📋 Key Information Summary
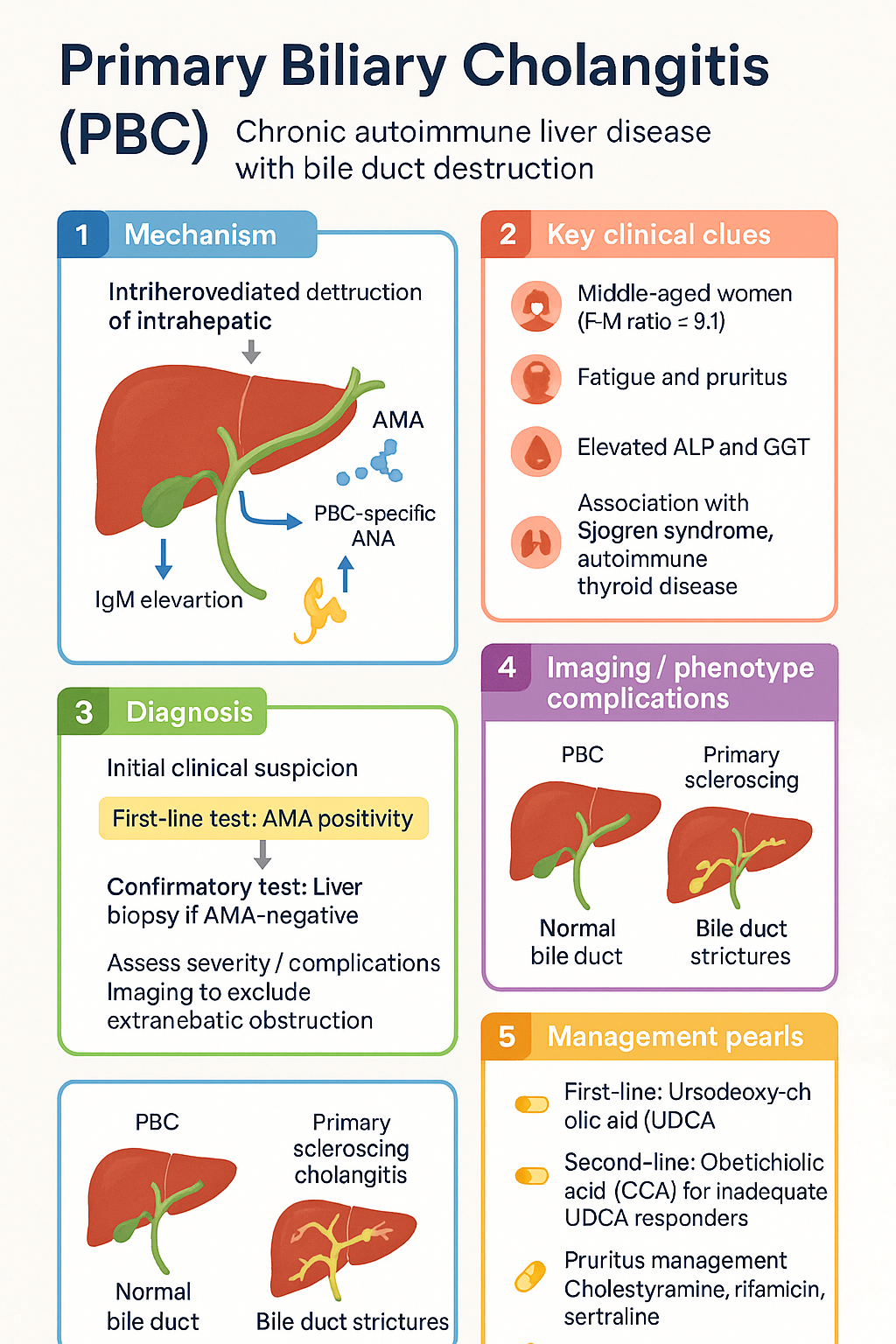
- Primary biliary cholangitis (PBC) is a chronic, immune-mediated granulomatous destruction of intrahepatic bile ducts, predominantly affecting middle-aged women (F:M ratio ≈ 9:1).
- Diagnosis requires two of three criteria: antimitochondrial antibody (AMA) positivity (or PBC-specific ANA against sp100/gp210), cholestatic LFTs persisting >6 months, and histologically compatible liver biopsy.
- IgM elevation is a characteristic (though not diagnostic) laboratory feature. Imaging must exclude extrahepatic biliary obstruction before diagnosis.
- Liver biopsy is reserved for AMA-negative patients, those with PBC-specific ANA only, or when overlap syndromes (e.g., PBC-AIH) are suspected.
- First-line therapy is ursodeoxycholic acid (UDCA) at 13–15 mg/kg/day; biochemical response is assessed at 12 months using POISE, GLOBE, UK-PBC, or Paris II criteria.
- Inadequate UDCA responders should receive second-line obeticholic acid (OCA) 5–10 mg daily; OCA is contraindicated in decompensated cirrhosis or portal hypertension due to risk of hepatic decompensation.
- Bezafibrate 400 mg/day (off-label) can be added to UDCA in suboptimal responders, with evidence from the BEZURSO and POISE trials.
- Emerging agents — seladelpar (recently FDA-approved) and elafibranor — show promise as add-on therapies for inadequate UDCA responders.
- Pruritus management follows a stepwise approach: cholestyramine (1st-line), rifampicin (2nd-line with LFT monitoring), sertraline, then naltrexone; refractory cases may require plasmapheresis or transplant.
- Fatigue has no proven pharmacotherapy; address modifiable contributors (depression, hypothyroidism, anaemia, sleep disorders).
- Osteoporosis screening with DEXA at diagnosis and every 2 years; fat-soluble vitamin (A, D, E, K) levels should be monitored, especially in advanced disease.
- Hepatocellular carcinoma (HCC) surveillance with 6-monthly ultrasound is indicated in patients with PBC-related cirrhosis.
- Liver transplantation is indicated for end-stage PBC (MELD ≥15 or decompensation); disease recurrence post-transplant occurs in 10–30% of patients.
- Aboriginal and Torres Strait Islander peoples may present later with more advanced disease; culturally safe, multidisciplinary care improves outcomes.
Introduction & Australian Epidemiology
Primary biliary cholangitis (PBC) — previously termed primary biliary cirrhosis — is a chronic, autoimmune cholestatic liver disease characterised by progressive, immune-mediated destruction of intrahepatic small bile ducts. The name was officially changed in 2015 to better reflect the disease spectrum, as many patients never develop cirrhosis.
PBC is the most common autoimmune liver disease in the developed world. Key epidemiological features include:
- Prevalence: Estimated at 15–40 per 100,000 in Australia, broadly consistent with international data (19–400 per 100,000 globally).
- Sex ratio: Female-to-male ratio approximately 9:1; approximately 90% of patients are female.
- Age: Median age at diagnosis is 50–55 years, though PBC can present at any age including in the paediatric population (rare).
- Trends: Incidence is increasing globally, partly due to improved detection of early/asymptomatic disease. Australian registry data suggest stable incidence over the past decade.
- Geographic variation: Higher prevalence in Northern European populations; prevalence in Aboriginal and Torres Strait Islander peoples is not well characterised but is likely under-recognised.
- Comorbidities: Strong association with other autoimmune conditions — Sjögren syndrome (up to 75%), autoimmune thyroid disease, Raynaud phenomenon, coeliac disease, and scleroderma/CREST syndrome.
Diagnosis
The diagnosis of PBC is made when a patient fulfils two of three criteria in the absence of other causes of cholestasis:
Investigations
Diagnostic Approach in AMA-Negative Patients
Approximately 5–10% of PBC patients are AMA-negative. In these cases:
- Check PBC-specific ANA (anti-sp100 and anti-gp210).
- Perform liver biopsy — look for florid duct lesions, granulomatous cholangitis, or bile duct paucity.
- Consider MRCP to exclude small-duct primary sclerosing cholangitis (PSC).
- AMA-negative PBC responds to UDCA similarly to AMA-positive disease; treat accordingly.
Overlap Syndromes
PBC can coexist with autoimmune hepatitis (PBC-AIH overlap syndrome), occurring in approximately 10% of patients. Suspicion arises when:
- ALP <2× ULN but ALT >5× ULN.
- IgG >2× ULN.
- Biopsy shows significant interface hepatitis alongside bile duct lesions.
Paris criteria and IAIHG scoring systems assist in identifying overlap. Management typically combines UDCA with immunosuppressive therapy (prednisolone ± azathioprine) under hepatologist supervision.
Treatment
First-Line: Ursodeoxycholic Acid (UDCA)
Response Assessment at 12 Months
Biochemical response to UDCA is assessed after 12 months of therapy. Multiple validated criteria exist; the choice depends on clinical context:
| Criterion | Definition of Adequate Response | Comment |
|---|---|---|
| Paris II | ALP and AST ≤1.5× ULN, and bilirubin ≤1 mg/dL (17 µmol/L) | Widely used in Australian practice; validated long-term prognostic prediction. |
| POISE criteria | ALP <1.67× ULN AND ≤15% reduction from baseline, OR total bilirubin ≤ ULN | Used in the POISE trial of OCA; gaining traction in Australasia. |
| GLOBE score | Score <0.30 for patients <65 years; <0.45 for patients ≥65 years | Online calculator available. Incorporates age, ALP, bilirubin, albumin, platelets. |
| UK-PBC score | Estimated 5-year risk of liver transplant or death <10% | Incorporates ALP, transaminases, bilirubin, albumin, platelets. Online calculator. |
Interpretation: Patients achieving an adequate biochemical response have a normalised life expectancy and do not require escalation. Those with an inadequate response (persistent ALP >1.67× ULN and/or elevated bilirubin) should be considered for second-line therapy.
Second-Line Therapy: Obeticholic Acid (OCA)
Off-Label Add-On: Bezafibrate
Emerging Agents
Several novel therapies are in late-stage development or recently approved:
| Agent | Mechanism | Status | Key Evidence |
|---|---|---|---|
| Seladelpar | Selective PPAR-δ agonist | FDA-approved (Aug 2024). Not yet PBS-listed in Australia. | ENHANCE trial: 61.7% achieved composite response at 12 months vs 20% placebo. Significant ALP reduction and pruritus improvement. |
| Elafibranor | Dual PPAR-α/δ agonist | FDA-approved (Jun 2024). Not yet PBS-listed in Australia. | ELATIVE trial: 51% composite response at 12 months vs 4% placebo. Robust ALP reduction. |
Symptom & Complication Management
Pruritus (Itch)
Pruritus affects approximately 20–70% of PBC patients at some point during the disease. It can be debilitating and significantly impairs quality of life. Management follows a stepwise approach:
Refractory pruritus: For patients unresponsive to the above, consider plasmapheresis, UV-B phototherapy, or referral for liver transplant assessment (pruritus is a valid transplant indication). Emerging data for maralixibat (IBAT inhibitor) in cholestatic pruritus.
Fatigue
Fatigue is the most prevalent symptom of PBC (affecting 50–80% of patients) and is often disproportionate to disease severity. Unfortunately, no pharmacological agent has proven effective.
- Modifiable contributors: Screen and treat depression (PHQ-9), hypothyroidism (TFTs), anaemia, obstructive sleep apnoea, coeliac disease, and medication side effects.
- Non-pharmacological: Graded exercise programmes, cognitive behavioural therapy, sleep hygiene counselling. Referral to allied health (exercise physiologist, psychologist).
- Patient support: PBC Foundation Australia and patient education resources improve coping and self-management.
Osteoporosis Screening & Management
Metabolic bone disease is common in PBC due to cholestasis-induced vitamin D malabsorption, reduced osteoblast activity, and chronic inflammation.
- DEXA scan at diagnosis (MBS item 12320).
- Repeat every 2 years.
- More frequent if postmenopausal, corticosteroid use, or advanced fibrosis.
- Calcium 1,000–1,200 mg/day + vitamin D 800–1,000 IU/day supplementation.
- Bisphosphonates (alendronate, risedronate) for T-score ≤ −2.5 or FRAX-indicated. Avoid IV bisphosphonates if oesophageal varices (risk of oesophagitis).
- Teriparatide or denosumab for refractory osteoporosis under specialist guidance.
Fat-Soluble Vitamin Deficiencies
Bile duct destruction in PBC impairs fat-soluble vitamin absorption (A, D, E, K). Deficiencies are more common with serum bilirubin >2× ULN or advanced fibrosis.
| Vitamin | Deficiency Signs | Replacement |
|---|---|---|
| Vitamin D | Osteomalacia, osteoporosis, fractures | Cholecalciferol 2,000–10,000 IU/day (titrate to 25-OH-D >75 nmol/L). May require higher doses in malabsorption. |
| Vitamin A | Night blindness, xerophthalmia | Retinol palmitate 25,000–50,000 IU/day PO; monitor levels to avoid toxicity. |
| Vitamin E | Ataxia, peripheral neuropathy (rare) | Alpha-tocopherol 400–800 IU/day PO if deficient. |
| Vitamin K | Coagulopathy (elevated INR) | Phytomenadione (vitamin K1) 10 mg IV/IM if INR prolonged. Maintenance with oral 10 mg weekly or as directed by INR. |
Hepatocellular Carcinoma (HCC) Surveillance
PBC-related cirrhosis carries a significant risk of HCC (annual incidence ~1–2%). Surveillance is mandatory:
- Who: All PBC patients with established cirrhosis (biopsy-proven or clinical/imaging evidence).
- How: 6-monthly abdominal ultrasound ± alpha-fetoprotein (AFP). MBS item 55030.
- HCC risk in PBC: Higher in male patients, those with advanced fibrosis (stage 4), and concurrent hepatitis C or metabolic risk factors.
Liver Transplantation
Liver transplantation is the definitive treatment for end-stage PBC and is associated with excellent outcomes (5-year survival >85%).
- Indications: MELD score ≥15, decompensation events (ascites, variceal bleeding, hepatic encephalopathy), HCC meeting Milan criteria, or intractable pruritus.
- Recurrence: PBC recurs in 10–30% of transplant recipients, typically 3–7 years post-transplant. Histological recurrence may occur before biochemical changes. UDCA is generally continued post-transplant.
- Referral: Refer to a liver transplant centre (Royal Prince Alfred Sydney, Austin Melbourne, Princess Alexandra Brisbane, Sir Charles Gairdner Perth, Flinders Adelaide) when MELD approaches 12–15 or at first decompensation event.
- Living donor transplant: Available at select Australian centres; discuss with transplant hepatologist.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Lindor KD, Bowlus CL, Boyer J, Levy C, Mayo M. Primary biliary cholangitis: 2018 practice guidance from the American Association for the Study of Liver Diseases. Hepatology. 2019;69(1):394-419.
- 2. European Association for the Study of the Liver. EASL Clinical Practice Guidelines: The diagnosis and management of patients with primary biliary cholangitis. J Hepatol. 2017;67(1):145-172.
- 3. Nevens F, Andreone P, Mazzella G, et al. A placebo-controlled trial of obeticholic acid in primary biliary cholangitis. N Engl J Med. 2016;375(7):631-643.
- 4. Corpechot C, Chazouillères O, Rousseau A, et al. A placebo-controlled trial of bezafibrate in primary biliary cholangitis. N Engl J Med. 2018;378(23):2171-2181.
- 5. Lammers WJ, van Buuren HR, Hirschfield GM, et al. Levels of alkaline phosphatase and bilirubin are surrogate end points of outcomes of patients with primary biliary cholangitis: an international follow-up study. Gastroenterology. 2014;147(6):1338-1349.
- 6. Carbone M, Mells GF, Pells G, et al. Sex and age are determinants of the clinical phenotype of primary biliary cirrhosis and response to ursodeoxycholic acid. Gastroenterology. 2013;144(3):560-569.
- 7. Bowlus CL, Galoosian RJ, Feld JJ, et al. Seladelpar efficacy and safety at 3 months in patients with primary biliary cholangitis: ENHANCE, a phase 3, randomized, placebo-controlled study. Hepatology. 2023;78(2):397-415.
- 8. Kowdley KV, Bowlus CL, Levy C, et al. Efficacy and safety of elafibranor in primary biliary cholangitis. N Engl J Med. 2024;390(9):795-805.
- 9. Carey EJ, Ali AH, Lindor KD. Primary biliary cirrhosis. Lancet. 2015;386(10003):1565-1575.
- 10. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.
- 11. Australian Indigenous HealthInfoNet. Overview of Aboriginal and Torres Strait Islander health status 2023. Perth: Edith Cowan University; 2023.
- 12. Corpechot C, Abenavoli L, Rabahi N, et al. Biochemical response to ursodeoxycholic acid and long-term prognosis in primary biliary cirrhosis. Hepatology. 2008;48(3):871-877.
- 13. Mayo MJ. Primary biliary cholangitis: narrowing the therapeutic gap. Hepatology. 2021;73(Suppl 1):40-50.
- 14. Services Australia. Pharmaceutical Benefits Schedule — Obeticholic acid. Canberra: Commonwealth of Australia; 2024. Available from: www.pbs.gov.au
- 15. Hirschfield GM, Dyson JK, Alexander GJM, et al. The British Society of Gastroenterology/UK-PBC primary biliary cholangitis treatment and management guidelines. Gut. 2018;67(9):1568-1594.