📋 Key Information Summary
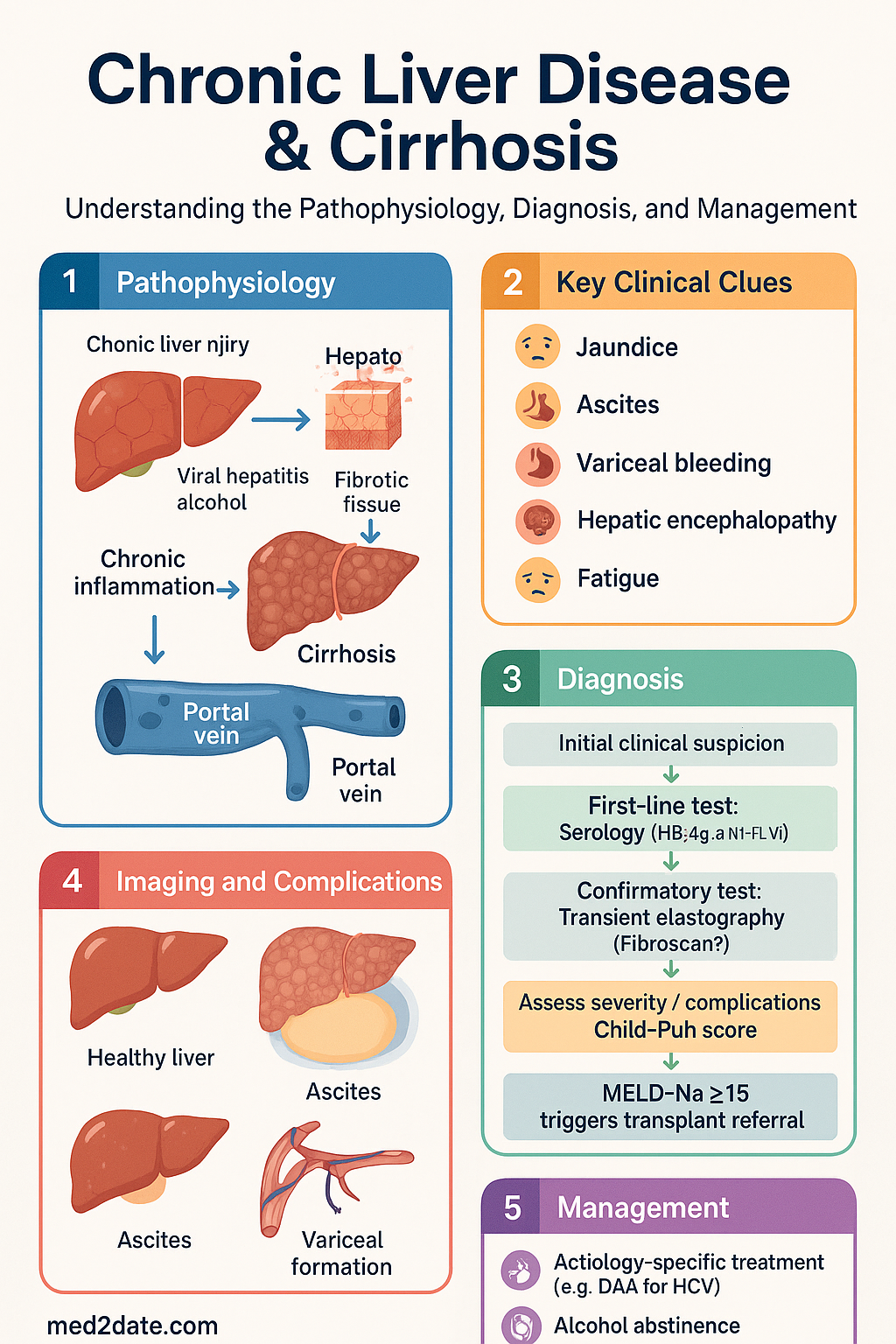
- Chronic liver disease (CLD) affects ~500 000 Australians; cirrhosis — the final common pathway — involves progressive fibrosis, hepatocyte dysfunction and portal hypertension.
- Aetiological workup is mandatory: serology (HBsAg, anti-HCV, HIV), autoimmune markers (ANA, ASMA, IgG for AIH; anti-mitochondrial Ab for PBC), metabolic screen (ferritin + transferrin saturation for HH; caeruloplasmin for Wilson; A1AT level and phenotype), and alcohol use assessment (AUDIT-C).
- Severity staging uses Child-Pugh score (A/B/C) and MELD-Na score; transient elastography (FibroScan®) quantifies fibrosis non-invasively; liver biopsy reserved for uncertain aetiology or dual pathology.
- Compensated cirrhosis carries 10-year survival >50%; decompensation (ascites, variceal bleeding, hepatic encephalopathy, jaundice) marks a sharp prognostic decline with ~50% 2-year mortality without transplant.
- Aetiology-specific treatment can reverse or halt progression: HCV SVR with DAA, sustained alcohol abstinence, HBV nucleos(t)ide suppression, and ≥7–10% weight loss in MASLD can lead to fibrosis regression and recompensation.
- HCC surveillance — 6-monthly abdominal ultrasound ± AFP in all cirrhotics (eligible for treatment).
- Variceal screening endoscopy at cirrhosis diagnosis; can defer if Baveno VII criteria met (LSM <20 kPa and platelets >150 × 10⁹/L).
- Primary variceal prophylaxis: carvedilol 6.25–12.5 mg daily preferred (non-selective β-blocker with α₁-antagonism); endoscopic band ligation (EBL) if NSBB intolerant.
- Acute variceal bleeding: resuscitate, IV terlipressin 2 mg then 1 mg q4h or octreotide 50 μg bolus then 250 μg/h infusion, IV ceftriaxone 1 g daily, early EBL within 12 hours; pre-emptive TIPS for Child-Pugh C 10–13 or B with active bleeding.
- Ascites management: sodium restriction <80 mmol/day, spironolactone ± furosemide, large-volume paracentesis with albumin replacement (8 g/L removed >5 L), TIPS for refractory ascites.
- Hepatic encephalopathy: precipitant identification (infection, GI bleed, constipation, dehydration, electrolytes), lactulose 15–30 mL titrated to 2–3 bowel motions/day; rifaximin 550 mg BD as add-on.
- Vaccinations — HAV, HBV (if non-immune), influenza annually, pneumococcal (PCV20 or PCV13 then PPSV23); bone density and nutritional assessment (sarcopenia, late-evening snack) are essential.
- ATSI populations experience higher CLD prevalence and mortality; remote access limitations, delayed diagnosis, and high HBV/HCV prevalence require targeted screening and culturally safe care.
🎧 Audio Brief
Aetiology & Assessment
Aetiological Workup
A systematic aetiological workup is essential because targeted treatment can halt or reverse fibrosis. Cirrhosis remains "cryptogenic" in ~5% of cases after thorough testing; dual pathology (e.g., AUD + MASLD) is increasingly recognised.
| Category | Investigations | Key Points |
|---|---|---|
| Viral | HBsAg, anti-HBc (IgG), anti-HBs; anti-HCV (reflex HCV RNA if positive); HIV | HCV cure with DAA eliminates risk; chronic HBV requires nucleos(t)ide suppression (entecavir or tenofovir) |
| Alcohol | AUDIT-C questionnaire; GGT, MCV, CDT; collateral history; FibroScan® | AUDIT-C ≥5 in men (≥4 in women) suggests hazardous use; sustained abstinence is the single most impactful intervention |
| MASLD / MASH | Fasting glucose/HbA1c, lipid profile, BMI/waist circumference, FIB-4 index, NFS; exclude other causes; MRI-PDFF or MRE if available | Previously NAFLD/NASH; ≥7–10% body weight loss associated with MASH resolution and fibrosis improvement; resmetirom (THRβ agonist) recently TGA-approved for MASH with F2–F3 fibrosis |
| Autoimmune | ANA, anti-smooth muscle Ab (ASMA), IgG (AIH); anti-mitochondrial Ab (AMA), IgM (PBC); MRCP (PSC); atypical pANCA | AIH: predniso(lo)ne + azathioprine; PBC: ursodeoxycholic acid 13–15 mg/kg/day; PSC: no proven therapy — ursodiol for cholestasis symptoms; pruritus: cholestyramine, rifampicin |
| Metabolic | Ferritin + transferrin saturation (HH); caeruloplasmin + serum copper (Wilson); α₁-antitrypsin level + phenotype (A1AT deficiency) | HH: therapeutic venesection if TSAT >45%; Wilson: penicillamine or trientine + zinc; A1AT: no specific Rx — transplant if decompensated |
| Drug-induced | Medication review (amiodarone, methotrexate, nitrofurantoin, minocycline, isoniazid, herbal/dietary supplements); RUCAM scoring | Withdrawal of offending agent; histological pattern helps (hepatitic vs cholestatic vs steatotic) |
Severity Scoring
Two complementary scores are used: Child-Pugh for clinical classification and MELD-Na for transplant listing and prognostication.
Child-Pugh Score
| Parameter | 1 point | 2 points | 3 points |
|---|---|---|---|
| Bilirubin (μmol/L) | <34 | 34–50 | >50 |
| Albumin (g/L) | >35 | 28–35 | <28 |
| INR | <1.7 | 1.7–2.3 | >2.3 |
| Ascites | None | Mild | Moderate–severe |
| Hepatic encephalopathy | None | Grade I–II | Grade III–IV |
MELD-Na Score
MELD-Na incorporates serum bilirubin, INR, creatinine and sodium to predict 90-day mortality. Used for transplant prioritisation in Australia. Scores 6–40 (capped at 40); MELD-Na ≥15 generally triggers transplant workup referral.
Non-Invasive Fibrosis Assessment
Transient elastography (FibroScan®) is widely available in metropolitan and many regional centres (MBS item 12205 — FibroScan, FibroTouch or equivalent). Cutoffs vary by aetiology:
| Aetiology | F2 (significant fibrosis) | F3 (advanced fibrosis) | F4 (cirrhosis) |
|---|---|---|---|
| MASLD | ≥8.0 kPa | ≥10.0 kPa | ≥13.6 kPa |
| Viral hepatitis | ≥7.0 kPa | ≥9.5 kPa | ≥12.5 kPa |
| Alcohol-related | ≥7.0 kPa | ≥9.5 kPa | ≥12.5 kPa |
FIB-4 index and NFS are useful first-line triage tools in primary care to exclude advanced fibrosis (high negative predictive value). Liver biopsy is reserved for: (1) uncertain aetiology after non-invasive testing, (2) suspected dual pathology, and (3) pre-transplant assessment where histological diagnosis changes management.
Compensated vs Decompensated Cirrhosis
The transition from compensated to decompensated cirrhosis is the defining prognostic event in chronic liver disease. Understanding this transition and the potential for recompensation is central to modern management.
Natural History
Decompensation Events
Aetiology-Specific Reversal & Recompensation
Sustained abstinence from alcohol (≥6 months) in alcohol-related liver disease improves histology in up to 50% of patients and is associated with recompensation. Relapse rates are high; integrated addiction medicine support is essential. Consider naltrexone (avoid in active liver disease) or acamprosate.
≥7–10% total body weight loss is associated with MASH resolution and fibrosis improvement by ≥1 stage. Caloric deficit 500–750 kcal/day, Mediterranean-style diet, supervised exercise. Bariatric surgery (Roux-en-Y) may be considered in selected patients. GLP-1 receptor agonists (liraglutide, semaglutide) show promise but are not yet PBS-listed for MASLD.
Surveillance & Routine Care
HCC Surveillance
All patients with cirrhosis who are potential candidates for treatment should undergo HCC surveillance, as early detection (BCLC stage 0/A) enables curative therapy (resection, ablation, transplant).
Key principles for GP and specialist practice:
- Surveillance should commence at cirrhosis diagnosis and continue for the patient's lifetime if they remain a treatment candidate.
- Surveillance reduces HCC-related mortality by 37% (RR 0.63; Cochrane meta-analysis).
- Non-cirrhotic chronic HBV carriers also require surveillance (age-specific risk stratification per AASLD/APASL guidelines).
- MASLD-related cirrhosis: HCC risk is present even without advanced fibrosis in some series; surveil those with F3–F4 fibrosis.
Variceal Screening Endoscopy
All patients with cirrhosis should be screened for oesophageal varices at diagnosis. The Baveno VII consensus (2022) refined the criteria for safe deferral:
Bone Density
Osteoporosis is prevalent in cirrhosis (12–55%) due to vitamin D deficiency, hypogonadism, chronic inflammation and cholestasis (particularly PBC/PSC). DEXA scan at diagnosis; repeat every 2 years if abnormal. Treat with calcium + vitamin D supplementation; bisphosphonates (alendronate) are safe in cirrhosis if no oesophageal varices (or varices are treated). Denosumab is an alternative but monitor calcium closely.
Nutritional Assessment
Malnutrition affects 50–90% of patients with cirrhosis and is an independent predictor of mortality. Key interventions:
- Sarcopenia screening: CT-measured skeletal muscle index (L3 level) or clinical tools (SARC-F, mid-arm muscle circumference). Physical activity and resistance training recommended.
- Caloric targets: 35 kcal/kg/day; protein 1.2–1.5 g/kg/day (do NOT restrict protein in hepatic encephalopathy unless Grade IV).
- Late-evening snack: A complex-carbohydrate snack before bed reduces overnight catabolism and improves nitrogen balance — strongly recommended in all cirrhotics.
- Vitamin and mineral supplementation: Vitamin D (1000–4000 IU/day), zinc (220 mg zinc sulphate daily if deficient), fat-soluble vitamin replacement (A, D, E, K) in cholestatic disease.
Vaccinations
| Vaccine | Schedule | Notes |
|---|---|---|
| Hepatitis A | 2 doses (0 and 6 months) | If non-immune (anti-HAV negative); check anti-HAV IgG first |
| Hepatitis B | Standard 3-dose schedule or accelerated 4-dose (0, 7, 21 days + 12 months) | Anti-HBs >10 IU/L = immune; higher doses (40 μg HBvaxPRO) may be needed in cirrhosis due to impaired immunogenicity |
| Influenza | Annual | NIP-funded; quadrivalent formulation preferred |
| Pneumococcal | PCV20 single dose, or PCV13 then PPSV23 (≥8 weeks later) | Pneumococcal disease risk increased in cirrhosis; NIP-funded under ATAGI recommendations |
| COVID-19 | Per current ATAGI schedule | Cirrhosis listed as immunocompromised condition for additional doses |
Variceal Management
Primary Prophylaxis
Primary prophylaxis aims to prevent the first variceal bleed. Indicated when medium/large varices are found on screening endoscopy, or when small varices have red signs or occur in Child-Pugh C patients.
First-Line: Non-Selective Beta-Blockers (NSBB)
Acute Variceal Bleeding
Acute variceal haemorrhage is a medical emergency with 6-week mortality of 15–20%. A coordinated approach involving emergency medicine, gastroenterology, interventional radiology and critical care is essential.
Vasoactive Drugs
Rescue Therapies
- Balloon tamponade (Sengstaken–Blakemore or Minnesota tube): temporary bridge (≤24 hr) for uncontrolled bleeding; inflate gastric balloon; requires ICU and intubation; risk of aspiration, oesophageal necrosis.
- Self-expandable metal stent (Danis stent): alternative to balloon tamponade; better tolerated, can remain 7–14 days.
- Pre-emptive TIPS (transjugular intrahepatic portosystemic shunt): within 72 hr for high-risk patients — Child-Pugh B with active bleeding at endoscopy, or Child-Pugh C 10–13. Reduces treatment failure and mortality in this subgroup (Villanueva, NEJM 2010; García-Pagán, Lancet 2013).
Secondary Prophylaxis
After the first variceal bleed, the risk of rebleeding is ~60% within 1 year. Secondary prophylaxis (combination therapy) reduces rebleeding to ~20%.
Aboriginal and Torres Strait Islander Health Considerations
Chronic liver disease is the 8th leading cause of death among Aboriginal and Torres Strait Islander peoples, with rates 3.5 times higher than the non-Indigenous population. Cirrhosis mortality has risen over the past two decades despite overall improvements in other chronic diseases. Culturally safe, community-driven approaches are essential.
📚 References
- 1. de Franchis R, Bosch J, Garcia-Tsao G, et al. Baveno VII — Renewing consensus in portal hypertension. J Hepatol. 2022;76(4):959–974.
- 2. Villanueva C, Colomo A, Bosch A, et al. Transfusion strategies for acute upper gastrointestinal bleeding. N Engl J Med. 2013;368(1):11–21.
- 3. García-Pagán JC, Caca K, Bureau C, et al. Early use of TIPS in patients with cirrhosis and variceal bleeding. N Engl J Med. 2010;362(25):2370–2379.
- 4. European Association for the Study of the Liver. EASL Clinical Practice Guidelines on the management of hepatic encephalopathy. J Hepatol. 2022;77(3):807–824.
- 5. Rinella ME, Neuschwander-Tetri BA, Siddiqui MS, et al. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology. 2023;77(5):1797–1835.
- 6. Fernández J, Tandon P, Hernandez-Gea V, et al. Non-selective beta-blockers in cirrhosis: current evidence and future directions. Lancet Gastroenterol Hepatol. 2021;6(3):230–241.
- 7. Australian Institute of Health and Welfare. Chronic liver disease and cirrhosis in Aboriginal and Torres Strait Islander peoples. Cat. no. IHW 249. Canberra: AIHW; 2022.
- 8. Davis JS, Turnidge J, Blyth CC, et al. Consensus guidelines for the management of bacterial infections in patients with chronic liver disease. Intern Med J. 2020;50(12):1448–1465.
- 9. Ge PS, Runyon BA. Treatment of patients with cirrhosis. N Engl J Med. 2016;375(8):767–777.
- 10. Tsochatzis EA, Bosch J, Burroughs AK. Liver cirrhosis. Lancet. 2014;383(9930):1749–1761.
- 11. Latt NL, Dutta MP, Tallis C, et al. Antiviral treatment for chronic hepatitis B virus in Aboriginal and Torres Strait Islander peoples: a systematic review. Aust N Z J Public Health. 2021;45(3):273–278.
- 12. Morgan TR. The impact of alcohol consumption on chronic liver disease. Hepatology. 2023;77(6):2109–2119.