📋 Key Information Summary
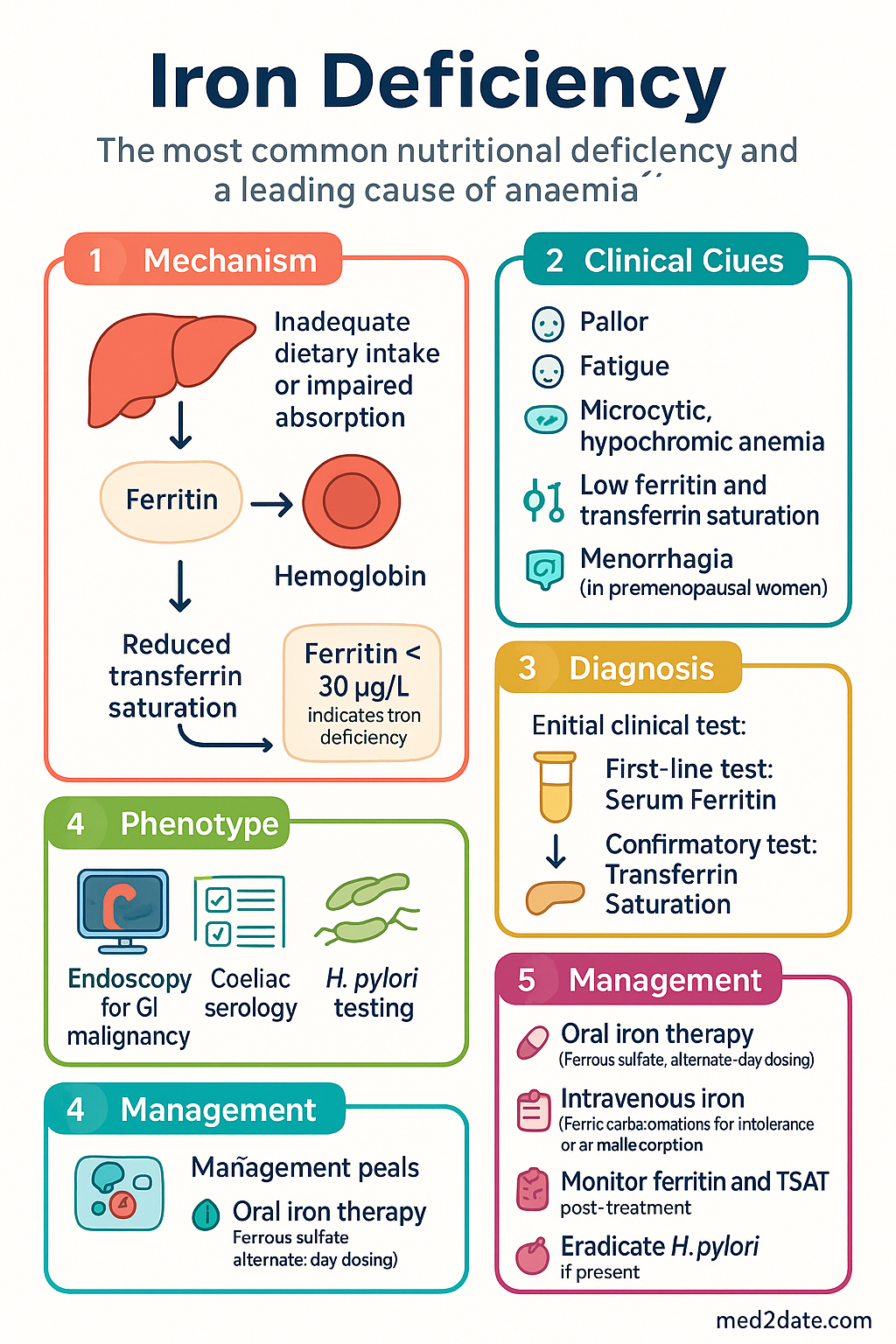
- Iron deficiency is the most common nutritional deficiency worldwide and a leading cause of anaemia in Australia.
- A ferritin level <30 µg/L is diagnostic of iron deficiency in otherwise well patients; in the context of inflammation (e.g., CRP >5 mg/L), a threshold of <100 µg/L is more appropriate.
- Transferrin saturation (TSAT) <20% supports the diagnosis, especially when ferritin is equivocal.
- Investigation of the underlying cause is mandatory, not just treatment of the anaemia.
- In men and postmenopausal women, bidirectional endoscopy (OGD and colonoscopy) is the standard of care to exclude gastrointestinal malignancy.
- Coeliac serology (tissue transglutaminase IgA) should be performed in all patients with iron deficiency, even without classic GI symptoms.
- H. pylori infection impairs iron absorption and its eradication is a crucial part of management.
- For premenopausal women, gynaecological causes (e.g., menorrhagia) are the most common aetiology, but GI investigation is warranted if symptoms persist or red flags are present.
- Oral iron is first-line therapy; alternate-day, single-dose regimens optimise absorption and reduce side effects.
- Intravenous iron is indicated for intolerance, malabsorption (e.g., IBD, coeliac), ongoing significant losses, CKD, pregnancy (2nd/3rd trimester), and perioperative optimisation.
- Ferric carboxymaltose allows large-dose infusion but carries a risk of hypophosphataemia; monitoring is required.
- All IV iron formulations carry a risk of hypersensitivity; facilities for resuscitation must be available.
- Aboriginal and Torres Strait Islander peoples experience a higher burden of iron deficiency due to complex socio-economic factors, dietary patterns, and higher rates of helminth infection.
🎧 Audio Brief
Investigation of Iron Deficiency
A systematic approach is required to confirm iron deficiency, assess its severity, and identify the underlying cause. The investigation strategy is guided by patient demographics, clinical presentation, and comorbidities.
1. Confirming Iron Deficiency and Assessing Severity
| Test | Diagnostic Threshold | Key Considerations |
|---|---|---|
| Serum Ferritin | <30 µg/L (low) | Acute-phase reactant. In the presence of inflammation (e.g., CRP >5 mg/L, chronic infection, malignancy, CKD, liver disease), a higher threshold of <100 µg/L is recommended to diagnose iron deficiency. |
| Transferrin Saturation (TSAT) | <20% | More specific in inflammatory states. Useful for confirming functional iron deficiency when ferritin is normal or high (e.g., in CKD or IBD). |
| Full Blood Count (FBC) | Microcytic, hypochromic anaemia | MCV and MCH are late findings. Low reticulocyte haemoglobin content (CHr) or percentage of hypochromic red cells (%HRC) are early indicators of iron-deficient erythropoiesis. |
2. Identifying the Underlying Cause
The investigation strategy follows the British and American Gastroenterological Associations' approach, tailored to Australian practice.
- Coeliac Serology: Tissue transglutaminase IgA (tTG-IgA) with total IgA. Perform in ALL patients with iron deficiency, regardless of GI symptoms.
- H. pylori Testing: Urea breath test or stool antigen test. Eradication is indicated if positive, as it contributes to IDA.
- Gynaecological Assessment: In premenopausal women, quantify menstrual blood loss (e.g., pictorial blood loss chart). Pelvic ultrasound if indicated.
Indication: Mandatory for men and postmenopausal women with iron deficiency anaemia (IDA) after excluding obvious non-GI causes. Consider in premenopausal women with IDA refractory to oral iron, red flag symptoms, or a family history of GI malignancy.
Procedure: Oesophago-gastro-duodenoscopy (OGD) with duodenal biopsies (to rule out coeliac disease) AND colonoscopy. In Australia, these are often performed as a single session under sedation (MBS item 30473).
Definition: Persistent or recurrent IDA after negative bidirectional endoscopy.
Next Step: Video capsule endoscopy (VCE, MBS item 11820) to visualise the small bowel. It is the investigation of choice for suspected small bowel angioectasias, Crohn's disease, or tumours.
Further Imaging: CT enterography or device-assisted enteroscopy (e.g., double-balloon enteroscopy) for therapeutic intervention if a lesion is identified on VCE.
Treatment of Iron Deficiency
The goals of treatment are to replenish iron stores, correct anaemia, and treat the underlying cause. The choice between oral and intravenous iron depends on the clinical context, urgency, and patient factors.
1. Oral Iron Therapy
2. Intravenous Iron Therapy
Indications for IV Iron:
- Oral iron intolerance or non-compliance.
- Inadequate absorption due to GI disease (e.g., active IBD, coeliac disease, prior gastric bypass).
- Ongoing blood losses exceeding the capacity for oral replacement (e.g., chronic haemodialysis, hereditary haemorrhagic telangiectasia).
- Chronic Kidney Disease (CKD) Stage 4-5, especially with ESA therapy.
- Pregnancy (2nd and 3rd trimester) when oral iron is ineffective or not tolerated.
- Perioperative optimisation for major surgery when time is limited.
| Formulation | Max Single Dose | Key Considerations | PBS Status |
|---|---|---|---|
| Ferric Carboxymaltose (Ferinject®) | 1000 mg | Allows large-dose infusion in ~15 mins. Risk of hypophosphataemia (can be prolonged/symptomatic). Check serum phosphate at 2-4 weeks post-infusion. | ⚠ PBS Authority Required |
| Iron Sucrose (Venofer®) | 200 mg per infusion | Extensive safety data. Well-tolerated. Requires multiple infusions for larger deficits. | ⚠ PBS Authority Required |
| Derisomaltose Iron (Monofer®) | 1500 mg | High dose in a single infusion. Lower risk of hypophosphataemia compared to ferric carboxymaltose. | ⚠ PBS Authority Required |
Monitoring After IV Iron:
- Check FBC and iron studies (ferritin, TSAT) 8–12 weeks post-infusion to assess response.
- Monitor for delayed hypersensitivity reactions (up to 24 hours post-infusion).
- For ferric carboxymaltose, check serum phosphate at 2–4 weeks. Symptomatic hypophosphataemia may require phosphate replacement and vitamin D assessment.
Aboriginal and Torres Strait Islander Health Considerations
Iron deficiency anaemia is significantly more prevalent among Aboriginal and Torres Strait Islander peoples, particularly women of childbearing age and children, contributing to a higher burden of chronic disease. Management requires a culturally safe, holistic approach.
📚 References
- 1. Pasricha SR, Tye-Din J, Muckenthaler MU, Swinkels DW. Iron deficiency. Lancet. 2021;397(10270):233-248.
- 2. Goddard AF, James MW, McIntyre AS, Scott BB. Guidelines for the management of iron deficiency anaemia. Gut. 2011;60(10):1309-1316.
- 3. Ko CW, Siddique SM, Patel A, et al. AGA Clinical Practice Guidelines on the Gastrointestinal Evaluation of Iron Deficiency Anemia in Adults. Gastroenterology. 2020;159(3):1085-1094.
- 4. Australian Institute of Health and Welfare (AIHW). Iron deficiency. AIHW, Canberra. 2023.
- 5. RACGP. Management of iron deficiency in general practice. RACGP, Melbourne. 2022.
- 6. Kidney Disease: Improving Global Outcomes (KDIGO) Anemia Work Group. KDIGO Clinical Practice Guideline for Anemia in Chronic Kidney Disease. Kidney Int Suppl. 2012;2(4):279-335.
- 7. Auerbach M, Adamson JW. How I diagnose and treat iron deficiency anemia. Am J Hematol. 2016;91(1):39-46.
- 8. Tolkien Z, Stecher L, Mander AP, Pereira DI, Powell JJ. Ferrous sulfate supplementation causes significant gastrointestinal side-effects in adults: a systematic review and meta-analysis. PLoS One. 2015;10(2):e0117383.
- 9. Australian Government Department of Health. Pharmaceutical Benefits Scheme (PBS) Item Reports: Iron Replacement Products. Accessed 2024.
- 10. National Aboriginal Community Controlled Health Organisation (NACCHO). Aboriginal and Torres Strait Islander Health Performance Framework: Iron Deficiency Anaemia. NACCHO, Canberra. 2023.
- 11. Medical Services Advisory Committee (MSAC). Public Summary Document: Application No. 1615 – Video Capsule Endoscopy. MSAC, Canberra. 2021.
- 12. Lim W, Afzal R, Bhagat K, et al. Intravenous iron: a systematic review and meta-analysis of efficacy and safety. Med J Aust. 2023;218(10):473-480.