📋 Key Information Summary
- Chronic diarrhoea is defined as loose, frequent stools persisting for >4 weeks; acute diarrhoea (<4 weeks) is managed differently and most commonly infectious or medication-related.
- Initial workup should include a thorough medication review (metformin, PPIs, SSRIs, NSAIDs, colchicine, antibiotics), travel history, dietary history (FODMAPs, lactose, artificial sweeteners), and baseline bloods (FBC, EUC, LFT, CRP, TFT, coeliac serology).
- Stool testing strategy is guided by clinical context: stool microscopy, culture and sensitivity for suspected infectious aetiology; C. difficile toxin PCR if recent antibiotics or healthcare exposure; faecal calprotectin to differentiate inflammatory from functional causes.
- Faecal elastase-1 (<200 µg/g) and 72-hour faecal fat (>7 g/day) are first-line tests for pancreatic exocrine insufficiency and fat malabsorption respectively.
- Coeliac disease screening requires total serum IgA plus tissue transglutaminase IgA (tTG-IgA); if IgA-deficient, order deamidated gliadin peptide (DGP) IgG; patients must be on a gluten-containing diet at testing.
- Hyperthyroidism is an under-recognised cause of chronic diarrhoea — always check TSH; bile acid diarrhoea (BAD) is increasingly recognised and diagnosed via SeHCAT scan or empirical bile acid sequestrant trial.
- Referral to gastroenterology is indicated for persistent unexplained diarrhoea, raised inflammatory markers (CRP/ESR), unintentional weight loss, nocturnal symptoms, rectal bleeding, or suspected organic disease.
- Red-flag features — age >50 at new symptom onset, nocturnal diarrhoea waking the patient, weight loss >5%, blood/mucus in stool, family history of colorectal cancer or IBD — warrant urgent colonoscopy.
- In Australia, Aboriginal and Torres Strait Islander peoples have higher rates of infectious gastroenteritis, chronic H. pylori, and environmental enteropathy; early investigation and culturally safe communication are essential.
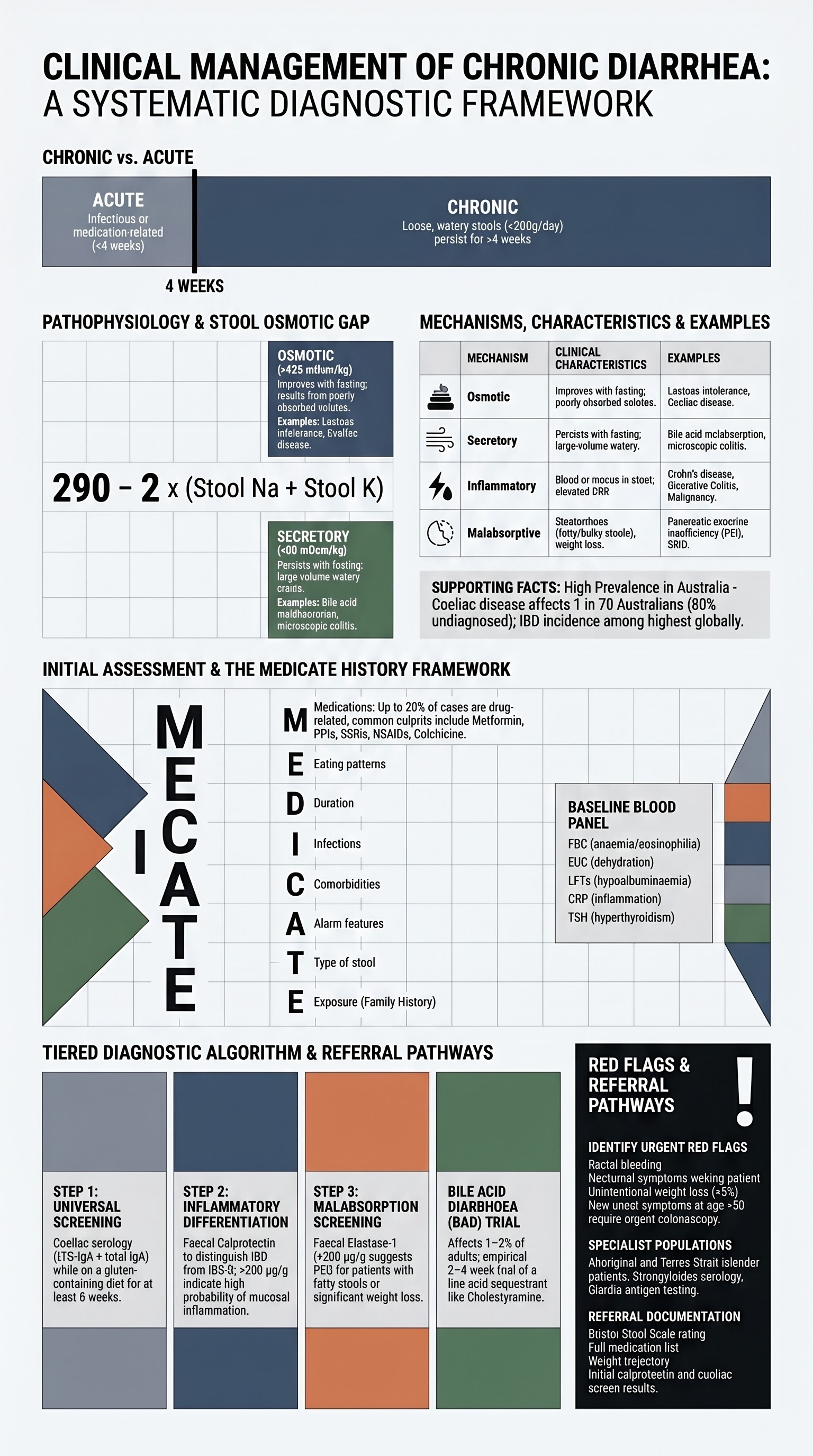
- Osmotic diarrhoea is suggested by stool osmotic gap >125 mOsm/kg; secretory diarrhoea has a gap <50 mOsm/kg — this distinction guides further workup.
- Iron deficiency anaemia, folate deficiency, vitamin D deficiency, and hypoalbuminaemia may accompany chronic diarrhoea and should prompt investigation for malabsorption.
- Irritable bowel syndrome (IBS-D) is a diagnosis of exclusion after organic causes have been ruled out; Rome IV criteria should be applied.
Introduction & Australian Epidemiology
Chronic diarrhoea — defined as the passage of loose or watery stools at least three times daily, or an increase in stool weight to >200 g/day, persisting beyond four weeks — is one of the most common presentations in Australian primary care. It affects approximately 5–7% of the adult population at any given time and accounts for a significant burden of specialist gastroenterology referrals nationwide.
The differential diagnosis is broad, spanning functional disorders (predominantly irritable bowel syndrome with diarrhoea, IBS-D), inflammatory bowel disease (Crohn disease and ulcerative colitis), coeliac disease, chronic infections, pancreatic exocrine insufficiency, bile acid malabsorption, medication side effects, endocrine disorders, and less commonly, colorectal neoplasia.
In the Australian context, several epidemiological considerations are particularly relevant:
- Coeliac disease affects approximately 1 in 70 Australians, though only 1 in 5 are diagnosed, making it one of the most common chronic causes of diarrhoea that is frequently missed in primary care.
- Inflammatory bowel disease (IBD) incidence in Australia is among the highest globally, with over 85,000 affected individuals; peak incidence is in the 15–29 and 60–69 age groups.
- Clostridioides difficile infection (CDI) rates have risen in Australian hospitals and aged-care facilities, particularly with ribotype 027 and 014/020 strains.
- Aboriginal and Torres Strait Islander Australians experience disproportionately higher rates of gastrointestinal infections, environmental enteropathy, and H. pylori carriage, contributing to chronic diarrhoea in remote communities.
- Bile acid diarrhoea (BAD) is estimated to affect 1–2% of the adult population and is increasingly recognised as an underdiagnosed cause of chronic watery diarrhoea, particularly post-cholecystectomy.
Classification & Initial Workup
A systematic approach to chronic diarrhoea begins with distinguishing it from acute diarrhoea and then classifying the likely mechanism to guide targeted investigation.
Acute vs Chronic Diarrhoea
| Feature | Acute Diarrhoea (<4 weeks) | Chronic Diarrhoea (>4 weeks) |
|---|---|---|
| Duration | <4 weeks | >4 weeks |
| Common causes | Infections (viral, bacterial, parasitic), medication, food poisoning | IBS-D, IBD, coeliac disease, bile acid malabsorption, pancreatic insufficiency, chronic infections |
| Initial management | Supportive; stool MCS if fever, blood, or travel; C. difficile if recent antibiotics | Structured diagnostic workup with targeted investigations |
| Key red flags | Dehydration, bloody stool, fever >38.5°C, immunosuppression | Weight loss, nocturnal symptoms, rectal bleeding, age >50 new onset, family history CRC |
Mechanism-Based Classification
| Mechanism | Characteristics | Stool Osmotic Gap | Examples |
|---|---|---|---|
| Osmotic | Improves with fasting; related to ingestion of poorly absorbed solutes | >125 mOsm/kg | Lactose intolerance, sorbitol/mannitol, magnesium laxatives, coeliac disease |
| Secretory | Persists with fasting; large-volume watery stools | <50 mOsm/kg | Bile acid malabsorption, VIPoma, carcinoid, cholera, microscopic colitis |
| Inflammatory | Blood/mucus in stool; elevated CRP, faecal calprotectin | Variable | Crohn disease, ulcerative colitis, diverticulitis, colorectal cancer, radiation proctitis |
| Motility-related | Rapid transit; associated with systemic conditions or medications | Variable | IBS-D, hyperthyroidism, diabetic autonomic neuropathy, post-vagotomy |
| Malabsorptive | Steatorrhoea, weight loss, nutritional deficiencies | >125 mOsm/kg | Pancreatic exocrine insufficiency, coeliac disease, SIBO, short bowel syndrome |
Stool Osmotic Gap Calculation
Initial Workup — Baseline Investigations
Every patient presenting with chronic diarrhoea (>4 weeks) should receive the following baseline investigations at first assessment:
Essential History — The MEDICATE Mnemonic
- M — Medications (metformin, PPIs, SSRIs, NSAIDs, olmesartan, colchicine, acarbose)
- E — Eating patterns (FODMAPs, lactose, artificial sweeteners — sorbitol, mannitol, erythritol)
- D — Duration and pattern (nocturnal vs daytime, postprandial, fasting)
- I — Infections and travel history (Giardia, parasites, C. difficile)
- C — Comorbidities (diabetes, thyroid disease, coeliac disease, IBD, HIV)
- A — Alarm features (weight loss, blood, nocturnal symptoms, age >50)
- T — Type and consistency (watery, fatty/bulky, bloody, mucoid)
- E — Family history (IBD, coeliac disease, colorectal cancer, polyposis syndromes)
Stool Testing Strategy
Stool investigations in chronic diarrhoea should be guided by clinical context rather than ordered reflexively. The testing approach differs based on whether the presentation is subacute (4–12 weeks) with infectious features, or chronic (>12 weeks) with features suggestive of inflammatory, malabsorptive, or functional aetiology.
Stool Tests — Indications and Interpretation
| Investigation | Indication | Interpretation | Availability |
|---|---|---|---|
| Stool microscopy, culture & sensitivity (MCS) | Recent travel, acute-on-chronic flare, fever, blood/mucus, immunosuppression | Identifies bacterial pathogens (Salmonella, Shigella, Campylobacter, Yersinia); request specific parasites if travel to endemic area | All Australian pathology labs; MBS Item 69310 |
| C. difficile toxin PCR / GDH + toxin EIA | Recent antibiotics (within 3 months), PPI use, healthcare/hospital contact, aged-care residence | PCR alone is highly sensitive but may detect colonisation; GDH screen + toxin EIA two-step algorithm preferred. Positive toxin = treat. | Available at all major labs; MBS Item 69322 |
| Faecal calprotectin | Suspected IBD vs IBS-D differentiation; elevated CRP; family history of IBD | <50 µg/g = low probability of IBD (NPV >95%); 50–200 = indeterminate (repeat in 4–6 weeks); >200 = high probability — refer to GI for colonoscopy | Major Australian labs (Sonic, DHM, QML, PathWest WA); MBS Item 69320 |
| Faecal elastase-1 | Suspected pancreatic exocrine insufficiency (PEI): steatorrhoea, weight loss, chronic alcohol use, pancreatic disease history | <200 µg/g = moderate PEI; <100 µg/g = severe PEI. Requires formed stool sample (avoid watery stool — falsely low). Does not require fasting. | Reference labs; MBS Item 69334 |
| 72-hour faecal fat quantification | Suspected fat malabsorption / steatorrhoea when faecal elastase is equivocal | >7 g/day on standard diet (>14 g/day on high-fat diet) = steatorrhoea. Requires 72-hour collection — patient compliance is often a barrier. | Reference and hospital-based labs; MBS Item 69334 |
| Stool ova, cysts & parasites (OCP) | Travel to endemic areas (SE Asia, Pacific, Africa, Central America), immunosuppression, eosinophilia, MSM, daycare exposure | Giardia lamblia is the most common parasitic cause in Australia; request Giardia-specific antigen test for higher sensitivity; three samples on alternate days improve yield. | All Australian labs; MBS Item 69310 |
| Faecal immunochemical test (FIT) | Suspected colorectal neoplasia; not a primary test for chronic diarrhoea but may be incidental | Positive FIT in context of chronic diarrhoea warrants colonoscopy. Australia's National Bowel Cancer Screening Program uses FIT for population screening from age 50. | All Australian labs; MBS Item 69325 |
| Faecal lactoferrin | Alternative to calprotectin for detecting intestinal inflammation; may be used in conjunction | Elevated in IBD and bacterial gastroenteritis; negative in IBS and viral gastroenteritis. | Available at major labs; MBS Item 69320 |
Stepwise Stool Testing Algorithm
Rule-Out Coeliac Disease & Thyroid Disease
Coeliac disease and thyroid dysfunction are two highly prevalent, treatable causes of chronic diarrhoea that should be excluded in every patient presenting with symptoms lasting >4 weeks. Both conditions are frequently underdiagnosed in Australian practice.
Coeliac Disease — Screening Protocol
Coeliac disease affects approximately 1.4% of the Australian population (1 in 70), with a diagnosed prevalence of only 0.3–0.4%, suggesting significant underdiagnosis. All patients with chronic unexplained diarrhoea, bloating, weight loss, iron deficiency anaemia, or a first-degree relative with coeliac disease should be screened.
Serological Testing
Coeliac Disease — Interpretation Guide
| Result | Interpretation | Next Step |
|---|---|---|
| tTG-IgA elevated, IgA normal | Likely coeliac disease | GI referral for duodenal biopsy (do not start GFD yet) |
| tTG-IgA negative, IgA normal | Coeliac disease unlikely | Consider other diagnoses; retest if high clinical suspicion |
| tTG-IgA negative, IgA deficient | Result uninterpretable (IgA deficiency) | Order DGP-IgG; GI referral |
| tTG-IgA weakly positive (1–2× ULN) | Indeterminate — may be false positive | Confirm with DGP-IgG and/or endomysial antibodies (EMA); GI referral |
Thyroid Disease
Hyperthyroidism accelerates gut motility and can present with chronic diarrhoea, often preceding classical symptoms such as tremor, weight loss, heat intolerance, and palpitations. Hypothyroidism is more commonly associated with constipation but can occasionally cause alternating bowel habits.
Bile Acid Diarrhoea (BAD)
Bile acid diarrhoea (also termed bile acid malabsorption) is an increasingly recognised cause of chronic watery diarrhoea, affecting an estimated 1–2% of the Australian population. It is particularly common after cholecystectomy (up to 20% of post-cholecystectomy patients) and in patients with Crohn disease involving the terminal ileum.
| Classification | Description | Common Causes |
|---|---|---|
| Type 1 (Secondary) | Ileal dysfunction or resection causing impaired bile acid reabsorption | Crohn disease (terminal ileum), ileal resection, radiation enteritis |
| Type 2 (Primary / Idiopathic) | Excess bile acid production without identifiable cause | Idiopathic; may be associated with FGF19 deficiency |
| Type 3 (Associated) | Bile acid dysregulation secondary to other conditions | Post-cholecystectomy, coeliac disease, SIBO, PPI use, chronic pancreatitis |
Diagnosis and Treatment of BAD
- SeHCAT scan (selenium-homocholic acid taurine scan): gold standard; retention <10% at 7 days confirms BAD. Limited availability in Australia (major tertiary centres only).
- Serum 7α-hydroxy-4-cholesten-3-one (C4): elevated levels suggest excess bile acid synthesis; available at select reference laboratories.
- Empirical trial of bile acid sequestrant (cholestyramine 4 g once or twice daily for 2–4 weeks): a therapeutic response supports the diagnosis and is the most practical approach in Australian primary care where SeHCAT is unavailable.
When to Refer to Gastroenterology
Most patients with chronic diarrhoea can be effectively evaluated in primary care with a structured diagnostic approach. However, timely gastroenterology referral is essential when specific red-flag features are present or when initial workup is unrevealing.
Referral Indications
| Indication | Urgency | Action |
|---|---|---|
| Rectal bleeding / blood in stool | Urgent | Colonoscopy within 2 weeks; rule out CRC, IBD, angiodysplasia |
| Unintentional weight loss (>5% body weight in 6 months) | Urgent | Colonoscopy + CT abdomen/pelvis; investigate for malignancy, IBD, malabsorption |
| Nocturnal diarrhoea (waking from sleep) | Urgent | Suggests organic cause — IBD, microscopic colitis, bile acid malabsorption. Urgent colonoscopy with random biopsies. |
| Age >50 with new-onset change in bowel habit | Urgent | Colonoscopy within 30 days; rule out colorectal neoplasia |
| Family history of CRC or hereditary polyposis | Urgent | Colonoscopy per surveillance guidelines; consider genetic referral (Lynch syndrome, FAP) |
| Elevated faecal calprotectin (>200 µg/g) | Semi-urgent | Ileocolonoscopy with biopsies to confirm or exclude IBD |
| Elevated inflammatory markers (CRP, ESR) with diarrhoea | Semi-urgent | Investigation for IBD, infection, malignancy; GI consultation |
| Positive coeliac serology | Semi-urgent | Gastroscopy with duodenal biopsy for histological confirmation; dietitian referral |
| Persistent unexplained diarrhoea (>4 weeks, negative initial workup) | Routine | GI consultation for consideration of colonoscopy with random biopsies (microscopic colitis), SeHCAT scan, hydrogen breath test (SIBO), or endocrine evaluation |
| Suspected microscopic colitis | Routine | Colonoscopy with random colonic biopsies (mucosa appears macroscopically normal); typically affects women >60 years with watery non-bloody diarrhoea |
| Suspected pancreatic exocrine insufficiency | Routine | GI/HPB referral for faecal elastase, CT pancreas, EUS if indicated; initiation of PERT |
| Suspected bile acid diarrhoea — failed empirical cholestyramine | Routine | GI referral for SeHCAT scan (where available) or consideration of alternative bile acid sequestrants (colestipol, colesevelam) |
What to Include in the Referral
- Detailed symptom description: duration, frequency, stool consistency (Bristol Stool Scale), presence of blood/mucus, nocturnal vs daytime
- Complete medication list including OTC, supplements, and recent antibiotic use
- Results of all investigations: FBC, EUC, LFTs, CRP, coeliac serology, TFT, faecal calprotectin, stool MCS
- Body weight trajectory (baseline and current)
- Family history of IBD, CRC, coeliac disease, polyposis
- Travel history if relevant
- Previous colonoscopy or gastroscopy reports if available
Special Populations
Pregnancy
Paediatrics
Elderly
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Australians experience significantly higher rates of gastrointestinal disease, chronic diarrhoea, and associated complications compared with non-Indigenous Australians. Culturally safe, trauma-informed approaches are essential when assessing and managing chronic diarrhoea in this population.
📚 References
- 1. Schiller LR, Pardi DS, Spiller R, et al. Gastro 2013 APDW/WCOG Shanghai Working Party Report: chronic diarrhea — definition, classification, diagnosis. J Gastroenterol Hepatol. 2014;29(1):6-25.
- 2. Australian Institute of Health and Welfare (AIHW). Gastroenteritis in Aboriginal and Torres Strait Islander communities. AIHW; 2023.
- 3. Crohn's and Colitis Australia. The Economic Impact of Inflammatory Bowel Disease in Australia. Crohn's & Colitis Australia; 2022.
- 4. Singh P, Arora A, Strand TA, et al. Global prevalence of celiac disease: systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2018;16(6):823-836.e2.
- 5. National Health and Medical Research Council (NHMRC). Iron: National Health and Medical Research Council Nutrient Reference Values for Australia and New Zealand. Canberra: NHMRC; 2023.
- 6. Slattery SA, Niaz O, Aziz Q, Ford AC, Farmer AD. Systematic review with meta-analysis: the prevalence of bile acid malabsorption in the irritable bowel syndrome with diarrhoea. Aliment Pharmacol Ther. 2015;42(1):3-11.
- 7. Drossman DA, Hasler WL. Rome IV — Functional GI Disorders: Disorders of Gut-Brain Interaction. Gastroenterology. 2016;150(6):1257-1261.
- 8. Royal Australian College of General Practitioners (RACGP). Guidelines for preventive activities in general practice (Red Book). 9th ed. Melbourne: RACGP; 2018.
- 9. Sandborn WJ, Feagan BG, Wolf DC, et al. Ozanimod induction and maintenance in moderate-to-severe Crohn's disease. N Engl J Med. 2023;389(10):919-930.
- 10. RHDAustralia (RACP, ASID, CARPA). Strongyloides: Clinical Management Guidelines for Northern Territory Primary Health Care. Darwin: RHDAustralia; 2023.
- 11. Tibble JA, Sigthorsson G, Foster R, Forgacs I, Bjarnason I. Use of surrogate markers of inflammation and Rome criteria to distinguish organic from nonorganic intestinal disease. Gastroenterology. 2002;123(2):450-460.
- 12. Ford AC, Moayyedi P, Chey WD, et al. American College of Gastroenterology monograph on management of irritable bowel syndrome. Am J Gastroenterol. 2018;113(Suppl 2):1-18.
- 13. Masclee GM, Coloma PM, Kuipers EJ, Sturkenboom MC. Increased risk of microscopic colitis with use of proton pump inhibitors and non-steroidal anti-inflammatory drugs. Am J Gastroenterol. 2015;110(5):749-759.
- 14. Therapeutic Goods Administration (TGA). Australian Product Information — Cholestyramine (Questran Lite). Canberra: TGA; 2023.