📋 Key Information Summary
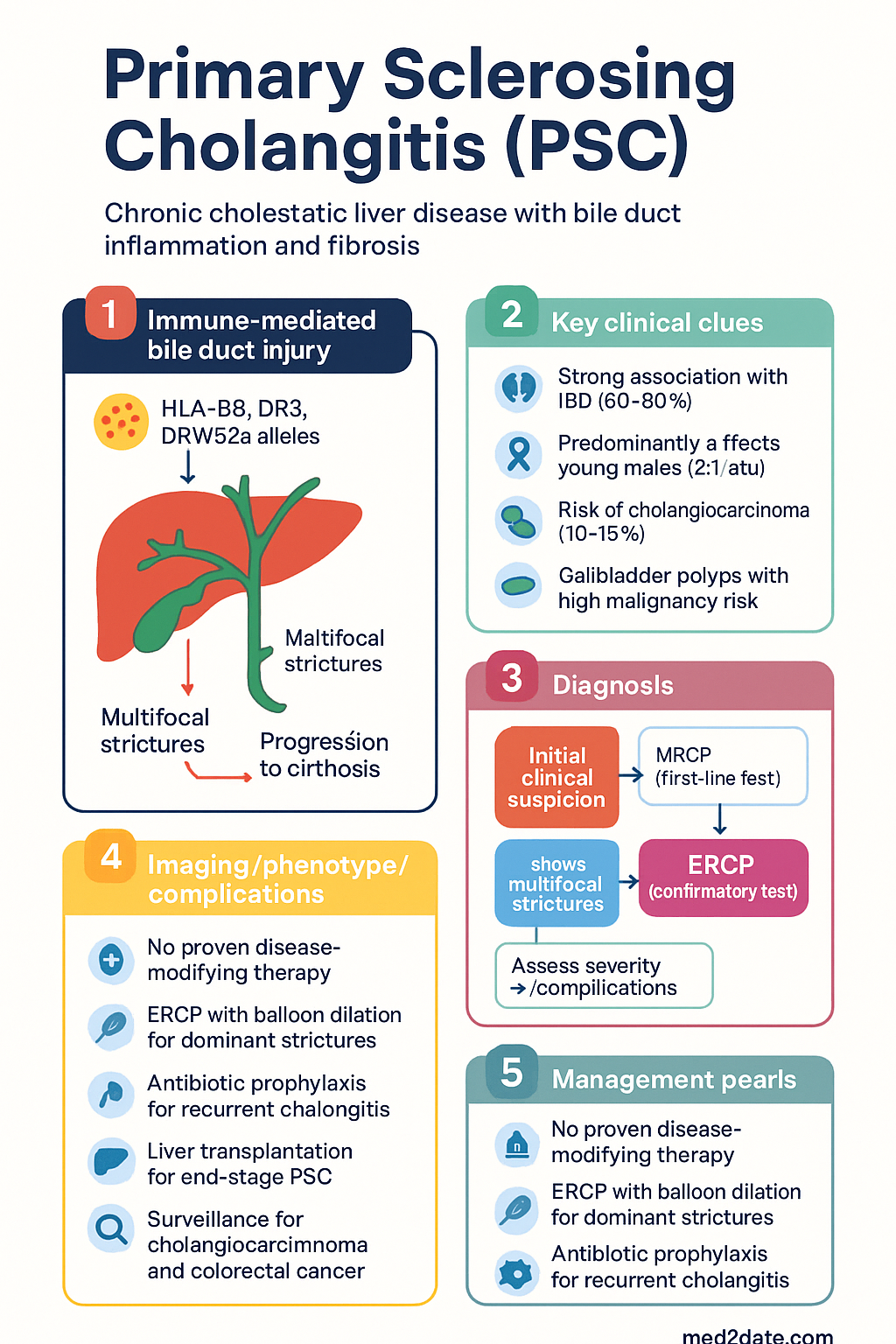
- Primary sclerosing cholangitis (PSC) is a chronic cholestatic liver disease characterised by inflammation and fibrosis of intrahepatic and/or extrahepatic bile ducts, progressing to cirrhosis in 50–60% of patients.
- Diagnosis requires MRCP or ERCP demonstrating multifocal strictures with beading; secondary causes (IgG4-related sclerosing cholangitis, ischaemic cholangiopathy, infections) must be excluded.
- Liver biopsy is not routinely required for diagnosis but may be useful in small-duct PSC or to assess parenchymal disease.
- Small-duct PSC (normal cholangiogram with histological periductal fibrosis) is a distinct variant with better prognosis; 12–20% progress to large-duct disease.
- Strong association with IBD — 60–80% of PSC patients have concomitant IBD (predominantly ulcerative colitis); colonoscopy is mandatory at PSC diagnosis for all patients.
- Cholangiocarcinoma (CCA) is the most feared complication (lifetime risk 10–15%); annual MRI/MRCP ± CA 19-9 is recommended for surveillance.
- Gallbladder polyps in PSC carry high malignancy risk; annual ultrasound and cholecystectomy for any polyp (regardless of size) is recommended.
- Colorectal cancer risk is markedly increased with concomitant IBD; annual colonoscopy with random biopsies is mandatory from PSC diagnosis.
- Hepatocellular carcinoma (HCC) surveillance with 6-monthly ultrasound ± AFP in all cirrhotic PSC patients.
- No proven disease-modifying therapy exists; ursodeoxycholic acid (UDCA) is not routinely recommended at high dose (≥20 mg/kg/day) and remains controversial at moderate dose (13–15 mg/kg/day).
- ERCP with endoscopic balloon dilation of dominant strictures is the preferred intervention; routine stenting is not recommended and may increase cholangitis risk.
- Antibiotic prophylaxis (e.g., ciprofloxacin or norfloxacin) should be considered for recurrent cholangitis episodes.
- Liver transplantation is the only curative option for end-stage PSC; disease recurrence occurs in approximately 20% of transplant recipients.
- Median transplant-free survival is 12–18 years; PSC disproportionately affects young males with a male-to-female ratio of approximately 2:1.
- Aboriginal and Torres Strait Islander patients may face barriers to specialist hepatology access and surveillance programme adherence, particularly in remote areas.
Introduction & Australian Epidemiology
Primary sclerosing cholangitis (PSC) is a chronic, progressive cholestatic liver disease characterised by inflammation, fibrosis, and stricturing of the intrahepatic and extrahepatic bile ducts. It is considered a pre-malignant condition with significant morbidity and reduced life expectancy.
Australian epidemiology: The estimated prevalence in Australia is 3–16 per 100,000 population, with an incidence of approximately 0.9–1.3 per 100,000 per year. PSC predominantly affects males (male-to-female ratio 2:1), with a median age at diagnosis of 30–40 years. Approximately 60–80% of Australian patients with PSC have concomitant inflammatory bowel disease (IBD), predominantly ulcerative colitis.
PSC carries a cumulative lifetime risk of cholangiocarcinoma (CCA) of 10–15%, colorectal cancer risk is significantly increased with concurrent IBD, and gallbladder neoplasia is an important concern. Median transplant-free survival is 12–18 years from diagnosis. Liver transplantation remains the only curative treatment, with approximately 3,000–4,000 liver transplants performed annually across Australian transplant centres (Melbourne, Sydney, Brisbane, Adelaide, Perth).
The pathogenesis is incompletely understood but involves immune-mediated bile duct injury, genetic susceptibility (HLA-B8, DR3, DRW52a alleles), and likely environmental triggers such as translocation of intestinal microbiota across a permeable gut barrier. There is a strong overlap with the gut–liver axis, consistent with the high prevalence of IBD.
Diagnosis & Associations
Diagnostic Criteria
PSC is diagnosed based on a combination of cholestatic liver biochemistry, characteristic cholangiographic findings, and exclusion of secondary causes. There is no single pathognomonic test.
Cholangiographic Imaging
MRCP (magnetic resonance cholangiopancreatography) is the first-line imaging modality for PSC diagnosis. It is non-invasive and has a sensitivity of 85–95% and specificity of 80–90% for large-duct PSC.
- Characteristic findings: multifocal strictures with beading (intrahepatic ± extrahepatic bile ducts), pruning of the biliary tree, diverticula-like outpouchings.
- MRCP can also assess gallbladder pathology and pancreatic duct involvement.
- Available at all major Australian radiology centres; MBS item 63441 (MRCP) is available with appropriate clinical indication.
ERCP (endoscopic retrograde cholangiopancreatography) is reserved for therapeutic intervention (dilation of dominant strictures, tissue sampling) or when MRCP is equivocal. Diagnostic ERCP alone is no longer first-line due to procedural risks (post-ERCP pancreatitis 3–5%, cholangitis 1–3%).
Exclusion of Secondary Causes
| Secondary Cause | Key Discriminating Features | Investigations |
|---|---|---|
| IgG4-related sclerosing cholangitis | Elevated serum IgG4 (>1.4 g/L), older males, associated autoimmune pancreatitis, proximal bile duct strictures, mass-forming lesions | Serum IgG4, IgG4 immunostain on biopsy, pancreatic imaging (CT/MRI) |
| Ischaemic cholangiopathy | History of hepatic artery thrombosis, prior liver transplant, chemotherapy (e.g., FUDR), radiation | Doppler US, clinical history |
| Infectious cholangitis | HIV-associated (cryptosporidial), CMV cholangiopathy, parasitic (clonorchiasis, opisthorchiasis), recurrent pyogenic cholangitis | HIV serology, stool microscopy, serology |
| Secondary sclerosing cholangitis (ICU) | Critically ill patients, prolonged ICU stay, ischaemic injury, parenteral nutrition | Clinical context, MRCP pattern |
| Choledocholithiasis / post-surgical | Prior biliary surgery, cholecystectomy, stones | MRCP, ERCP with extraction |
Laboratory Findings
- Cholestatic pattern: elevated ALP (usually >2× ULN), GGT elevated, bilirubin normal early but rises with disease progression.
- Transaminases (ALT, AST) mildly elevated (usually <5× ULN); markedly elevated ALT suggests superimposed autoimmune hepatitis (PSC-AIH overlap, ~10% of paediatric PSC).
- p-ANCA positive in 30–80% of PSC patients (non-specific, not diagnostic).
- IgG levels mildly elevated in ~60%; IgG4 should be tested to exclude IgG4-SC.
- Autoantibodies: ANA and SMA may be present but are not diagnostic; anti-mitochondrial antibody (AMA) should be negative (positive AMA suggests PBC).
Liver Biopsy
Liver biopsy is not routinely required for the diagnosis of PSC when characteristic cholangiographic findings are present. However, it may be indicated in the following situations:
- Small-duct PSC: cholestatic biochemistry + histological periductal ("onion-skin") fibrosis but normal cholangiogram.
- Suspected PSC–autoimmune hepatitis overlap syndrome.
- Staging of hepatic fibrosis when non-invasive assessment is uncertain.
- When secondary causes require histological confirmation.
Histological features include periductal concentric ("onion-skin") fibrosis, bile duct proliferation, ductopenia, and fibrosis progressing to biliary cirrhosis. The Ludwig staging system (stages I–IV) is used for histological staging.
Small-Duct PSC
Association with Inflammatory Bowel Disease
The association between PSC and IBD is one of the strongest in hepatology:
- 60–80% of PSC patients have concurrent IBD; the majority have ulcerative colitis (UC) (~70%), with Crohn's disease in ~10% and indeterminate colitis in ~20%.
- PSC can be diagnosed before, concurrent with, or years after IBD onset.
- PSC-IBD has a distinct phenotype: right-sided or pancolonic predominance, rectal sparing, backwash ileitis, and higher colorectal cancer risk than IBD alone.
- Mandatory colonoscopy at PSC diagnosis for all patients (regardless of IBD history) with segmental biopsies to screen for IBD and dysplasia.
- Additional extra-hepatic associations: type 1 diabetes, coeliac disease, thyroiditis, retroperitoneal fibrosis, psoriasis.
Surveillance
PSC is a pre-malignant condition with multiple surveillance requirements. A structured surveillance programme is essential for all patients and should be coordinated through a hepatology centre.
Cholangiocarcinoma (CCA) Surveillance
- Annual MRI abdomen with MRCP — sensitivity for CCA detection is superior to CT. MBS item 63441 (MRCP) and 63510 (MRI liver) are available with specialist referral.
- CA 19-9 — optional adjunct; sensitivity 50–90%, specificity 50–80%. Elevated values (>100 U/mL) warrant urgent further investigation. CA 19-9 is not Lewis antigen–independent; 5–10% of the population are Lewis antigen–negative and cannot produce CA 19-9.
- Combination MRI/MRCP + CA 19-9 annually is the recommended approach (EASL 2022, AASLD 2010 consensus).
- Any new or progressive dominant stricture on MRCP, or CA 19-9 >100 U/mL, requires urgent ERCP with brush cytology ± FISH (fluorescence in situ hybridization for polysomy) and multidisciplinary hepatobiliary MDT review.
- Fluorodeoxyglucose (FDG)-PET/CT may be considered in equivocal cases but is not part of routine surveillance.
Gallbladder Neoplasia Surveillance
Gallbladder polyps in PSC patients carry a significantly higher malignancy risk (up to 50–60% of polyps in PSC may be dysplastic or malignant) compared to the general population.
- Annual gallbladder ultrasound for all PSC patients.
- Cholecystectomy is recommended for any gallbladder polyp detected in a PSC patient, regardless of size. This differs from the general population guideline (cholecystectomy for polyps ≥10 mm).
- Even polyps <5 mm in PSC patients should prompt cholecystectomy discussion at MDT, as malignant transformation can occur at any size.
- Post-cholecystectomy, continue annual gallbladder fossa ultrasound if cirrhotic (for incidental liver findings).
Colorectal Cancer Surveillance
- Annual colonoscopy with segmental biopsies (at minimum 4-quadrant biopsies every 10 cm + targeted biopsies of any lesions) for all PSC patients with concomitant IBD.
- Colonoscopy at PSC diagnosis for all patients (including those without known IBD), as 25–30% will have subclinical IBD.
- If initial colonoscopy is normal with no IBD, repeat colonoscopy every 3–5 years.
- Chromoendoscopy (with indigo carmine or methylene blue) or virtual chromoendoscopy (NBI, BLI) improves dysplasia detection and is recommended where available.
- Consider total proctocolectomy with ileal pouch-anal anastomosis (IPAA) for patients with refractory colonic dysplasia; note that pouchitis is common after IPAA in PSC patients (~50%).
- Mesalamine (5-ASA) for IBD does not reduce CRC risk in PSC and is not recommended as a chemopreventive agent specifically.
Hepatocellular Carcinoma (HCC) Surveillance
- HCC is less common in PSC than cholangiocarcinoma but can occur, particularly in patients with established cirrhosis.
- 6-monthly abdominal ultrasound ± serum AFP for all PSC patients with cirrhosis (consistent with Australian national HCC surveillance guidelines).
- CT or MRI may supplement ultrasound in patients with obesity, nodular cirrhotic livers, or indeterminate ultrasound findings.
- HCC surveillance should continue post-liver transplantation if there was pre-transplant cirrhosis (particularly within Milan criteria).
Surveillance Summary Table
| Malignancy | Surveillance Modality | Frequency | When to Start |
|---|---|---|---|
| Cholangiocarcinoma | MRI/MRCP ± CA 19-9 | Annual | At PSC diagnosis |
| Gallbladder neoplasia | Abdominal ultrasound | Annual | At PSC diagnosis |
| Colorectal cancer (with IBD) | Colonoscopy + biopsies | Annual | At PSC diagnosis |
| Colorectal cancer (without IBD) | Colonoscopy | Every 3–5 years | At PSC diagnosis |
| HCC (cirrhotic only) | Ultrasound ± AFP | 6-monthly | When cirrhosis diagnosed |
Additional Surveillance
- Bone densitometry (DXA): cholestatic liver disease is a risk factor for metabolic bone disease; DXA at diagnosis and every 2–3 years.
- Fat-soluble vitamin levels (A, D, E, K): check annually, particularly if bilirubin elevated or jaundiced.
- Vitamin D: supplement to maintain 25-OH vitamin D >75 nmol/L; vitamin D deficiency is highly prevalent in PSC.
- Hepatic function (LFTs, albumin, INR): every 3–6 months; ALP trends correlate with prognosis (ALP <1.5× ULN associated with better outcomes).
- Pruritus management: assess at each visit; consider cholestyramine 4 g BD–QDS (before meals), rifampicin 150–300 mg BD, naltrexone 25–50 mg daily if cholestatic pruritus.
Management
Disease-Modifying Therapy
Ursodeoxycholic Acid (UDCA)
The role of UDCA in PSC remains controversial:
- High-dose UDCA (≥20 mg/kg/day): Not routinely recommended. The HALT-C trial demonstrated potential harm (higher rates of clinical endpoints including death, transplant, and CCA). The 28–30 mg/kg/day dose showed worse outcomes.
- Moderate-dose UDCA (13–15 mg/kg/day): Controversial. Improves biochemistry (ALP reduction) but no proven survival benefit or reduction in CCA risk. Some guidelines (AASLD) suggest it may be used on a case-by-case basis, while others (EASL 2022) do not recommend routine use.
- Low-dose UDCA (≤10 mg/kg/day): Generally well tolerated; limited data on efficacy. May be considered pragmatically for cholestasis symptom relief.
- Australian practice: UDCA use is at the discretion of the treating hepatologist. If used, moderate dose (13–15 mg/kg/day) is preferred; high dose (≥20 mg/kg/day) should be avoided.
Other Investigational Agents
Several therapies are under investigation in clinical trials but are not currently recommended for routine use in PSC:
- Obeticholic acid (OCA): FXR agonist; phase 2/3 trials ongoing; no established benefit in PSC to date.
- Norursodeoxycholic acid (norUDCA): Phase 2 data showed ALP reduction; phase 3 trials in progress (CANTO trial).
- Vancomycin: Antibiotic with immunomodulatory properties; small studies showed ALP improvement in some patients, particularly in paediatric PSC. Not standard of care; under further investigation.
- Fibrates (bezafibrate, fenofibrate): PPAR agonists; limited data in PSC; may reduce ALP but no proven clinical benefit.
- Anti-TNF agents, vedolizumab, ustekinumab: For concurrent IBD; no evidence of benefit for PSC-specific outcomes. Vedolizumab may worsen PSC in some reports.
Endoscopic Management — Dominant Strictures
A dominant stricture in PSC is defined as a stricture <1.5 mm diameter in the common bile duct or <1.0 mm in a hepatic duct (Hoffmann criteria). Dominant strictures occur in approximately 45–58% of PSC patients.
- Balloon dilation: Targeted dilation of dominant strictures improves symptoms (pruritus, jaundice) and biochemical cholestasis in 70–80% of cases. Repeated dilations may be required.
- Stenting: Temporary stenting may be considered for refractory dominant strictures not responding to balloon dilation alone, or for bridging to transplant. Long-term stenting is associated with stent occlusion, bacterial colonisation, and recurrent cholangitis.
- Tissue sampling: All dominant strictures should be sampled with brush cytology ± FISH (fluorescence in situ hybridisation) to exclude cholangiocarcinoma. Sensitivity improves with combination of brush cytology + FISH (polysomy on FISH has 50–60% sensitivity, 80–90% specificity for malignancy).
- Peroral cholangioscopy (SpyGlass): Can be used for direct visualisation and targeted biopsy of suspicious strictures; improves CCA detection when combined with FISH.
- ERCP should be performed by experienced biliary endoscopists at centres with hepatobiliary MDT support.
Management of Cholangitis
Acute cholangitis is a common complication of PSC and a frequent cause of hospitalisation. Management includes:
Antibiotic Prophylaxis for Recurrent Cholangitis
Patients with recurrent episodes of cholangitis (≥2 per year) should be considered for long-term antibiotic prophylaxis:
Liver Transplantation
Liver transplantation is the only curative treatment for end-stage PSC and is indicated for patients with:
- Decompensated cirrhosis (ascites, encephalopathy, variceal bleeding).
- Recurrent cholangitis not amenable to endoscopic management.
- Intractable pruritus.
- Hepatopulmonary syndrome or portopulmonary hypertension.
- Early cholangiocarcinoma (within Milan criteria, typically in combination with neoadjuvant chemoradiation; highly selected patients).
- MELD score ≥15 or meeting specific listing criteria at the relevant Australian transplant centre.
Key transplantation considerations in PSC:
- PSC recurrence post-transplant: Occurs in approximately 20% of recipients (range 10–37% at 5–10 years). Recurrent PSC is diagnosed based on cholangiographic findings mimicking PSC, after exclusion of other causes (hepatic artery thrombosis, ABO incompatibility, anastomotic strictures). Recurrence may lead to re-transplantation.
- Living donor liver transplantation (LDLT): Available at selected Australian centres; may reduce wait-list time. Recurrence rates similar to deceased donor transplant.
- Colectomy timing: Patients with concurrent UC may require colectomy before or after transplant. Severe UC refractory to medical therapy may warrant pre-transplant colectomy. Post-transplant immunosuppression may exacerbate UC.
- Cholangiocarcinoma: Historically a contraindication; selected patients with early-stage, unresectable CCA may be eligible for transplant under neoadjuvant protocols (chemoradiation + transplant) — highly specialised, available at limited centres.
- Post-transplant immunosuppression: Tacrolimus-based regimens are standard. UDCA post-transplant for recurrent PSC is sometimes used but lacks robust evidence.
Pruritus Management
Cholestatic pruritus affects 30–70% of PSC patients and can significantly impair quality of life. Stepwise approach:
Metabolic Bone Disease
- Osteoporosis occurs in 15–30% of PSC patients; DXA at diagnosis and every 2–3 years.
- Calcium supplementation (1,000–1,200 mg/day) and vitamin D (cholecalciferol 1,000–2,000 IU/day) for all patients.
- Bisphosphonates (e.g., alendronate 70 mg PO weekly) if T-score ≤ −2.5 or fragility fracture. Avoid IV bisphosphonates if bilirubin >50 µmol/L (hepatotoxicity concern — use oral).
- Denosumab 60 mg SC 6-monthly is an alternative (PBS Authority Required for osteoporosis).
Fat-Soluble Vitamin Deficiency
Check levels annually, more frequently if jaundiced:
- Vitamin A: Retinol 25,000–50,000 IU PO weekly if deficient.
- Vitamin D: Cholecalciferol 1,000–5,000 IU/day PO; aim 25-OH vitamin D >75 nmol/L.
- Vitamin E: Tocopherol 400–800 IU/day PO if deficient.
- Vitamin K: Phytomenadione (vitamin K1) 10 mg PO/SC weekly if INR prolonged; 10 mg IV if bleeding.
Special Populations
Aboriginal and Torres Strait Islander Health
📚 References
- 1. European Association for the Study of the Liver (EASL). EASL Clinical Practice Guidelines on sclerosing cholangitis. J Hepatol. 2022;77(3):761–806.
- 2. Chapman R, Fevery J, Kalloo A, et al. Diagnosis and management of primary sclerosing cholangitis. Hepatology. 2010;51(2):660–678.
- 3. Lindor KD, Kowdley KV, Harrison ME. ACG Clinical Guideline: Primary Sclerosing Cholangitis. Am J Gastroenterol. 2015;110(5):646–659.
- 4. Karlsen TH, Folseraas T, Thorburn D, Vesterhus M. Primary sclerosing cholangitis — a comprehensive review. J Hepatol. 2017;67(6):1298–1323.
- 5. Boonstra K, Weersma RK, van Erpecum KJ, et al. Population-based epidemiology, malignancy risk, and outcome of primary sclerosing cholangitis. Hepatology. 2013;58(6):2045–2055.
- 6. Lindström L, Hultcrantz R, Boberg KM, Friis-Liby I, Bergquist A. Association between reduced levels of alkaline phosphatase and survival times of patients with primary sclerosing cholangitis. Clin Gastroenterol Hepatol. 2013;11(7):841–846.
- 7. Lazaridis KN, LaRusso NF. Primary Sclerosing Cholangitis. N Engl J Med. 2016;375(12):1161–1170.
- 8. Australian Institute of Health and Welfare (AIHW). Liver disease and liver cancer. Available at: https://www.aihw.gov.au. Accessed 2024.
- 9. Bowlus CL, Lim JK, Lindor KD. AGA Clinical Practice Update on Surveillance for Hepatobiliary Cancers in Patients With Primary Sclerosing Cholangitis: Expert Review. Clin Gastroenterol Hepatol. 2019;17(13):2416–2422.
- 10. Tabibian JH, Weeding E, Jorgensen RA, et al. Randomised clinical trial: vancomycin or metronidazole in patients with primary sclerosing cholangitis — a pilot study. Aliment Pharmacol Ther. 2013;37(6):604–612.
- 11. Fickert P, Hirschfield GM, Denk G, et al. norUrsodeoxycholic acid improves cholestasis in primary sclerosing cholangitis: results of a phase 2 dose-finding study. J Hepatol. 2019;70(3):538–548.
- 12. Torres J, Palmela C, Vieira HM, et al. Inflammatory bowel disease and primary sclerosing cholangitis: a population-based study. Aliment Pharmacol Ther. 2018;48(11–12):1235–1247.
- 13. Said K, Glaumann H, Bergquist A. Gallbladder disease in patients with primary sclerosing cholangitis. J Hepatol. 2008;48(4):598–605.
- 14. Rudolph G, Gotthardt D, Klöters-Plachky P, et al. Influence of dominant bile duct stenoses and biliary infections on outcome in primary sclerosing cholangitis. J Hepatol. 2009;51(1):149–155.
- 15. Graziadei IW, Wiesner RH, Marotta PJ, et al. Long-term results of patients undergoing liver transplantation for primary sclerosing cholangitis. Hepatology. 1999;30(5):1121–1127.