglycaemia
Hepatic glycogen depletion and impaired gluconeogenesis lead to hypoglycaemia in ALF. This is especially dangerous in children.
- Monitor blood glucose every 1–2 hours (or continuous CGM in ICU).
- Maintain glucose >4 mmol/L with 10% dextrose infusion (avoid 5% dextrose — insufficient glucose delivery).
- If refractory hypoglycaemia, increase dextrose concentration (20–50%) via central line.
Coagulopathy
Elevated INR in paracetamol ALF reflects reduced hepatic synthesis of clotting factors. Management principles:
- Do NOT give prophylactic fresh frozen plasma (FFP). FFP masks the INR trend, which is a key prognostic indicator and guide for transplant referral.
- Give vitamin K (phytomenadione) 10 mg IV if INR is elevated at 24 hours post-overdose and NAC is ongoing — paracetamol can deplete vitamin K-dependent factors.
- FFP is only indicated for active uncontrolled bleeding or prior to invasive procedures.
- Consider prothrombin complex concentrate (PCC) for life-threatening haemorrhage if FFP is insufficient or volume overload is a concern.
- Monitor fibrinogen; cryoprecipitate if <1.0 g/L with bleeding.
- Platelet transfusion only if <10 × 10⁹/L or <50 × 10⁹/L with active bleeding.
Hepatic Encephalopathy
Hepatic encephalopathy in ALF is due to cerebral oedema and ammonia accumulation. Grading and management:
| Grade | Features | Management |
|---|---|---|
| I–II | Confusion, drowsiness, asterixis | Head-up 20–30°. Avoid sedation. Lactulose 20–30 mL PO/NG TDS titrated to 2–3 soft stools/day. Rifaximin may be considered. |
| III | Marked confusion, somnolence but rousable | Intubation for airway protection. ICP monitoring considered. Avoid hyperthermia, hyponatraemia, hypoxia. Mannitol 0.5–1 g/kg IV bolus if signs of raised ICP. |
| IV | Coma, decerebrate posturing | ICP monitoring (bolt) at specialist centre. Target ICP <20–25 mmHg, CPP >60 mmHg. Consider hyperventilation (temporary), hypertonic saline for Na <140. Transplant is the only definitive therapy. |
Acute Kidney Injury / Renal Failure
Renal failure occurs in approximately 25% of paracetamol ALF cases and worsens the prognosis significantly.
- Monitor urine output (target >0.5 mL/kg/h), creatinine, and electrolytes closely.
- Avoid nephrotoxins (aminoglycosides, NSAIDs, contrast).
- Continuous venovenous haemofiltration (CVVH) is preferred over intermittent haemodialysis in haemodynamically unstable patients with ALF.
- CVVH also assists with ammonia clearance.
- Renal replacement therapy may be needed temporarily; renal function often recovers if the patient survives or receives a transplant.
Transplant Referral Pathway
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Monitoring
Serial laboratory monitoring is essential to detect evolving hepatotoxicity and guide decisions about continuing NAC or referring for transplant.
| Test | Timing | Action Thresholds |
|---|---|---|
| Paracetamol level | 4 h, 8 h (MR), repeat if persistent | Nomogram above treatment line → NAC; any detectable level at >24 h → NAC |
| ALT | Baseline, 12 h, 21 h (end of NAC), then daily | >1000 = significant; rising trend = continue NAC; peak then falling = good |
| INR | Baseline, 12 h, 21 h, then 6–12 hourly if elevated | >1.3 = abnormal; >6.5 with encephalopathy + Cr >300 = King's College Criteria B |
| Creatinine | Baseline, 12 h, 21 h, then daily | >300 µmol/L = part of King's College Criteria B; rising = continue NAC, consider CVVH |
| pH (arterial) | Baseline if late presentation; repeat if deteriorating | <7.3 after resuscitation = King's College Criteria A |
| Lactate | Baseline, 12 h post-resuscitation | >3.5 (early) or >3.0 (post-resuscitation) = lactate-modified criteria |
| Glucose | Every 1–2 h in ALF; 4–6 hourly in non-ALF | <4 mmol/L → IV 10% dextrose |
📚 References
- 1. Daly FFS, Fountain JS, Murray L, Graudins A, Buckley NA. Guidelines for the management of paracetamol poisoning in Australia and New Zealand — explanation and elaboration. Med J Aust. 2008;188(5):296–301.
- 2. Chiew AL, Isbister GK, Kirby A, Chan BSH, Buckley NA, Page CB. Massive paracetamol overdose: an observational study of the effect of activated charcoal and N-acetylcysteine. Clin Toxicol. 2020;58(10):1004–1011.
- 3. Bateman DN, Carroll R, Pettie J, et al. Effect of the UK's revised paracetamol poisoning management outcomes: 2-year prospective observational study of 135 admissions. Lancet. 2014;383(9930):1742–1747.
- 4. O'Grady JG, Alexander GJM, Hayllar KM, Williams R. Early indicators of prognosis in fulminant hepatic failure. Gastroenterology. 1989;97(2):439–445.
- 5. Schmidt LE, Dalhoff K. Serum phosphate is an early predictor of outcome in severe acetaminophen-induced hepatotoxicity. Hepatology. 2002;36(3):659–665.
- 6. Bernal W, Donaldson N, Wyncoll D, Wendon J. Blood lactate as an early predictor of outcome in paracetamol-induced acute liver failure: a cohort study. Lancet. 2002;359(9306):558–563.
- 7. Wong A, Graudins A. Simplification of the standard three-bag intravenous acetylcysteine regimen for paracetamol poisoning results in a lower incidence of adverse drug reactions. Clin Toxicol. 2016;54(2):115–119.
- 8. Isbister GK, Downes MA, McNamara K, Berling I, Mostafa A, Buckley NA. Intravenous paracetamol overdose: two case reports and a review of the literature. Emerg Med Australas. 2017;29(1):100–103.
- 9. Rumack BH, Matthew H. Acetaminophen poisoning and toxicity. Pediatrics. 1975;55(6):871–876.
- 10. Australian Institute of Health and Welfare (AIHW). Intentional self-harm hospitalisations in Australia 2021–22. Cat. no. INJCAT 234. Canberra: AIHW; 2023.
- 11. Poisons Information Centre (New South Wales). Paracetamol overdose management guidelines. Sydney: NSW Poisons Information Centre; 2024.
- 12. Craig DGN, Lee A, Hayes PC, Simpson KJ. Review article: the current management of acute liver failure. Aliment Pharmacol Ther. 2010;31(3):345–358.
- 13. Stravitz RT, Lee WM. Acute liver failure. Lancet. 2019;394(10201):869–881.
- 14. Royal Australasian College of Physicians (RACP). Position statement: opioid and paracetamol poisoning in Australia. Sydney: RACP; 2021.