📋 Key Information Summary
- Dyspepsia is defined as chronic or recurrent pain or discomfort centred in the upper abdomen, affecting approximately 30–40% of Australian adults annually, and accounting for a significant proportion of GP consultations.
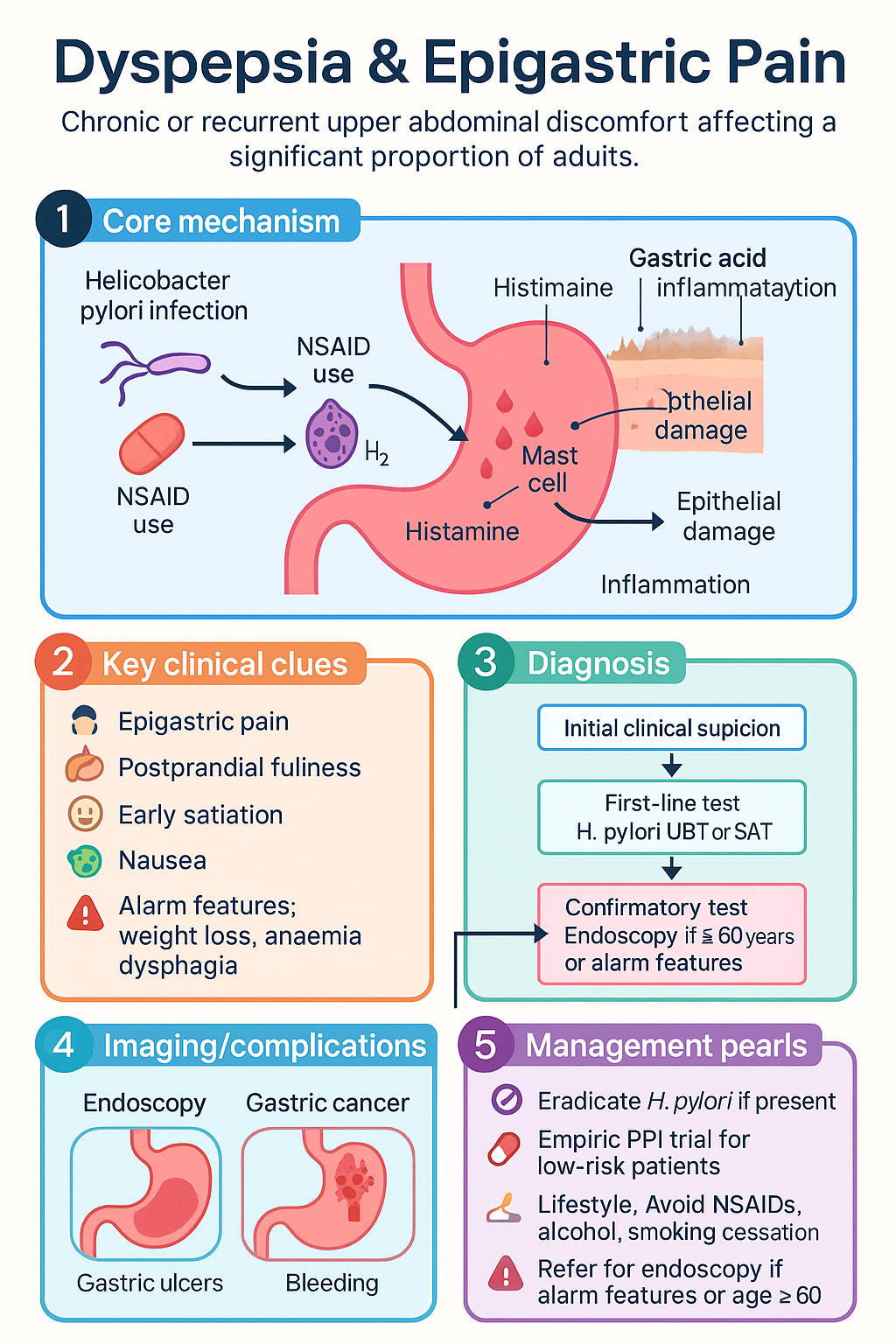
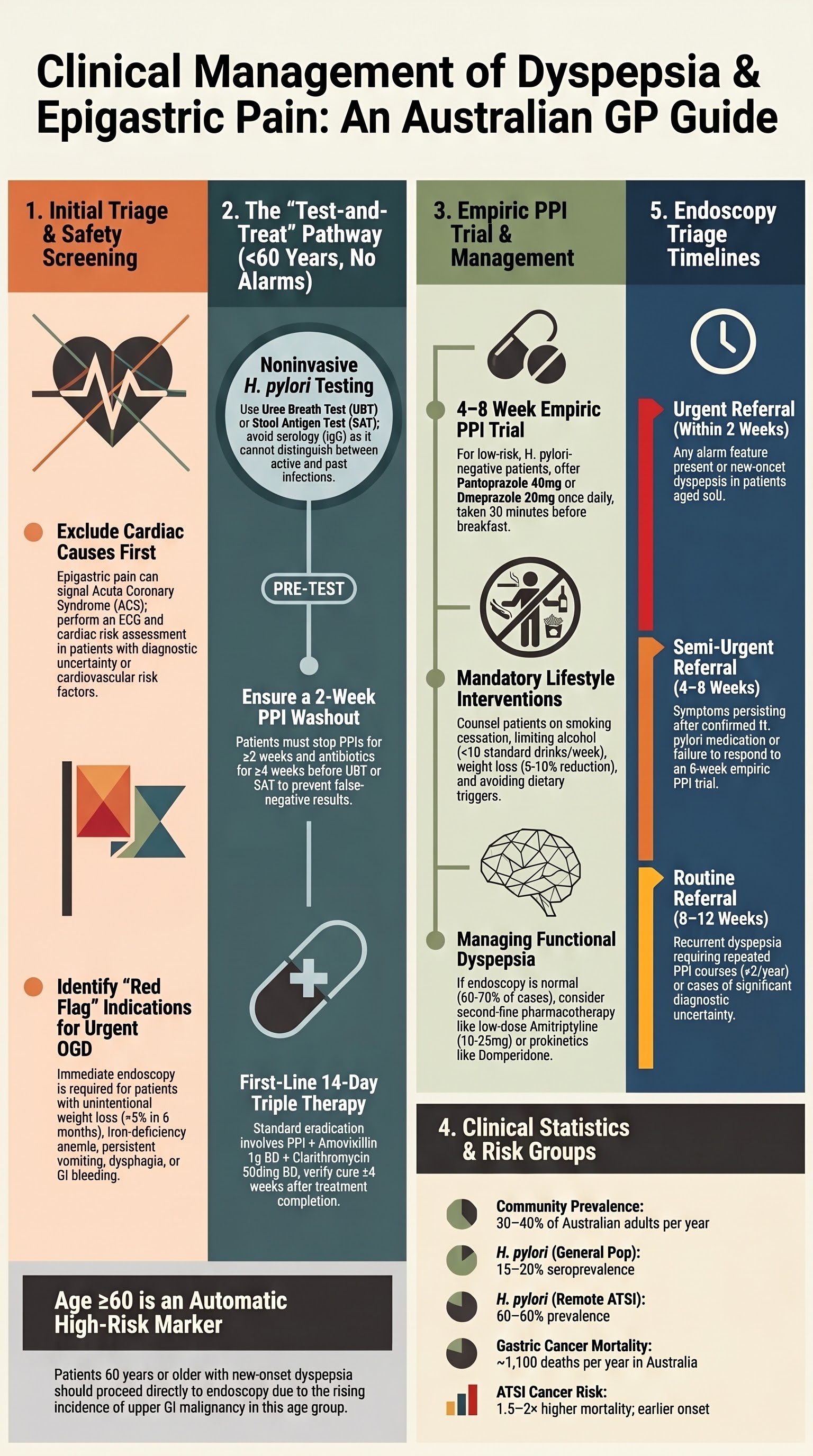
- Always differentiate dyspepsia from cardiac pain — epigastric discomfort may represent acute coronary syndrome; perform an ECG and cardiac risk assessment when there is diagnostic uncertainty.
- Identify alarm features (weight loss, unintentional >5% in 6 months; unexplained iron-deficiency anaemia; persistent vomiting; dysphagia; GI bleeding; progressive symptoms) and age ≥60 years as indications for prompt endoscopy (OGD).
- Review medications — NSAIDs, aspirin, corticosteroids, bisphosphonates, SSRIs, anticoagulants — and counsel regarding alcohol cessation, smoking cessation, and weight management as first-line lifestyle interventions.
- Noninvasive H. pylori testing with urea breath test (UBT) or stool antigen test (SAT) is recommended for all patients <60 years without alarm features; serology alone is insufficient for active infection diagnosis.
- If H. pylori is detected, treat with a guideline-based eradication regimen — first-line: PPI + amoxicillin 1 g BD + clarithromycin 500 BD for 14 days; second-line or bismuth quadruple therapy for treatment failure.
- Confirm H. pylori eradication at ≥4 weeks after completing treatment and ≥2 weeks off PPI using UBT or SAT — do not rely on repeat endoscopy biopsy alone.
- For low-risk patients <60 years without alarm features: offer a 4–8 week empiric PPI trial (e.g., pantoprazole 40 mg or omeprazole 20 mg once daily) before considering referral or endoscopy.
- Patients ≥60 years with new-onset dyspepsia should proceed directly to endoscopy — the incidence of upper GI malignancy rises significantly after age 60 in the Australian population.
- Refer for endoscopy if symptoms persist or relapse despite confirmed H. pylori eradication and an adequate PPI trial, or if alarm features develop at any age.
- Aboriginal and Torres Strait Islander peoples have higher H. pylori prevalence, higher rates of gastric cancer presenting at younger ages, and reduced access to endoscopy in remote communities — lower the threshold for investigation and referral.
Introduction & Australian Epidemiology
Dyspepsia encompasses a spectrum of upper gastrointestinal symptoms including epigastric pain, burning, postprandial fullness, early satiation, bloating, and nausea. It is one of the most common presentations in Australian general practice, accounting for up to 5% of all GP encounters and is the most frequent reason for gastroenterology referral.
In Australia, community-based surveys estimate that 30–40% of adults experience dyspeptic symptoms in any given year, though only a minority seek medical attention. The annual prevalence of functional (non-ulcer) dyspepsia is approximately 15–20%, while peptic ulcer disease affects 5–10% of the population at some point in their lives. Gastro-oesophageal reflux disease (GORD) overlaps significantly and may co-exist.
The economic burden is substantial. Dyspepsia-related consultations, endoscopies, proton-pump inhibitor (PPI) prescriptions, and hospital admissions cost the Australian healthcare system an estimated .5–2 billion annually. PPIs remain among the most prescribed PBS-listed medications, with >20 million prescriptions dispensed per year nationally.
Key Australian Epidemiological Data
| Metric | Data |
|---|---|
| Community prevalence of dyspepsia | 30–40% per year |
| Functional (non-ulcer) dyspepsia | ~15–20% of adults |
| H. pylori seroprevalence (general population) | ~15–20% (declining) |
| H. pylori seroprevalence (ATSI communities) | ~60–80% in remote communities |
| Annual PPI prescriptions (PBS) | >20 million |
| Gastric cancer incidence (Australia) | ~2,300 new cases/year; mortality ~1,100/year |
Initial Assessment & Alarm Features
The initial evaluation of a patient presenting with dyspepsia or epigastric pain requires a systematic approach to (1) exclude cardiac causes, (2) identify modifiable risk factors and offending medications, and (3) detect alarm features that mandate urgent investigation.
Step 1: Exclude Cardiac Pain
Alarm Features Requiring Urgent Endoscopy
| Alarm Feature | Clinical Significance | Action |
|---|---|---|
| Unintentional weight loss (>5% body weight in 6 months) | Suggests malignancy or severe organic disease | Urgent OGD within 2 weeks |
| Progressive dysphagia | Oesophageal or gastric cardia malignancy; peptic stricture | Urgent OGD within 2 weeks |
| Persistent vomiting | Gastric outlet obstruction, malignancy, severe gastroparesis | Urgent OGD; consider CT abdomen |
| GI bleeding (haematemesis, melaena, positive faecal occult blood) | Peptic ulcer with active bleeding, malignancy, varices | Immediate OGD if haemodynamically significant |
| Iron-deficiency anaemia (unexplained) | Occult GI blood loss from ulcer, malignancy, coeliac disease | OGD + colonoscopy |
| Palpable abdominal mass | Advanced malignancy or large GIST | Urgent CT abdomen + OGD |
| Age ≥60 years with new-onset dyspepsia | Significantly increased risk of upper GI malignancy | Direct-to-endoscopy pathway |
Severity Assessment
Medication Review — Common Offending Agents
| Medication Class | Mechanism | Management |
|---|---|---|
| NSAIDs (ibuprofen, naproxen, diclofenac, celecoxib) | COX-1 inhibition → reduced mucosal prostaglandins, direct mucosal injury | Cease if possible; switch to paracetamol; if ongoing need, use lowest dose + co-prescribe PPI |
| Low-dose aspirin (100–300 mg) | Mucosal injury, impairs ulcer healing | Continues if cardiovascular indication; add PPI for gastroprotection |
| Corticosteroids (especially with NSAIDs) | Synergistic mucosal damage when combined with NSAIDs | Add PPI if concurrent NSAID use; avoid combination where possible |
| Bisphosphonates (alendronate, risedronate) | Oesophageal and gastric mucosal irritation | Review necessity; ensure correct administration technique |
| SSRIs / SNRIs | Increased GI bleeding risk (serotonin-mediated platelet effects) | Consider PPI co-prescription if concurrent antiplatelet/anticoagulant |
Noninvasive H. pylori Testing & Treatment
Test-and-Treat Strategy
For patients <60 years with dyspepsia and no alarm features, the recommended approach in Australian guidelines is the test-and-treat strategy: perform a noninvasive test for Helicobacter pylori and treat if positive, rather than proceeding directly to endoscopy. This strategy is cost-effective, reduces unnecessary endoscopies by approximately 30–40%, and achieves symptom resolution in 20–30% of dyspeptic patients.
Noninvasive Diagnostic Tests
Pre-Test Requirements
H. pylori Eradication Regimens
First-Line Therapy — Standard Triple Therapy (14 days)
Second-Line Therapy — Bismuth Quadruple Therapy (14 days)
For patients who fail first-line triple therapy, or in areas of high clarithromycin resistance, bismuth quadruple therapy is the recommended second-line regimen.
Confirming Eradication — Test of Cure
If first-line therapy fails, options include:
- Bismuth quadruple therapy (as above) — preferred second-line
- PPI + amoxicillin 1 g BD + levofloxacin 500 mg daily + bismuth — third-line option; local fluoroquinolone resistance data should guide use
- Referral for culture-guided therapy — consider in patients with ≥2 eradication failures; available at select reference laboratories (e.g., Royal Melbourne Hospital Microbiology, Westmead Hospital)
Empiric PPI Trial
For low-risk patients <60 years without alarm features, an empiric proton-pump inhibitor trial is a reasonable initial management strategy, either after a negative H. pylori test or as a first-line approach if testing is not immediately available. This approach is endorsed by the Australian Therapeutic Guidelines and the Gastroenterological Society of Australia (GESA).
When to Use Empiric PPI
- Age <60 years
- No alarm features (see alarm feature table above)
- H. pylori testing negative or test-and-treat completed
- Predominantly epigastric pain/burning (suggestive of functional dyspepsia or mild peptic ulcer disease)
- NSAID-related dyspepsia (after NSAID cessation or with ongoing NSAID use + gastroprotection)
PPI Dosing for Empiric Trial
PPI Trial Response Assessment
Adjunctive and Lifestyle Measures
- Weight loss if BMI ≥25 — even 5–10% reduction improves symptoms
- Smoking cessation — reduces ulcer recurrence and improves mucosal healing
- Alcohol reduction — aim for <10 standard drinks/week; avoid binge drinking
- Dietary modifications — avoid late-night eating, large meals, known trigger foods (spicy, fatty, citrus, caffeine, chocolate)
- Elevate head of bed if nocturnal reflux symptoms
- Stress management — psychological comorbidity (anxiety, depression) is common in functional dyspepsia; consider CBT, low-dose TCAs (amitriptyline 10–25 mg nocte) if refractory
When to Refer for Endoscopy
Upper gastrointestinal endoscopy (oesophagogastroduodenoscopy, OGD) is the definitive investigation for dyspepsia and epigastric pain when indicated. In Australia, OGD is widely available through public and private gastroenterology services, with typical wait times of 2–4 weeks for urgent referrals and 4–12 weeks for routine referrals in the public system.
Indications for Endoscopy — Summary
| Indication | Urgency | Timeframe |
|---|---|---|
| Any alarm feature (weight loss, dysphagia, bleeding, anaemia, vomiting, mass) | Urgent | Within 2 weeks |
| New-onset dyspepsia age ≥60 years | Urgent | Within 2–4 weeks |
| Symptoms persist/relapse after confirmed H. pylori eradication + adequate PPI trial | Semi-urgent | Within 4–6 weeks |
| Failure to respond to 8-week empiric PPI trial | Semi-urgent | Within 4–8 weeks |
| Recurrent dyspepsia requiring repeated courses of PPI (>2 per year) | Routine | Within 8–12 weeks |
| Patient preference / diagnostic uncertainty | Routine | Within 8–12 weeks |
What Endoscopy Achieves
- Visualisation: Oesophagus, stomach, and duodenum — identifies erosive oesophagitis, peptic ulcers, malignancy, Barrett's oesophagus, gastric polyps, and other structural pathology
- Biopsy: CLO test (rapid urease test) for H. pylori at endoscopy; histopathological assessment for H. pylori, intestinal metaplasia, dysplasia, and malignancy
- Therapeutic intervention: Haemostasis for bleeding ulcers, dilation of strictures, endoscopic mucosal resection for early neoplasia
Pathway Algorithm
Functional Dyspepsia — Second-Line Pharmacotherapy
Special Populations
Pregnancy
Paediatrics
Elderly (≥65 years)
Renal Impairment
Hepatic Impairment
Immunocompromised
📚 References
- 1. Gastroenterological Society of Australia (GESA). Clinical update: Dyspepsia and H. pylori. Sydney: GESA; 2023. Available at: gesa.org.au.
- 2. Ford AC, Marwaha A, Sood R, Moayyedi P. Global prevalence of, and risk factors for, uninvestigated dyspepsia: a meta-analysis. Gut. 2015;64(7):1049–1057.
- 3. Talley NJ, Ford AC. Functional dyspepsia. N Engl J Med. 2015;373(19):1853–1863.
- 4. Malfertheiner P, Megraud F, Rokkas T, et al. Management of Helicobacter pylori infection: the Maastricht VI/Florence consensus report. Gut. 2022;71(9):1724–1762.
- 5. Chey WD, Leontiadis GI, Howden CW, Moss SF. ACG Clinical Guideline: Treatment of Helicobacter pylori Infection. Am J Gastroenterol. 2017;112(2):212–239.
- 6. National Health and Medical Research Council (NHMRC). Clinical practice guideline: Evidence review for the investigation and management of dyspepsia. Canberra: NHMRC; 2020.
- 7. Australian Institute of Health and Welfare (AIHW). Cancer in Aboriginal & Torres Strait Islander people of Australia. Canberra: AIHW; 2023.
- 8. Holtmann G, Shah A, Morrison M. Pathophysiology of functional gastrointestinal disorders: a holistic overview. Dig Dis. 2017;35(Suppl 1):5–13.
- 9. Royal Australian College of General Practitioners (RACGP). Prescribing drugs of dependence in general practice: Part B — Benzodiazepines and PPIs. Melbourne: RACGP; 2022.
- 10. Menon S, Nightingale P, Trivedi S, et al. Systematic review and meta-analysis of H. pylori infection in Aboriginal Australians. Intern Med J. 2020;50(9):1045–1054.
- 11. Pharmaceutical Benefits Scheme (PBS). Australian Government Department of Health. Schedule of Pharmaceutical Benefits. Canberra: Commonwealth of Australia; 2024.
- 12. Drossman DA, Hasler WL. Rome IV — Functional GI disorders: disorders of gut-brain interaction. Gastroenterology. 2016;150(6):1257–1261.
- 13. Eusebi LH, Rabitti S, Artesiani ML, et al. Proton pump inhibitors: risks of long-term use. J Gastroenterol Hepatol. 2017;32(7):1295–1302.
- 14. RHDAustralia (ASHM). Recommendations for the clinical management of H. pylori in Aboriginal and Torres Strait Islander populations. Darwin: RHDAustralia; 2021.