📋 Key Information Summary
- Universal HBsAg screening is recommended for all pregnant women in Australia at first antenatal visit, with repeat testing for high-risk women in the third trimester.
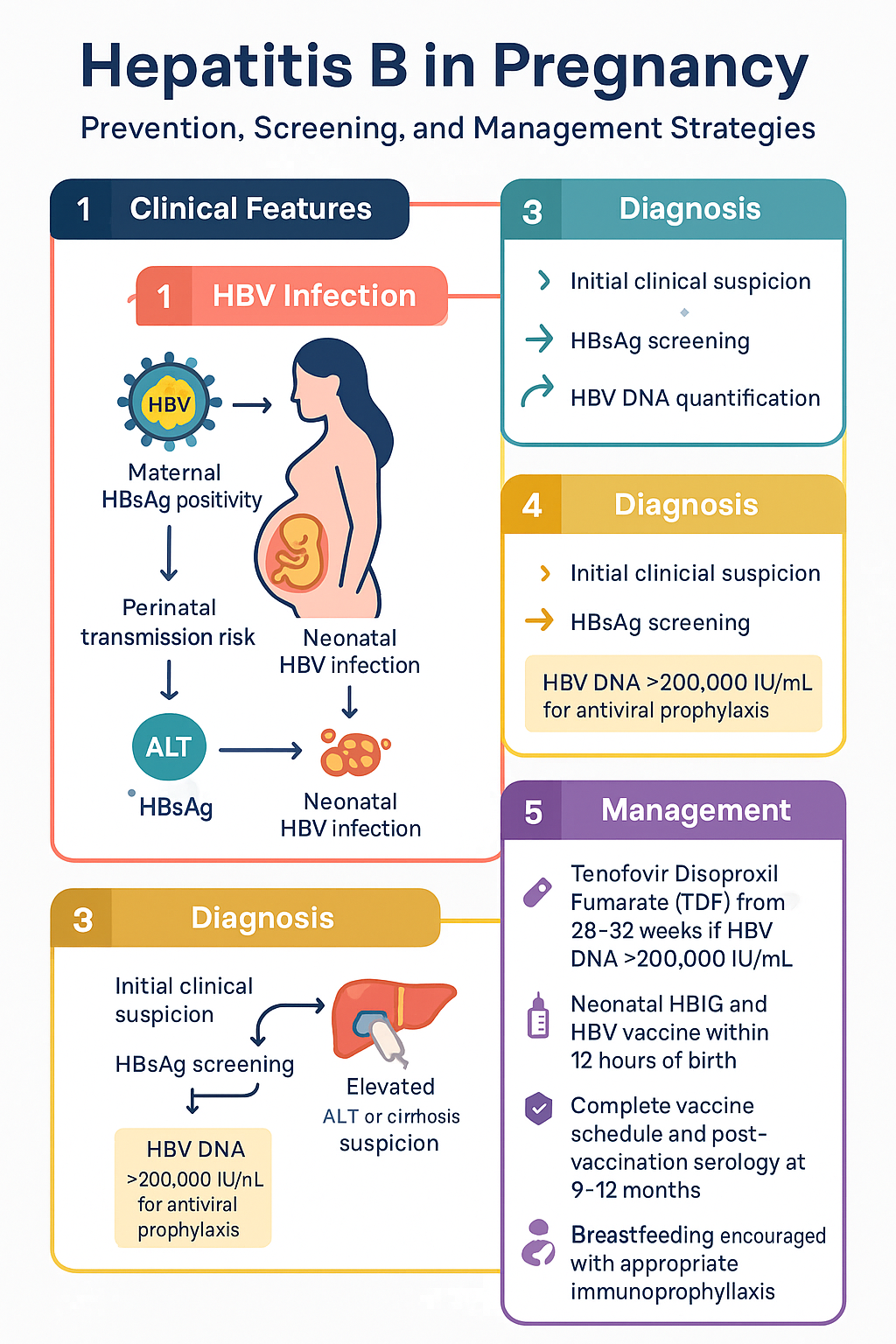
- Hepatitis B affects approximately 1% of the Australian population; perinatal transmission remains the most common route of chronic HBV acquisition globally.
- All HBsAg-positive pregnant women require HBV DNA quantification and ALT assessment to guide antiviral prophylaxis decisions and determine disease activity.
- Tenofovir disoproxil fumarate (TDF) 300 mg daily from 28–32 weeks' gestation is recommended when maternal HBV DNA exceeds 200,000 IU/mL to reduce vertical transmission risk.
- Women already receiving antiviral therapy for chronic HBV should continue treatment through pregnancy, with TDF preferred due to its established safety profile in pregnancy.
- Entecavir and tenofovir alafenamide (TAF) should be switched to TDF before conception or as soon as pregnancy is confirmed.
- All neonates born to HBsAg-positive mothers must receive hepatitis B immunoglobulin (HBIG) 100 IU IM plus monovalent HBV vaccine within 12 hours of birth, regardless of maternal viral load.
- The full hepatitis B vaccine schedule (at birth, 2 months, 4 months, 6 months — using hexavalent vaccine) must be completed for all exposed neonates.
- Post-vaccination serology (HBsAg and anti-HBs) is mandatory at 9–12 months of age to confirm immune response and exclude breakthrough infection.
- Breastfeeding is safe and encouraged for HBsAg-positive mothers provided the infant has received appropriate immunoprophylaxis.
- Aboriginal and Torres Strait Islander women have higher HBV prevalence; culturally safe screening programmes and antenatal partnerships are essential.
- Vertical transmission rates can be reduced from approximately 90% (without intervention) to below 1% with combined maternal antiviral prophylaxis and neonatal immunoprophylaxis.
Maternal Screening & Antiviral Prophylaxis
Universal HBsAg Screening in Pregnancy
All pregnant women in Australia should be screened for hepatitis B surface antigen (HBsAg) at the first antenatal visit, consistent with the National Perinatal Guidelines and the Australian National Hepatitis B Testing Policy. Universal screening identifies women at risk of perinatal transmission and allows timely initiation of preventive strategies.
Australia has a population prevalence of chronic HBV of approximately 1%, with higher rates among Aboriginal and Torres Strait Islander peoples (estimated 2–6% in some communities), people born in endemic regions (sub-Saharan Africa, East and South-East Asia, the Pacific Islands), and people who inject drugs.
Baseline Assessment for HBsAg-Positive Women
Once HBsAg positivity is confirmed, the following investigations should be performed promptly:
Antiviral Prophylaxis — Tenofovir Disoproxil in the Third Trimester
Maternal antiviral prophylaxis aims to reduce the risk of in-utero and intrapartum HBV transmission by suppressing viral load prior to delivery. The principal indication for prophylactic antiviral therapy in previously untreated women is a maternal HBV DNA level >200,000 IU/mL.
Women Already on Antiviral Therapy
Women who are already receiving antiviral treatment for chronic HBV at the time of conception should continue therapy throughout pregnancy. The choice of agent requires review:
- TDF (Viread®): Preferred agent — continue unchanged throughout pregnancy.
- Entecavir (Baraclude®): Switch to TDF pre-conception or as soon as pregnancy is confirmed; entecavir has less pregnancy safety data.
- Tenofovir alafenamide (TAF — Vemlidy®): Switch to TDF pre-conception or at confirmation of pregnancy; insufficient pregnancy safety data.
- Lamivudine: May be continued if already established, though TDF is preferred due to superior potency and lower resistance risk.
- Interferon-alpha: Contraindicated in pregnancy — must be ceased pre-conception with adequate washout.
Effectiveness of Combined Prophylaxis
| Strategy | Approximate vertical transmission rate | Notes |
|---|---|---|
| No intervention | 70–90% (if HBeAg+) | Highest risk with high viral load and HBeAg positivity |
| Neonatal immunoprophylaxis alone (HBIG + vaccine) | 5–15% | Failure rate increases with maternal HBV DNA >200,000 IU/mL |
| Maternal TDF + neonatal immunoprophylaxis | <1–2% | Current best-practice standard; landmark RCTs (Pan et al., JAMA 2016) |
Neonatal Management
Immediate Post-Exposure Prophylaxis (Within 12 Hours of Birth)
All neonates born to HBsAg-positive mothers — regardless of maternal viral load, HBeAg status, or whether the mother received antiviral prophylaxis — must receive dual immunoprophylaxis within 12 hours of birth. This is a critical time-sensitive intervention.
Complete Vaccine Schedule
Following the birth dose, the infant should complete the standard hepatitis B vaccination schedule as part of the National Immunisation Program (NIP). In Australia, this is delivered via the hexavalent combination vaccine (DTPa-hepB-IPV-Hib).
| Dose | Age | Vaccine | Funding |
|---|---|---|---|
| 1 (birth) | At birth (≤12 hours) | Monovalent HBV (Engerix-B® 10 µg or HB-Vax II® 5 µg) | NIP funded for at-risk neonates |
| 2 | 2 months | Hexavalent (Infanrix hexa® or Vaxelis®) | NIP funded — all infants |
| 3 | 4 months | Hexavalent (Infanrix hexa® or Vaxelis®) | NIP funded — all infants |
| 4 | 6 months | Hexavalent (Infanrix hexa® or Vaxelis®) | NIP funded — all infants |
Post-Vaccination Serology
Post-vaccination serology is essential to confirm successful immunisation and to exclude breakthrough HBV infection. Testing should be performed at 9–12 months of age (i.e., at least 4 weeks after the final scheduled vaccine dose).
Breastfeeding
Breastfeeding is safe and encouraged for HBsAg-positive mothers. There is no evidence that breastfeeding increases the risk of HBV transmission when the infant has received appropriate immunoprophylaxis (HBIG + vaccine). The WHO, Australian Breastfeeding Association, and Australian Society of Clinical Immunology and Allergy (ASCIA) all support breastfeeding in this context.
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Pan CQ, Duan Z, Dai E, et al. Tenofovir to prevent hepatitis B transmission in mothers with high viral load. N Engl J Med. 2016;374(24):2324–2334.
- 2. Jourdain G, Ngo-Giang-Huong N, Harrison L, et al. Tenofovir versus placebo to prevent perinatal transmission of hepatitis B. N Engl J Med. 2018;378(10):911–923.
- 3. World Health Organization. Guidelines for the prevention, care and treatment of persons with chronic hepatitis B infection. Geneva: WHO; 2015 (updated March 2024).
- 4. Australian Government Department of Health and Aged Care. Australian National Immunisation Program Schedule. Canberra: Commonwealth of Australia; 2024.
- 5. The Royal Australian College of General Practitioners (RACGP). Australian Immunisation Handbook — Hepatitis B. Updated 2024. Available at: immunisationhandbook.health.gov.au.
- 6. Visvanathan K, Dusheiko G, Giles M, et al. Managing HBV in pregnancy. Prevention, prophylaxis, and treatment. J Hepatol. 2016;65(3):562–575.
- 7. Australian Institute of Health and Welfare (AIHW). Hepatitis B and C in Australia — Annual Surveillance Report 2023. Canberra: AIHW; 2023.
- 8. National Perinatal Epidemiology and Statistics Unit (NPESU). Antenatal Screening for Infectious Diseases in Australia. Sydney: NPESU, UNSW; 2022.
- 9. Australian Government. National Aboriginal and Torres Strait Islander Hepatitis B Strategy 2018–2022. Canberra: Commonwealth of Australia; 2018.
- 10. Dionne-Odom J, Tita ATN, Silverman NS. #38: Hepatitis B in pregnancy screening, treatment, and prevention of vertical transmission. Am J Obstet Gynecol. 2016;214(1):6–14.
- 11. Yi P, Chen R, Huang Y, Zhou RR, Fan XG. Management of mother-to-child transmission of hepatitis B virus: Propositions and challenges. J Clin Virol. 2016;77:32–39.
- 12. Terrault NA, Lok ASF, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology. 2018;67(4):1560–1599.