📋 Key Information Summary
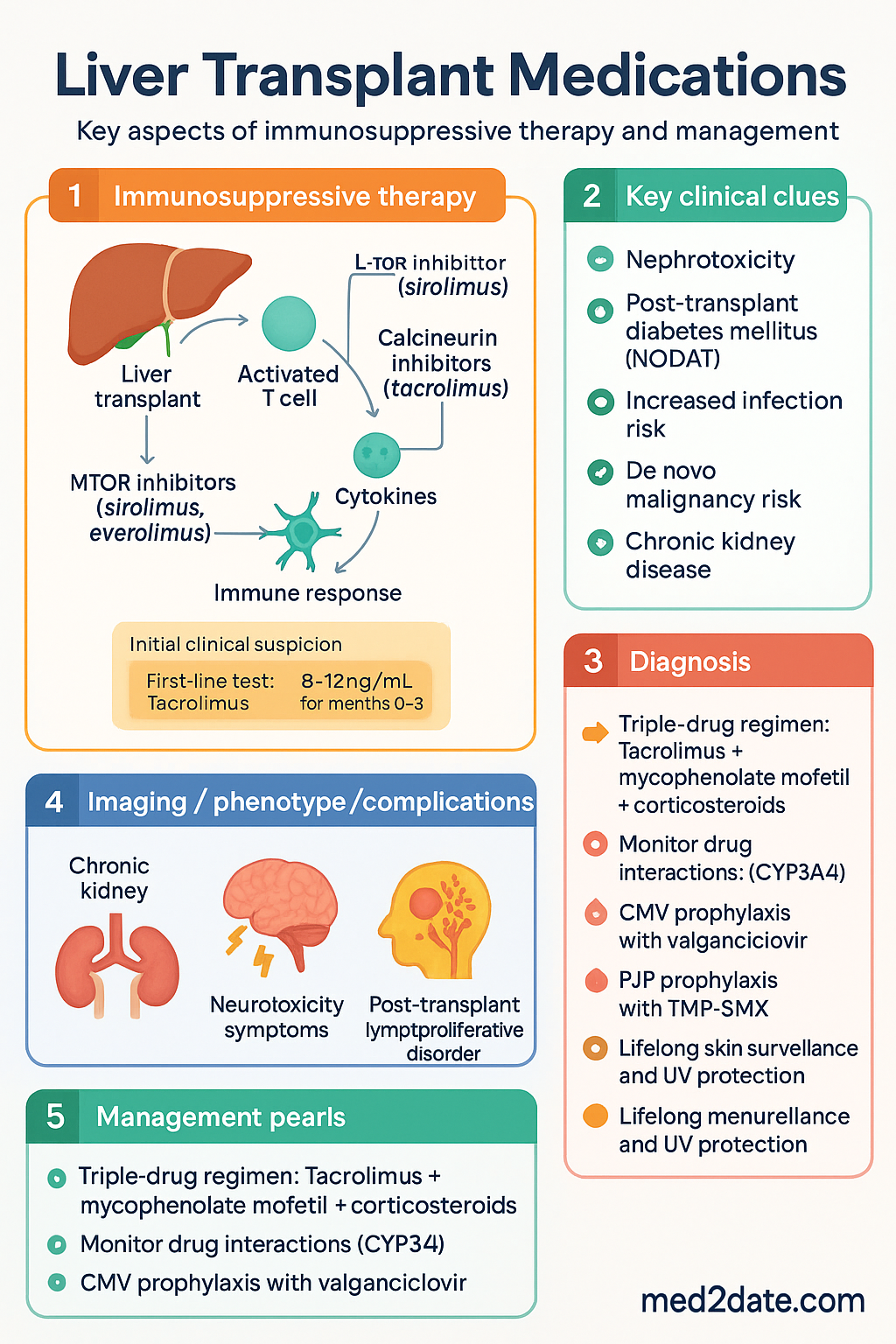
- Liver transplant immunosuppression in Australia follows a triple-drug paradigm: a calcineurin inhibitor (CNI) — almost exclusively tacrolimus — plus an antimetabolite (mycophenolate mofetil) plus short-course corticosteroids.
- Induction therapy with basiliximab (IL-2 receptor antagonist) is standard for most adult liver transplant recipients; antithymocyte globulin (ATG) reserved for high immunological risk or delayed renal recovery.
- Tacrolimus target trough levels vary by time post-transplant: 8–12 ng/mL (months 0–3), 5–8 ng/mL (months 3–12), 4–6 ng/mL (>12 months) — individualised by rejection risk and renal function.
- CYP3A4 interactions are critical: azoles (fluconazole, itraconazole), macrolides (erythromycin, clarithromycin), diltiazem, and grapefruit juice raise tacrolimus levels; rifampicin, phenytoin, and carbamazepine dramatically lower levels and must trigger pre-emptive dose doubling and frequent monitoring.
- Mycophenolate mofetil (CellCept®) 1 g BD is the preferred antimetabolite; azathioprine used less commonly. mTOR inhibitors (sirolimus, everolimus) are second-line agents useful for CNI nephrotoxicity sparing and HCC recurrence reduction.
- Post-transplant diabetes mellitus (NODAT) affects 10–40% of recipients; tacrolimus is a stronger risk factor than ciclosporin. Metformin is first-line; insulin may be required acutely.
- CMV prophylaxis with valganciclovir is guided by donor/recipient serostatus: D+/R− (highest risk) receives 6 months; other at-risk combinations receive 3–6 months.
- PJP prophylaxis with trimethoprim-sulfamethoxazole (TMP-SMX) is given for 6–12 months post-transplant; dapsone or atovaquone are alternatives for sulphonamide allergy.
- Chronic kidney disease develops in up to 20% of recipients by 10 years — primarily CNI-mediated. Strategies include CNI minimisation, mTOR inhibitor conversion, and early nephrology referral.
- De novo malignancy risk is 2–3× general population; post-transplant lymphoproliferative disorder (PTLD) is associated with EBV serostatus mismatch. Lifelong skin surveillance and UV protection are essential.
- Vaccinations must be completed pre-transplant where possible (including pneumococcal, influenza, hepatitis B). Live vaccines are contraindicated post-transplant.
- Aboriginal and Torres Strait Islander patients may face barriers including geographic remoteness from transplant centres, variable health literacy, and higher baseline prevalence of chronic liver disease — requiring culturally safe, multidisciplinary follow-up.
🎧 Audio Brief
Induction & Maintenance Immunosuppression
Principles of Immunosuppressive Therapy
Liver transplant immunosuppression in Australia aims to balance rejection prevention against infection risk, malignancy, and drug toxicity. The liver is relatively immunoprivileged compared with other solid organs, allowing lower overall immunosuppressive intensity. Most centres adopt a triple-drug regimen from the outset.
Induction Therapy
Induction agents provide intense immunosuppression during the perioperative period when rejection risk is highest.
Maintenance Immunosuppression
The standard Australian maintenance regimen comprises a calcineurin inhibitor (tacrolimus) + an antimetabolite (mycophenolate mofetil) ± low-dose corticosteroids. Conversion to mTOR inhibitors is considered for CNI toxicity or HCC recurrence risk.
Calcineurin Inhibitors
Antimetabolites
mTOR Inhibitors
mTOR inhibitors (sirolimus, everolimus) are used as CNI-sparing agents or in patients with de novo or recurrent HCC. They impair wound healing and should generally be avoided in the first 4–6 weeks post-transplant.
Corticosteroids
Acute Cellular Rejection Management
| Phase | Tacrolimus target (ng/mL) | Mycophenolate | Prednisolone |
|---|---|---|---|
| 0–3 months | 8–12 | 1 g BD | Taper from 200 mg to 20 mg |
| 3–12 months | 5–8 | 1 g BD (or reduce) | Taper toward 5 mg or cessation |
| >12 months | 4–6 | 500 mg–1 g BD | 5 mg or ceased |
| Autoimmune disease | 6–8 | 1 g BD (maintain) | 5 mg long-term |
Drug Interactions & Monitoring
CYP3A4 Interactions — Critical Safety Issue
Tacrolimus and ciclosporin are extensively metabolised by CYP3A4 and CYP3A5 in the gut wall and liver. P-glycoprotein (P-gp) also modulates absorption. Co-administration with CYP3A4 modulators is one of the most common causes of drug-related toxicity or sub-therapeutic levels in transplant recipients.
CYP3A4 Inhibitors — Raise Tacrolimus/Ciclosporin Levels
| Drug / Substance | Potency | Action Required |
|---|---|---|
| Ketoconazole | Strong | Avoid or reduce CNI by 50–75%; monitor levels 48–72 h after initiation |
| Fluconazole (doses >200 mg/day) | Moderate–Strong | Reduce CNI dose by 25–50%; monitor levels every 3–5 days |
| Itraconazole, posaconazole, voriconazole | Strong | Reduce CNI by 50%; therapeutic drug monitoring essential |
| Erythromycin, clarithromycin | Moderate | Avoid if possible; use azithromycin (minimal CYP3A4 effect) instead |
| Diltiazem, verapamil | Moderate | Reduce CNI by 25–50%; monitor levels |
| Grapefruit / grapefruit juice | Moderate | Strictly avoid — inhibits intestinal CYP3A4 and P-gp |
| Seville oranges, star fruit | Mild–Moderate | Avoid |
CYP3A4 Inducers — Lower Tacrolimus/Ciclosporin Levels
| Drug | Potency | Action Required |
|---|---|---|
| Rifampicin (rifampin) | Strong | Double or triple CNI dose; check trough every 2–3 days; consult transplant team |
| Phenytoin | Strong | Double CNI dose; monitor levels frequently; consider alternative anticonvulsant (levetiracetam) |
| Carbamazepine | Strong | Avoid if possible — switch to levetiracetam or sodium valproate |
| St John's wort (Hypericum perforatum) | Strong | Strictly contraindicated — advise patients to cease all herbal supplements |
| Nafcillin, rifabutin | Moderate | Increase CNI dose; monitor levels every 3–5 days |
Therapeutic Drug Monitoring Schedule
| Time Post-Transplant | Tacrolimus Trough Frequency | Notes |
|---|---|---|
| 0–2 weeks | Daily | Stabilise levels; adjust dose in 0.5–1 mg increments |
| 2 weeks – 3 months | 1–2× per week | Steady state; monitor renal function, glucose |
| 3–12 months | Every 2–4 weeks | Gradual target reduction |
| >12 months (stable) | Every 1–3 months | Check levels after any drug interaction change |
| After interacting drug change | 48–72 h after change, then every 2–3 days until stable | Document interaction in patient record |
Adverse Effect Monitoring
Other monitoring: Blood pressure (CNI-induced hypertension — target <130/80 mmHg, use amlodipine if needed as it does not affect CNI levels; avoid diltiazem/verapamil), lipid profile (mTOR inhibitors worsen hyperlipidaemia), FBC (mycophenolate/azathioprine cytopenias), LFTs (rejection surveillance).
Post-Transplant Diabetes (NODAT) Management
Infectious Prophylaxis & Long-Term Complications
CMV Prophylaxis
Cytomegalovirus (CMV) is the most important viral pathogen post-liver transplant. Prophylaxis is determined by donor (D) and recipient (R) CMV IgG serostatus.
| D/R Serostatus | Risk Category | Prophylaxis | Duration |
|---|---|---|---|
| D+/R− | Highest | Valganciclovir 900 mg PO daily | 6 months (some centres 12 months) |
| D+/R+ | High | Valganciclovir 900 mg PO daily | 3–6 months |
| D−/R+ | Moderate | Valganciclovir 900 mg PO daily (or valaciclovir 2 g TDS) | 3 months |
| D−/R− | Low | No routine prophylaxis; monitor with CMV PCR | — |
PJP (Pneumocystis jirovecii) Prophylaxis
Antifungal Prophylaxis
Invasive fungal infection (IFI) — predominantly Candida and Aspergillus — is a significant early post-transplant complication. Antifungal prophylaxis is recommended for high-risk patients.
- High-risk criteria: Re-transplantation, reoperation, renal replacement therapy, massive transfusion (>40 units), prolonged ICU stay, choledochojejunostomy anastomosis, fulminant hepatic failure.
- First-line: Fluconazole 200–400 mg PO/IV daily for 4–6 weeks (covers Candida). PBS: General Benefit.
- If Aspergillus risk: Posaconazole 300 mg PO daily or voriconazole 200 mg PO BD — consult infectious diseases. Monitor CNI levels closely (strong CYP3A4 inhibition).
- Low-risk patients: No routine antifungal prophylaxis; monitor clinically.
Pre-Transplant Vaccination
All vaccinations should be completed before liver transplant wherever possible. Live vaccines are contraindicated post-transplant and for 4 weeks prior if possible.
| Vaccine | Pre-Transplant | Post-Transplant |
|---|---|---|
| Influenza (inactivated) | Yes | Yes — annually from 1 month post-transplant |
| Pneumococcal (PCV13 then PPSV23) | Yes — complete series | Revaccinate 3–5 years post-transplant |
| Hepatitis B | Yes — high-dose schedule (40 μg × 3) | Booster if anti-HBs <10 mIU/mL |
| Hepatitis A | Yes if non-immune | Safe post-transplant (inactivated) |
| COVID-19 (mRNA) | Yes — complete primary + booster | Yes — may have reduced response; additional doses recommended |
| MMR (live) | Yes if non-immune | Contraindicated — live vaccine |
| Varicella (live) | Yes if non-immune (VZV IgG negative) | Contraindicated — use aciclovir prophylaxis if exposed |
| Zoster (Shingrix — recombinant) | Yes if ≥50 years | Safe post-transplant (non-live); 2 doses, 2–6 months apart |
Long-Term Complications
Chronic Kidney Disease
CKD develops in up to 20% of liver transplant recipients by 10 years, predominantly driven by CNI nephrotoxicity. Pre-existing renal impairment (hepatorenal syndrome), diabetes, and hypertension are contributing factors.
- Strategies: CNI minimisation (target lower troughs); conversion to mTOR inhibitor (everolimus or sirolimus) with low-dose CNI; early nephrology referral if eGFR <30 mL/min.
- Monitor eGFR, urine ACR, and electrolytes at every visit.
- Avoid nephrotoxins (NSAIDs, iodinated contrast without hydration) and maintain adequate hydration.
Cardiovascular Disease
Metabolic syndrome is common post-transplant (incidence 40–60%) driven by corticosteroids, CNI, and mTOR inhibitors. Cardiovascular disease is now a leading cause of late mortality.
- Targets: BP <130/80 mmHg, LDL <2.0 mmol/L, HbA1c <7.0% (individualised).
- Statins (atorvastatin preferred — minimal CYP3A4 interaction with tacrolimus at low doses). PBS: General Benefit.
- Amlodipine for hypertension (does not interact with CNI; avoid diltiazem).
- Encourage physical activity, weight management, smoking cessation, and Mediterranean diet.
De Novo Malignancy
Post-transplant malignancy risk is 2–3× that of the age-matched general population. Non-melanoma skin cancer (NMSC) and post-transplant lymphoproliferative disorder (PTLD) are the most significant.
- NMSC: Most common de novo malignancy. Risk increases with cumulative immunosuppression and UV exposure in Australia. Annual full skin examination by a dermatologist or trained GP; daily SPF 50+ sunscreen; protective clothing.
- PTLD: Associated with EBV D+/R− mismatch and intensity of immunosuppression. Presents most commonly in the first year. Lowering immunosuppression is first-line; rituximab for CD20+ tumours; chemotherapy for refractory disease.
- Solid organ tumours: Increased risk of colorectal, lung, and kidney cancers. Follow national screening programmes (bowel cancer screening from 45 years).
Recurrent Primary Disease
Certain liver diseases recur post-transplant and require specific management:
- Hepatitis C: Direct-acting antivirals (DAAs) post-transplant (sofosbuvir/velpatasvir) achieve >95% SVR. PBS listed.
- Hepatitis B: Hepatitis B immunoglobulin (HBIg) + nucleos(t)ide analogue (entecavir/tenofovir) — indefinite prophylaxis.
- Autoimmune hepatitis: Recurrence in 20–40%. Maintain low-dose prednisolone (5 mg) and adequate immunosuppression.
- Primary sclerosing cholangitis: Recurrence in 10–25%; often diagnosed on cholangiography. Associated with underlying IBD — continue colonoscopy surveillance.
- Primary biliary cholangitis: Recurrence in 10–30%. Ursodeoxycholic acid (UDCA) may be continued post-transplant.
- NASH / metabolic-associated steatohepatitis: Recurrence common if metabolic syndrome persists. Aggressive risk factor management.
Late Rejection
Late acute rejection (>6 months) and chronic rejection are less common but carry significant graft implications. Non-adherence with immunosuppression is the most common cause.
- Maintain adequate trough levels; educate patients about adherence — particularly in adolescents.
- Chronic (ductopenic) rejection: progressive loss of bile ducts; may present with cholestatic biochemistry. Treatment: optimise immunosuppression; if refractory, re-transplantation may be required.
ATSI — Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. European Association for the Study of the Liver (EASL). EASL Clinical Practice Guidelines: Liver transplantation. J Hepatol. 2016;64(2):433–485.
- 2. Charlton M, Levitsky J, Bzowej N, et al. Liver transplantation in patients with nonalcoholic steatohepatitis: a consensus conference report. Am J Transplant. 2022;22(Suppl 1):1–34.
- 3. Kotton CN, Kumar D, Caliendo AM, et al. The Third International Consensus Guidelines on the Management of Cytomegalovirus in Solid-organ Transplantation. Transplantation. 2018;102(6):900–931.
- 4. Transplantation Society of Australia and New Zealand (TSANZ). Organ Transplantation from Deceased Donors: Policies and Guidelines. Sydney: TSANZ; 2023.
- 5. Kidney Disease: Improving Global Outcomes (KDIGO). KDIGO Clinical Practice Guideline for the Care of Kidney Transplant Recipients. Am J Transplant. 2009;9(Suppl 3):S1–S155.
- 6. Australian Technical Advisory Group on Immunisation (ATAGI). Australian Immunisation Handbook. Australian Government Department of Health; 2023. Available at: https://immunisationhandbook.health.gov.au.
- 7. Australasian Society for Infectious Diseases (ASID). Guidelines for the Prevention, Diagnosis and Management of Infections in Solid Organ Transplant Recipients. Sydney: ASID; 2020.
- 8. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework 2020 Summary Report. Canberra: AIHW; 2020.
- 9. Line PD, Rela M, editors. Transplantation of the Liver. 3rd ed. Elsevier; 2015.
- 10. Organ and Tissue Authority (OTA). DonateLife Annual Report 2022–23. Canberra: Australian Government; 2023.
- 11. McKenna GJ, Trotter JF, Klintmalm E, et al. Limiting hepatocellular carcinoma recurrence after liver transplantation: is it time for mTOR inhibitor–based immunosuppression? Transplantation. 2014;97(9):931–936.
- 12. RHDAustralia. The 2020 Australian Guideline for Prevention, Diagnosis and Management of Acute Rheumatic Fever and Rheumatic Heart Disease. 3rd ed. Darwin: Menzies School of Health Research; 2020.
- 13. The Transplantation Society. Banff Schema for Allograft Rejection: 2022 Update. Am J Transplant. 2022;22(8):1873–1886.