📋 Key Information Summary
- Irritable bowel syndrome (IBS) is a chronic functional gastrointestinal disorder characterised by recurrent abdominal pain associated with altered bowel habits, affecting approximately 10–15% of Australians.
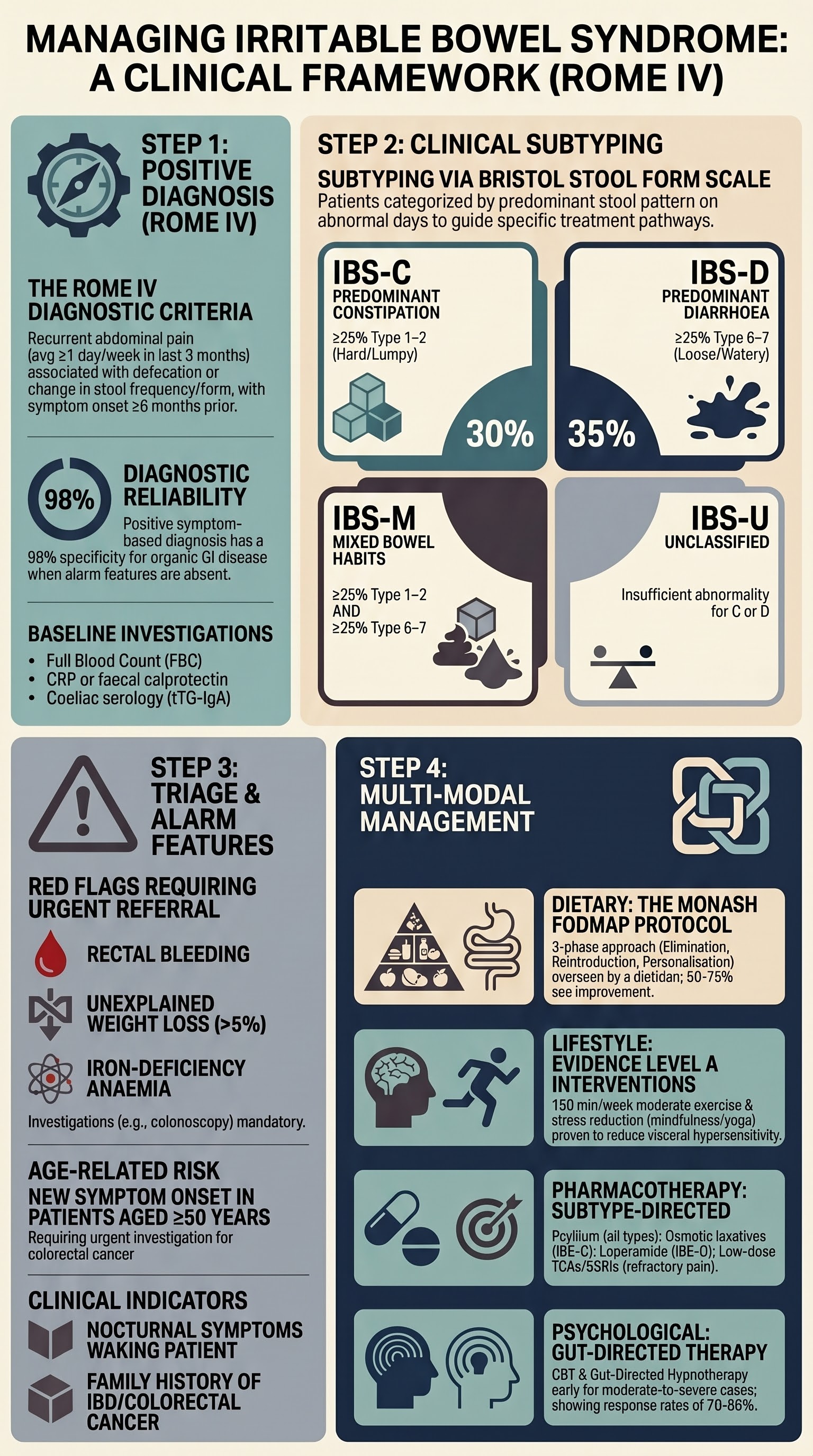
- Diagnosis is clinical using the Rome IV criteria: recurrent abdominal pain ≥1 day/week in the last 3 months, related to defecation, associated with change in stool frequency or form; symptom onset ≥6 months before diagnosis.
- Subtype using the Bristol Stool Form Scale: IBS-C (≥25% Bristol 1–2), IBS-D (≥25% Bristol 6–7), IBS-M (both), IBS-U (unclassified).
- A limited diagnostic workup is recommended in the absence of alarm features: FBC, CRP or faecal calprotectin, coeliac serology (especially in IBS-D/IBS-M), and TSH where indicated.
- Alarm features requiring urgent investigation include rectal bleeding, unintentional weight loss, iron-deficiency anaemia, nocturnal symptoms, family history of colorectal cancer or IBD, and onset after age 50.
- First-line dietary management includes a monash FODMAP-guided elimination diet (2–6 weeks) followed by structured reintroduction under dietitian supervision; soluble fibre (psyllium) is recommended over insoluble fibre.
- Lifestyle interventions — regular moderate exercise, stress reduction, adequate sleep — have Level A evidence for symptom improvement in IBS.
- Pharmacotherapy is subtype-directed: antispasmodics (hyoscine, mebeverine, peppermint oil) for pain; laxatives (osmotic preferred) for IBS-C; loperamide for IBS-D; low-dose TCAs or SSRIs for refractory symptoms.
- Rifaximin (PBS Authority Required) is an option for IBS-D failing conventional therapy; eluxadoline and linaclotide are available but may have restricted PBS access.
- Gut-directed psychological therapies (CBT, gut-directed hypnotherapy) are effective for moderate–severe IBS and should be offered early, not as a last resort.
- Referral to gastroenterology is indicated for alarm features, diagnostic uncertainty, IBS-M with predominant bloody diarrhoea, or failure to respond to 6–12 months of optimised management.
- Aboriginal and Torres Strait Islander Australians have higher rates of functional GI symptoms and face barriers to specialist and dietitian access; culturally safe, community-based approaches are essential.
Introduction & Australian Epidemiology
Irritable bowel syndrome (IBS) is the most common functional gastrointestinal disorder (FGID) worldwide, defined by the Rome IV criteria as a disorder of gut–brain interaction. It is characterised by recurrent abdominal pain associated with defecation or a change in bowel habits, in the absence of structural or biochemical abnormalities that would explain the symptoms.
In Australia, population-based surveys estimate a prevalence of 10–15% using Rome IV criteria, with approximately 30% of those affected seeking medical care. IBS accounts for a substantial proportion of gastroenterology outpatient referrals and primary care consultations. The condition is more prevalent in women (female-to-male ratio approximately 2:1), with peak onset between ages 20 and 40 years.
The economic burden is significant: direct healthcare costs (GP visits, investigations, medications) combined with indirect costs (absenteeism, reduced productivity) are estimated at over AUD 1 billion annually. Patients with IBS report quality-of-life impairment comparable to diabetes mellitus and chronic kidney disease.
IBS significantly impacts on primary care utilisation. The Royal Australian College of General Practitioners (RACGP) recommends a positive diagnostic strategy — making a symptom-based diagnosis and initiating management — rather than pursuing exhaustive exclusionary investigations, provided alarm features are absent.
Rome IV Criteria & Subtyping
The Rome IV criteria (2016) represent the international consensus for diagnosing IBS. A positive diagnosis based on symptom criteria has a sensitivity of approximately 65% and specificity of 98% for organic GI disease when alarm features are absent.
Rome IV Diagnostic Criteria for IBS
Recurrent abdominal pain, on average, ≥1 day per week in the last 3 months, associated with two or more of the following:
- Related to defecation (may be improved or worsened by defecation)
- Associated with a change in stool frequency
- Associated with a change in stool form (appearance)
Criteria fulfilled for the last 3 months with symptom onset ≥6 months before diagnosis.
IBS Subtypes by Bristol Stool Form Scale
Subtyping is based on the predominant stool pattern on days with abnormal bowel movements, using the Bristol Stool Form Scale (BSFS). Patients should be subtyped at each clinical encounter as the pattern may change over time.
| Subtype | Abbreviation | Bristol Type | Proportion of Days | Prevalence |
|---|---|---|---|---|
| IBS with predominant constipation | IBS-C | Type 1–2 (hard/lumpy) | ≥25% of bowel movements | ~30% |
| IBS with predominant diarrhoea | IBS-D | Type 6–7 (loose/watery) | ≥25% of bowel movements | ~35% |
| IBS with mixed bowel habits | IBS-M | Type 1–2 on ≥25% and Type 6–7 on ≥25% | Both criteria met | ~25% |
| IBS unclassified | IBS-U | Insufficient abnormality of stool consistency | Neither C nor D criteria met | ~10% |
Distinguishing IBS from Other FGIDs
Functional dyspepsia, functional constipation, and functional diarrhoea overlap considerably with IBS. The Rome IV framework acknowledges that up to 40% of patients with IBS meet criteria for at least one other FGID. Key distinctions:
- Functional constipation: Difficult, infrequent stools without significant abdominal pain — pain is the defining feature that separates IBS-C from functional constipation.
- Functional diarrhoea: Loose stools without pain — distinguishing feature from IBS-D.
- Microscopic colitis: Must be considered in older women with IBS-D-like symptoms; requires colonic biopsies to exclude.
Limited Diagnostic Workup
A positive diagnostic approach — diagnosing IBS based on symptom criteria and a limited set of investigations — is recommended over an exhaustive exclusionary workup. Studies demonstrate that extensive investigation rarely identifies organic disease in patients meeting Rome IV criteria without alarm features, and repeated negative testing increases health anxiety.
Alarm Features Requiring Further Investigation
- Rectal bleeding or melaena not explained by haemorrhoids
- Unintentional weight loss >5% over 6 months
- Iron-deficiency anaemia (ferritin <30 µg/L, low MCV)
- Nocturnal symptoms that wake the patient from sleep
- Family history of colorectal cancer, coeliac disease, or inflammatory bowel disease
- New onset of symptoms in a patient aged ≥50 years
- Progressive worsening of symptoms over weeks to months
- Palpable abdominal mass or lymphadenopathy
Recommended Baseline Investigations
Optional / Specialist-Level Investigations
- Hydrogen breath testing: For suspected small intestinal bacterial overgrowth (SIBO) or lactose/fructose malabsorption. Available at select centres; MBS items vary by state. Not routinely recommended for IBS diagnosis.
- Colonoscopy: Indicated only with alarm features or age ≥50 with new-onset symptoms (bowel cancer screening age). Bulk-billed via National Bowel Cancer Screening Program if age 50–74.
- Upper GI endoscopy: Consider if prominent upper abdominal symptoms, suspected coeliac disease (with positive serology), or refractory dyspepsia.
- SeHCAT scan: For suspected bile acid malabsorption (BAM) in IBS-D — available at limited tertiary centres in Australia (MBS Item 61339). BAM accounts for up to 25% of IBS-D cases.
Positive Diagnosis Approach — Summary
Dietary & Lifestyle Management
Dietary and lifestyle interventions form the foundation of IBS management. Up to 70% of patients report that food triggers their symptoms. A structured, dietitian-guided approach is recommended over self-directed restriction, which risks nutritional deficiency and disordered eating.
Low FODMAP Diet
The low FODMAP (Fermentable Oligosaccharides, Disaccharides, Monosaccharides, And Polyols) diet was developed at Monash University and is the most evidence-based dietary intervention for IBS. It has Level A evidence from multiple randomised controlled trials.
Three-Phase FODMAP Protocol
- Elimination phase (2–6 weeks): Restrict all high-FODMAP foods. Assess response — approximately 50–75% of patients experience meaningful symptom improvement. If no improvement after 6 weeks, FODMAP is unlikely to be the primary driver; proceed to other interventions.
- Reintroduction phase (6–8 weeks): Systematically reintroduce each FODMAP subgroup one at a time, in increasing doses, over 3 days. Identify individual triggers and tolerance thresholds.
- Personalisation phase (ongoing): Liberalise the diet to include all tolerated foods. Goal is the least restrictive diet that maintains symptom control. Long-term strict low FODMAP is not recommended due to risks of reduced microbiome diversity and nutritional inadequacy.
Fibre Supplementation
- Soluble fibre (psyllium/ispaghula husk): Recommended as first-line for all IBS subtypes. Start at 3–5 g daily, titrate up to 10–12 g over several weeks. Evidence supports improvement in global IBS symptoms and stool consistency. Available OTC (Metamucil®, Fybogel®).
- Insoluble fibre (wheat bran): Not recommended in IBS — may worsen bloating, flatulence, and abdominal pain. Avoid or use with caution.
- Partially hydrolysed guar gum (PHGG): Emerging evidence supports use in IBS-C and IBS-M. 5 g daily. Available as Sunfiber® in Australia.
Lifestyle Interventions
Other Dietary Considerations
- Gluten-free diet: May benefit a subset of patients (non-coeliac gluten/wheat sensitivity) even with negative coeliac serology. Trial of 4–6 weeks after excluding coeliac disease; evidence is moderate.
- Caffeine and alcohol: Advise moderation. Both exacerbate visceral motility and sensitivity. Limit caffeine to ≤2 cups/day.
- Probiotics: Evidence is strain-specific. Bifidobacterium infantis 35624 and Lactobacillus plantarum 299v have the strongest evidence. Trials of individual strains for 4–8 weeks are reasonable. Multi-strain preparations of uncertain benefit. Not PBS-listed.
Pharmacologic Management
Pharmacotherapy in IBS is adjunctive to dietary and lifestyle interventions and should be tailored to the predominant symptom and subtype. Medications should be trialled for a minimum of 4–8 weeks at adequate dose before declaring failure. Polypharmacy should be avoided.
Symptom-Based: Abdominal Pain & Cramping
Subtype-Specific: IBS-C (Constipation Predominant)
Subtype-Specific: IBS-D (Diarrhoea Predominant)
Gut-Directed Antidepressants
Low-dose neuromodulators are effective in IBS at doses lower than those used for depression. They modulate visceral pain perception, central pain processing, and gut motility. Allow 6–8 weeks for full effect.
Bile Acid Sequestrants (IBS-D with Suspected BAM)
Subtype-Specific: IBS-M (Mixed Bowel Habits)
IBS-M is the most challenging subtype to treat pharmacologically as patients alternate between constipation and diarrhoea. Management principles include:
- Target the currently predominant symptom at each visit
- Antispasmodics and gut-directed antidepressants (especially TCAs) are preferred as they address pain without exacerbating bowel habit abnormalities
- Avoid antidiarrhoeals (may worsen constipation phases) and stimulant laxatives (may worsen diarrhoea phases)
- Soluble fibre (psyllium) is particularly useful as it normalises stool form in both directions
- Low-dose TCAs are often the single most useful medication in IBS-M
Quick Reference: Medication by Subtype
Psychological Therapies & Referral
The gut–brain axis is central to IBS pathophysiology. Psychological comorbidity (anxiety, depression, somatisation) is present in up to 60% of patients with IBS seen in specialist practice. Psychological therapies have Level A evidence and should be presented as a treatment modality, not a stigmatising suggestion that symptoms are "psychological."
Evidence-Based Psychological Therapies
When to Refer
- Alarm features (rectal bleeding, weight loss, iron-deficiency anaemia, nocturnal symptoms, age ≥50 with new symptoms, family history of CRC/IBD)
- Diagnostic uncertainty — atypical symptoms, incomplete Rome IV criteria, positive faecal calprotectin or CRP
- Failure to respond to 6–12 months of optimised first- and second-line management
- IBS-M with predominant bloody diarrhoea (exclude microscopic colitis, bile acid malabsorption)
- Severe symptoms with significant functional impairment (unable to work, social isolation)
- Patient request for specialist opinion
Access to Psychological Therapies for IBS in Australia
| Therapy | Availability | How to Access | Cost |
|---|---|---|---|
| Gut-directed CBT (face-to-face) | Metropolitan centres; some regional via telehealth | MHTP + psychologist referral; Ask for GI-experienced psychologist | Gap varies (~AUD 50–150/session) |
| Gut-directed hypnotherapy | Limited — select tertiary hospitals and private practitioners | Gastroenterologist or GP referral | Variable; some hospital-based = no cost |
| Digital hypnotherapy (Nerva app) | Australia-wide (online) | Self-enrol or GP-prescribed | ~AUD 120 for 6-week programme |
| Monash Mindgut (CBT via telehealth) | Australia-wide | Research program; check availability | May be free during research phases |
The Therapeutic Relationship
A strong GP–patient relationship is the most important factor in IBS management. Validating the patient's symptoms, explaining the pathophysiology (disordered gut–brain signalling, not "all in your head"), and setting realistic expectations (symptom management rather than cure) improve adherence and outcomes. The RACGP recommends regular follow-up (every 4–8 weeks during active management) to reinforce positive strategies and adjust treatment.
Special Populations
Pregnancy & Breastfeeding
Paediatrics
- Paediatric IBS affects 5–10% of children and is diagnosed using modified Rome IV criteria. Functional abdominal pain — not otherwise specified (FAP-NOS) should be distinguished.
- First-line: dietary modification (fibre, identify triggers), parental reassurance, normal school attendance. Low FODMAP in children should only be undertaken with paediatric dietitian supervision.
- Pharmacotherapy evidence is limited in children. Peppermint oil (enteric-coated, ≥8 years) and psyllium have the best evidence. Avoid TCAs in children without specialist guidance.
- Psychological interventions (CBT, guided imagery, gut-directed hypnotherapy) have strong evidence in paediatric functional GI disorders. Refer to paediatric psychologist.
- Referral to paediatric gastroenterology if alarm features, diagnostic uncertainty, or failure to respond to 3–6 months of management.
Elderly (≥65 years)
- New-onset IBS symptoms in patients aged ≥50 years mandate investigation (colonoscopy) to exclude colorectal cancer, diverticular disease, and microscopic colitis before accepting an IBS diagnosis.
- IBS is less common in elderly patients; consider medication-related GI symptoms (metformin, NSAIDs, PPIs, SSRIs, antibiotics).
- Anticholinergic medications (hyoscine) should be used cautiously due to risk of confusion, urinary retention, falls, and constipation. Mebeverine is preferred.
- Loperamide use with caution — risk of megacolon if there is subclinical obstruction.
- Low-dose TCAs: increased risk of cardiac conduction abnormalities, falls, and cognitive impairment. ECG before starting. Consider SSRI as alternative.
Renal Impairment
- Macrogol 3350: use with caution in CKD — monitor electrolytes (hyponatraemia, hypokalaemia). Avoid in patients on fluid restriction.
- Amitriptyline: no specific dose adjustment, but enhanced sensitivity in uraemia. Start low, go slow.
- Linaclotide: no dose adjustment required.
- Loperamide: no specific adjustment; minimal renal excretion.
Hepatic Impairment
- Rifaximin: avoid in Child-Pugh C (severe) hepatic impairment.
- Eluxadoline: contraindicated in severe hepatic impairment. ALT monitoring recommended.
- Escitalopram: maximum 10 mg/day in hepatic impairment.
- Amitriptyline: reduce dose; use caution.
- Loperamide: use with caution — reduced first-pass metabolism.
📚 References
- 1. Lacy BE, Mearin F, Chang L, et al. Bowel disorders. Gastroenterology. 2016;150(6):1393–1407.e5. doi:10.1053/j.gastro.2016.02.031 (Rome IV criteria)
- 2. Ford AC, Sperber AD, Corsetti M, Camilleri M. Irritable bowel syndrome. Lancet. 2020;396(10263):1675–1688. doi:10.1016/S0140-6736(20)31548-8
- 3. Whorwell PJ, Altringer L, Morel J, et al. Efficacy of an encapsulated probiotic Bifidobacterium infantis 35624 in women with irritable bowel syndrome. World J Gastroenterol. 2009;15(12):1453–1458.
- 4. Halmos EP, Power VA, Shepherd SJ, Gibson PR, Muir JG. A diet low in FODMAPs reduces symptoms of irritable bowel syndrome. Gastroenterology. 2014;146(1):67–75.e5. doi:10.1053/j.gastro.2013.09.046
- 5. Johannesson E, Simrén M, Strid H, Bajor A, Sadik R. Physical activity improves symptoms in irritable bowel syndrome: a randomized controlled trial. Am J Gastroenterol. 2011;106(5):915–922. doi:10.1038/ajg.2010.480
- 6. Ford AC, Harris LA, Lacy BE, Quigley EMM, Moayyedi P. Systematic review with meta-analysis: the efficacy of prebiotics, probiotics, synbiotics and antibiotics in irritable bowel syndrome. Aliment Pharmacol Ther. 2018;48(10):1044–1060. doi:10.1111/apt.15001
- 7. Black CJ, Ford AC. Global burden of irritable bowel syndrome: trends, predictions and risk factors. Nat Rev Gastroenterol Hepatol. 2020;17(8):473–486. doi:10.1038/s41575-020-0286-8
- 8. Lackner JM, Jaccard J, Keefer L, et al. Improvement in gastrointestinal symptoms after cognitive behavior therapy for refractory irritable bowel syndrome. Gastroenterology. 2018;155(1):47–57. doi:10.1053/j.gastro.2018.03.063
- 9. Peters SL, Yao CK, Philpott H, Yelland GW, Muir JG, Gibson PR. Randomised clinical trial: the efficacy of gut-directed hypnotherapy is similar to that of the low FODMAP diet for the treatment of irritable bowel syndrome. Aliment Pharmacol Ther. 2016;44(5):447–459. doi:10.1111/apt.13706
- 10. Royal Australian College of General Practitioners (RACGP). Guidelines for preventive activities in general practice. 9th ed. Melbourne: RACGP; 2018.
- 11. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework: Summary report. Canberra: AIHW; 2023.
- 12. Menees SB, Maneerattannaporn M, Kim HM, Chey WD. The efficacy and safety of rifaximin for the irritable bowel syndrome: a systematic review and meta-analysis. Am J Gastroenterol. 2012;107(1):28–35. doi:10.1038/ajg.2011.355
- 13. Wald A, Rakel D. Behavioral and complementary approaches for the treatment of irritable bowel syndrome. Nutr Clin Pract. 2008;23(3):284–292.
- 14. National Health and Medical Research Council (NHMRC). Evidence-based clinical practice guideline for the management of overweight and obesity in adults, adolescents and children in Australia. Melbourne: NHMRC; 2013.
- 15. Chey WD, Kurlander J, Eswaran S. Irritable bowel syndrome: a clinical review. JAMA. 2015;313(9):949–958. doi:10.1001/jama.2015.0954