📋 Key Information Summary
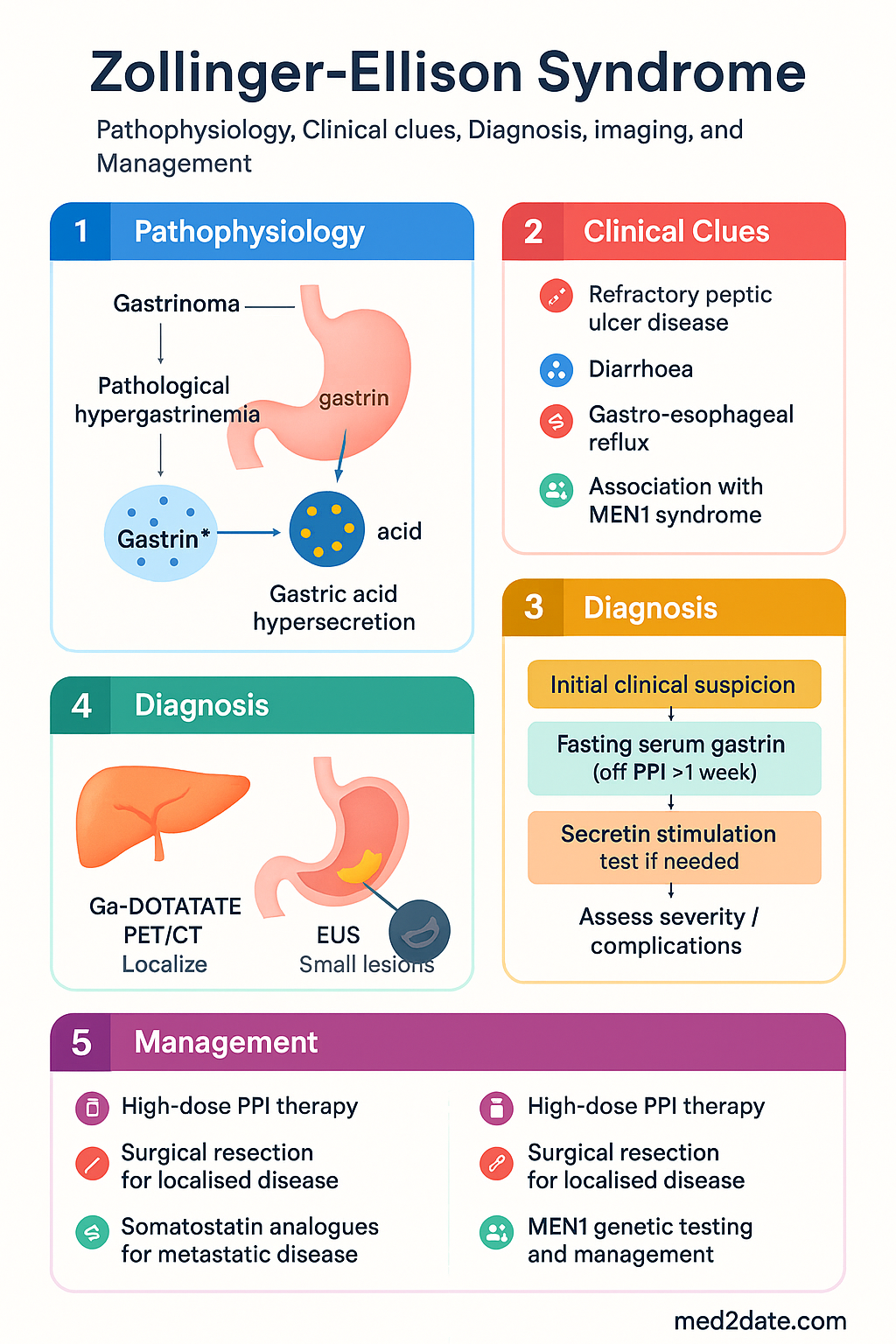
- Zollinger-Ellison Syndrome (ZES) is caused by a gastrin-secreting neuroendocrine tumour (gastrinoma) leading to pathological hypergastrinaemia and gastric acid hypersecretion.
- Approximately 25% of gastrinomas occur in the setting of Multiple Endocrine Neoplasia type 1 (MEN1) — always screen for hyperparathyroidism, pituitary adenomas, and germline MEN1 mutations.
- Classic triad: refractory peptic ulcer disease (often atypical locations such as jejunum), diarrhoea, and gastro-oesophageal reflux — suspect ZES in patients with recurrent ulcers despite adequate PPI therapy.
- Diagnosis requires fasting serum gastrin ≥1000 pg/mL with gastric pH <2, or a positive secretin stimulation test if gastrin is moderately elevated (100–1000 pg/mL).
- Patients must discontinue PPIs for ≥1 week before fasting gastrin testing to avoid false negatives; however, this carries risk of rebound acid hypersecretion — discuss risk-benefit with a gastroenterologist.
- Chromogranin A is a useful supportive marker and may help monitor treatment response in metastatic disease.
- Localisation: somatostatin receptor imaging with 68Ga-DOTATATE PET/CT is the preferred modality; EUS is essential for small pancreatic/duodenal lesions not seen on cross-sectional imaging.
- High-dose PPI (e.g., omeprazole 60–120 mg/day PO or equivalent) is the cornerstone of acid suppression — lifelong therapy is usually required.
- Localised gastrinoma (no metastases): surgical resection offers the only chance of cure; sporadic tumours have higher resectability than MEN1-associated tumours.
- Metastatic gastrinoma: somatostatin analogues (octreotide LAR, lanreotide Autogel) for symptom and tumour control; peptide receptor radionuclide therapy (PRRT, e.g., 177Lu-DOTATATE) for progressive somatostatin receptor-positive disease; consider systemic chemotherapy (temozolomide ± capecitabine) or targeted therapy (everolimus) for refractory cases.
- Aboriginal and Torres Strait Islander Australians may have reduced access to specialist diagnostics and surgical services; coordinate with regional tertiary centres and use telehealth where available.
- The majority of gastrinomas are malignant (60–70%), but well-differentiated neuroendocrine tumours have relatively favourable 5-year survival (60–90%) compared to poorly differentiated neuroendocrine carcinomas.
🎧 Audio Brief
Zollinger-Ellison Syndrome
Zollinger-Ellison Syndrome (ZES) is a rare clinical syndrome resulting from autonomous secretion of gastrin by a neuroendocrine tumour (gastrinoma), leading to profound gastric acid hypersecretion. Gastrinomas are the most common functional pancreatic neuroendocrine tumour (pNET) after insulinoma, with an estimated incidence of 0.5–2 per million population per year in Australia.
Refractory or Recurrent Peptic Ulcer Disease
The hallmark of ZES is peptic ulcer disease that is refractory to standard-dose proton pump inhibitor (PPI) therapy or recurs after definitive surgical treatment (e.g., after successful Helicobacter pylori eradication). Patients often present with multiple ulcers, ulcers that are large (>2 cm), or ulcers in atypical locations — most notably the second and third portions of the duodenum and the jejunum. Jejunal ulcers are particularly suspicious for ZES and should prompt investigation.
Diarrhoea
Secretory diarrhoea occurs in 30–75% of patients with ZES and may be the presenting symptom, even in the absence of overt peptic ulceration. The mechanism involves: (1) direct damage to the small bowel mucosa from excess acid, (2) inactivation of pancreatic lipase by low intraduodenal pH leading to fat malabsorption, and (3) increased intestinal motility. The diarrhoea is typically large-volume, watery, and often improves with PPI therapy — a useful diagnostic clue.
Gastro-Oesophageal Reflux and Oesophagitis
Severe gastro-oesophageal reflux disease (GORD) and erosive oesophagitis are common in ZES, occurring in up to 60% of patients. The reflux may be resistant to standard PPI doses and may progress to Barrett's oesophagus in long-standing untreated cases. Hiatus hernia is frequently present. Barrett's oesophagus has been reported in 26% of ZES patients in some series.
Association with MEN1
Approximately 20–30% of gastrinomas occur in the context of MEN1 syndrome, an autosomal dominant condition caused by inactivating mutations in the MEN1 tumour suppressor gene (chromosome 11q13). MEN1-associated ZES has distinct features compared to sporadic ZES:
| Feature | Sporadic ZES | MEN1-Associated ZES |
|---|---|---|
| Proportion of ZES cases | ~75% | ~25% |
| Tumour location | Duodenal wall (40–50%), pancreas | Usually duodenal, often small (<1 cm), multiple |
| Malignancy risk | Higher (liver metastases in ~30%) | Lower liver metastases risk |
| Surgical cure rate | ~30–40% | <5% (multifocal disease) |
| Associated endocrinopathies | None | Primary hyperparathyroidism (95%), pituitary adenoma (30–40%), adrenal/other |
The MEN1 clinical syndrome includes the "3 Ps": Parathyroid hyperplasia (primary hyperparathyroidism, present in >90% of MEN1 patients), Pancreatic neuroendocrine tumours (including gastrinoma), and Pituitary adenomas (most commonly prolactinoma). Primary hyperparathyroidism may precede or co-present with ZES and can worsen hypercalcaemia-mediated gastric acid secretion, compounding acid hypersecretion.
Diagnostic Workup
The diagnosis of ZES requires demonstration of inappropriate (pathological) hypergastrinaemia in the setting of gastric acid hypersecretion. A systematic diagnostic approach is essential, as misdiagnosis delays appropriate treatment and may lead to life-threatening complications.
Fasting Serum Gastrin
Fasting serum gastrin is the primary biochemical test for ZES. The patient must fast for ≥12 hours. Critically, proton pump inhibitors (PPIs) must be discontinued for ≥1 week before testing, as PPIs directly suppress acid and cause secondary (reactive) hypergastrinaemia, leading to false-positive results. Histamine H₂-receptor antagonists may be substituted during the washout period but should also be stopped 48–72 hours before testing.
| Fasting Serum Gastrin | Interpretation |
|---|---|
| <100 pg/mL | Normal — ZES effectively excluded |
| 100–1000 pg/mL | Equivocal — requires further testing (secretin stimulation, gastric pH) |
| ≥1000 pg/mL with gastric pH <2 | Diagnostic of ZES (diagnostic criterion met) |
Gastric pH <2 with Hypergastrinaemia
Concurrent measurement of fasting gastric pH (via nasogastric aspiration or at endoscopy) is essential. A gastric pH <2 in the setting of hypergastrinaemia confirms acid hypersecretion. If the fasting gastrin is moderately elevated (100–1000 pg/mL) but gastric pH is ≥2, acid hypersecretion is not present and alternative causes of hypergastrinaemia should be considered (atrophic gastritis, PPI use, renal failure).
Secretin Stimulation Test
When fasting gastrin is equivocally elevated (100–1000 pg/mL), the secretin stimulation test provides definitive differentiation. Intravenous secretin (2 units/kg bolus) is administered, and serum gastrin is measured at 2, 5, 10, 15, and 20 minutes post-injection. A rise in serum gastrin of ≥120 pg/mL above baseline is diagnostic of ZES. Sensitivity is approximately 85–95%. This test requires specialist gastroenterology or endocrine laboratory capability.
Chromogranin A
Chromogranin A (CgA) is a non-specific neuroendocrine tumour marker elevated in 80–100% of gastrinomas. It is useful as a supportive test and for monitoring disease burden and treatment response in metastatic disease. CgA may be falsely elevated by PPI use, renal impairment, atrophic gastritis, or chronic atrophic gastritis with enterochromaffin-like (ECL) cell hyperplasia. Reference range: <100 μg/L (varies by assay).
68Ga-DOTATATE PET/CT
68Ga-DOTATATE PET/CT (somatostatin receptor imaging) is now the gold-standard functional imaging modality for localising gastrinomas and detecting metastatic disease. It exploits the high expression of somatostatin receptor subtype 2 (SSTR2) on well-differentiated neuroendocrine tumours. Sensitivity for primary gastrinoma detection: 85–95%, compared to 50–70% for conventional CT/MRI. This scan is also essential for selecting patients eligible for peptide receptor radionuclide therapy (PRRT). It is available at major Australian PET centres (MBS item 61646 under restricted indications).
Endoscopic Ultrasound (EUS)
EUS is the most sensitive imaging technique for detecting small pancreatic and duodenal gastrinomas, many of which are <1–2 cm and missed by cross-sectional imaging (CT, MRI). EUS also allows fine-needle aspiration (FNA) for histological confirmation. In MEN1-associated ZES, EUS is critical for identifying multiple small duodenal gastrinomas. EUS should be performed at centres with neuroendocrine tumour expertise.
MEN1 Genetic Testing
Germline MEN1 mutation testing is recommended for all patients with confirmed ZES, as the result alters surgical strategy and long-term surveillance. Testing is performed on peripheral blood DNA using next-generation sequencing or Sanger sequencing of the MEN1 gene (chromosome 11q13). If a pathogenic mutation is identified, cascade screening of first-degree relatives is recommended. In Australia, MEN1 genetic testing is available through public genetics services and some private pathology providers.
Management
Management of ZES has two parallel goals: (1) control of gastric acid hypersecretion to prevent peptic ulcer complications, and (2) treatment of the gastrinoma itself, ranging from curative surgical resection to systemic therapy for metastatic disease.
High-Dose PPI for Acid Control
High-dose proton pump inhibitor (PPI) therapy is the cornerstone of acid suppression in ZES and is required lifelong in most patients. The goal is to maintain basal acid output (BAO) <10 mEq/h (or <5 mEq/h if prior gastric surgery). Therapy should be commenced immediately upon diagnosis.
Surgical Resection of Localised Gastrinoma
Surgical resection is the only potentially curative treatment for gastrinoma. It should be considered in all patients with localised disease (no liver or distant metastases) after thorough preoperative localisation.
Sporadic gastrinoma: Enucleation or formal resection of the gastrinoma with regional lymphadenectomy. Duodenal gastrinomas require careful exploration of the duodenal wall (including duodenotomy) as these may be very small and multifocal. Cure rates of 30–40% have been reported in experienced centres.
MEN1-associated gastrinoma: Surgery is more controversial due to the multifocal nature of duodenal gastrinomas in MEN1. Current guidelines suggest surgery when the primary gastrinoma is >2 cm (increased metastatic risk), with lymph node sampling. The role of prophylactic surgery in MEN1 patients with small gastrinomas remains under investigation.
Somatostatin Analogues
Somatostatin analogues (SSAs) bind somatostatin receptors on gastrinoma cells, inhibiting hormone secretion and exerting antiproliferative effects. They are indicated for: (1) symptomatic control when PPI alone is insufficient, (2) antiproliferative effect in well-differentiated metastatic NETs, and (3) as a bridge to PRRT.
Peptide Receptor Radionuclide Therapy (PRRT)
PRRT with 177Lu-DOTATATE (Lutathera®) is a targeted radionuclide therapy that delivers beta radiation to somatostatin receptor-expressing tumour cells. It is indicated for progressive, well-differentiated, somatostatin receptor-positive gastroenteropancreatic NETs, including gastrinomas.
Regimen: 177Lu-DOTATATE 7.4 GBq IV infusion every 8 weeks for 4 cycles, co-administered with amino acid solution (arginine/lysine) for renal protection. Pre-treatment requires positive somatostatin receptor imaging (68Ga-DOTATATE PET/CT) confirming receptor expression.
Evidence: The NETTER-1 trial demonstrated significantly improved progression-free survival with 177Lu-DOTATATE plus octreotide LAR versus high-dose octreotide LAR alone in advanced midgut NETs (HR 0.21; P<0.001). While gastrinomas were not the primary population studied, PRRT is widely used for progressive pancreatic/duodenal NETs based on extrapolation and cohort data.
Australian availability: 177Lu-DOTATATE (Lutathera®) is TGA-approved and PBS-listed as an Authority Required benefit for progressive, well-differentiated, SSTR-positive gastroenteropancreatic NETs. It is administered at designated nuclear medicine centres across Australia (e.g., Peter MacCallum Cancer Centre, Royal North Shore Hospital, Royal Adelaide Hospital, Sir Charles Gairdner Hospital).
Systemic Therapy for Metastatic Disease
For patients with progressive metastatic gastrinoma not controlled by somatostatin analogues and PRRT, or with aggressive poorly differentiated histology, additional systemic therapies may be considered:
| Agent | Regimen | Indication | PBS Status |
|---|---|---|---|
| Temozolomide + Capecitabine | Temozolomide 150–200 mg/m² PO days 1–5 q28d + Capecitabine 1500 mg/m²/day PO days 1–14 q28d | Progressive pancreatic NET (including gastrinoma); well-differentiated | ✔ PBS General Benefit (temozolomide); ✔ PBS (capecitabine) |
| Everolimus | 10 mg PO daily | Advanced, progressive, well-differentiated pancreatic NET | ⛔ Authority Required (NET) |
| Sunitinib | 37.5 mg PO daily (continuous dosing) | Progressive, well-differentiated pancreatic NET | ⛔ Authority Required |
| Cisplatin/Etoposide | Standard NE regimen | Poorly differentiated neuroendocrine carcinoma (high-grade) | ✔ PBS General Benefit |
All systemic therapy decisions should be made within a multidisciplinary team (MDT) meeting with neuroendocrine tumour expertise, including endocrinology, gastroenterology, HPB surgery, nuclear medicine, medical oncology, and radiology.
Special Populations
ATSI Health Considerations
While Zollinger-Ellison Syndrome is rare and specific ATSI prevalence data are limited, Aboriginal and Torres Strait Islander Australians face systemic barriers to diagnosis and management of rare endocrine conditions. The following considerations apply:
📚 References
- 1. Ito T, Jensen RT. Zollinger-Ellison syndrome. In: Feldman M, Friedman LS, Brandt LJ, eds. Sleisenger and Fordtran's Gastrointestinal and Liver Disease. 11th ed. Philadelphia: Elsevier; 2021:512–537.
- 2. Jensen RT, Niederle B, Mitry E, et al. Gastrinoma (duodenal and pancreatic). Neuroendocrinology. 2006;84(3):173–182.
- 3. Falconi M, Eriksson B, Kaltsas G, et al. ENETS Consensus Guidelines Update for the Management of Patients with Functional Pancreatic Neuroendocrine Tumors and Non-Functional Pancreatic Neuroendocrine Tumors. Neuroendocrinology. 2016;103(2):153–171.
- 4. Strosberg J, El-Haddad G, Wolin E, et al. Phase 3 trial of 177Lu-DOTATATE for midgut neuroendocrine tumors (NETTER-1). N Engl J Med. 2017;376(2):125–135.
- 5. Thakker RV, Newey PJ, Walls GV, et al. Clinical practice guidelines for multiple endocrine neoplasia type 1 (MEN1). J Clin Endocrinol Metab. 2012;97(9):2990–3011.
- 6. Metz DC, Jensen RT. Gastrointestinal neuroendocrine tumors: pancreatic endocrine tumors. Gastroenterology. 2008;135(5):1469–1492.
- 7. Poitras P, Gingras MH, Rehfeld JF. Secretin stimulation test for Zollinger-Ellison syndrome. Clin Biochem. 2020;84:8–14.
- 8. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander health performance framework 2020 summary report. Canberra: AIHW; 2020.
- 9. Sadowski SM, Millo C, Cottle-Delannes C, et al. 68Ga-DOTATATE PET/CT, 68Ga-DOTA-TOC PET/CT, and 18F-FDG PET/CT in the localization of Zollinger-Ellison syndrome. J Nucl Med. 2019;60(1):45–50.
- 10. Norton JA, Fraker DL, Alexander HR, et al. Surgery increases cure rates in patients with Zollinger-Ellison syndrome. Ann Surg. 2000;231(2):191–198.
- 11. Singh S, Asa SL, Dey C, et al. Diagnosis and management of gastrointestinal neuroendocrine tumors: an evidence-based Canadian consensus. Cancer Treat Rev. 2016;47:32–45.
- 12. Pharmaceutical Benefits Scheme (PBS). PBS Schedule. Australian Government Department of Health. Available at: https://www.pbs.gov.au. Accessed 2024.