📋 Key Information Summary
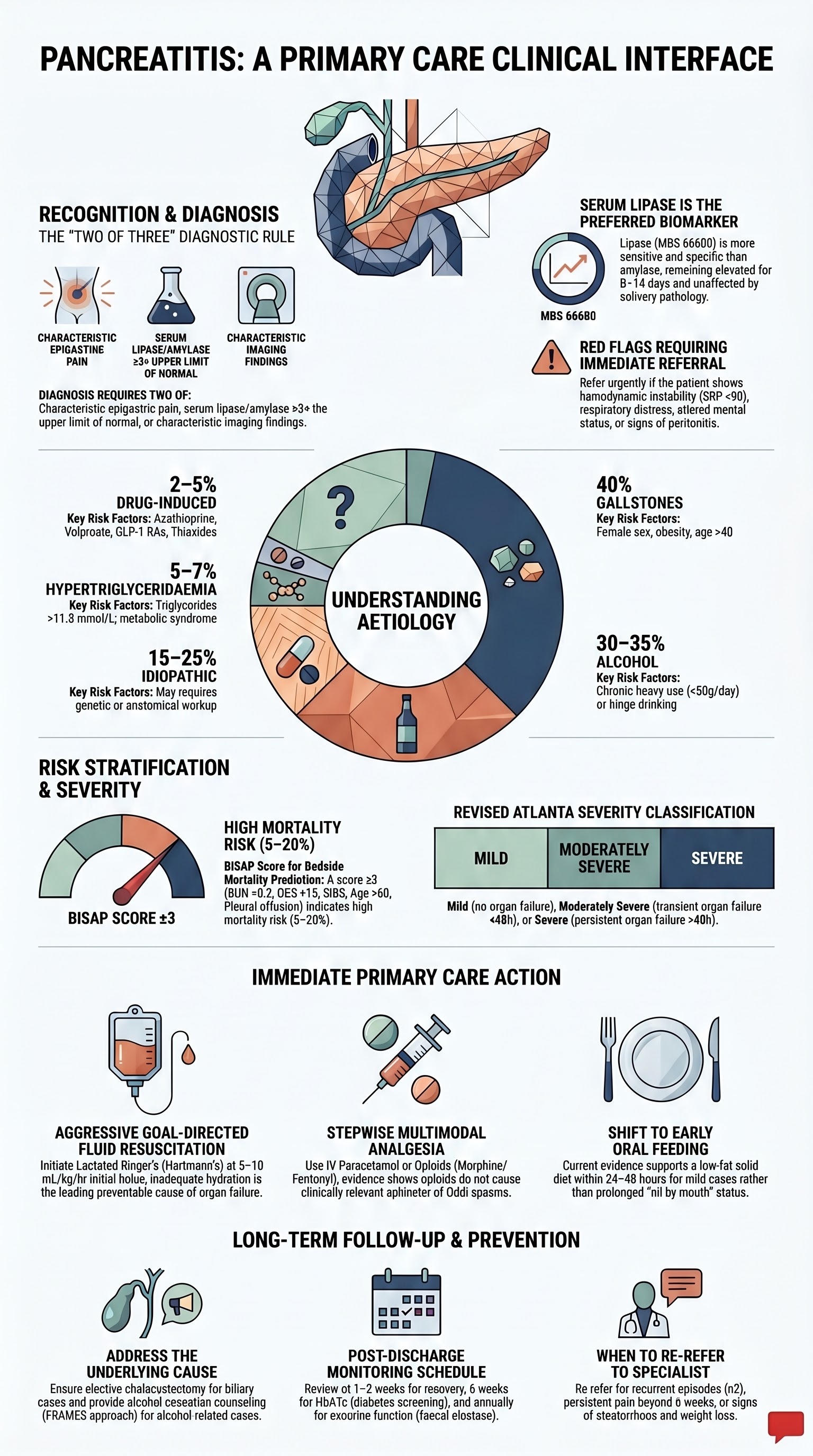
- Acute pancreatitis presents with severe epigastric pain radiating to the back, often with nausea and vomiting; serum lipase ≥3× the upper limit of normal is the diagnostic threshold.
- The two leading aetiologies in Australia are gallstones (~40%) and alcohol (~30%); medications and hypertriglyceridaemia account for a further 10–15%.
- Most suspected acute pancreatitis requires emergency department assessment — primary care role is early recognition, initial analgesia, nil by mouth, and prompt referral.
- Aggressive IV fluid resuscitation (lactated Ringer's solution, 5–10 mL/kg/hr initial bolus then target-guided) within the first 24 hours reduces organ failure and mortality.
- The Revised Atlanta Classification stratifies severity into mild (no organ failure, no local complications), moderately severe (transient organ failure <48 h), and severe (persistent organ failure ≥48 h).
- BISAP score (BUN >8.2 mmol/L, impaired mental status, SIRS, age >60, pleural effusion) ≥3 predicts high mortality and guides escalation of care.
- Cholangitis or persistent biliary obstruction requires urgent ERCP within 24–72 hours; magnetic resonance cholangiopancreatography (MRCP) or endoscopic ultrasound can confirm choledocholithiasis.
- Primary care follow-up must address the underlying cause: alcohol cessation counselling, triglyceride management (target <1.7 mmol/L with fibrates), and elective cholecystectomy for biliary pancreatitis.
- Post-discharge monitoring includes repeat lipase/amylase if symptomatic, HbA1c/fasting glucose for new-onset diabetes, and faecal elastase for exocrine insufficiency after recurrent episodes.
- Drug-induced pancreatitis requires immediate cessation of the offending agent; high-risk drugs include azathioprine, valproate, GLP-1 receptor agonists, and thiazide diuretics.
- Aboriginal and Torres Strait Islander Australians have significantly higher rates of gallstone disease, alcohol-related pancreatitis, and hypertriglyceridaemia, compounded by rural and remote access barriers.
- Patients with recurrent acute pancreatitis (≥2 episodes) should be referred to a gastroenterologist for consideration of genetic testing (PRSS1, SPINK1, CFTR), autoimmune workup, and CT/MRI pancreas protocol imaging.
Introduction & Australian Epidemiology
Acute pancreatitis is an inflammatory condition of the pancreas that accounts for a significant and increasing burden on Australian emergency departments and hospitals. It ranges from a self-limiting disease (approximately 80% of cases) to a life-threatening condition with multi-organ failure and mortality rates of 20–30% in severe cases. The primary care clinician plays a critical role in early recognition, initial management, timely referral, and long-term follow-up to prevent recurrence.
In Australia, acute pancreatitis results in approximately 15,000–20,000 hospital admissions per year, with an age-standardised incidence of 30–40 per 100,000 population. Incidence has been rising over the past two decades, driven by increasing gallstone disease (linked to obesity), alcohol consumption patterns, and metabolic syndrome-related hypertriglyceridaemia. The disease carries an overall mortality of 2–5%, but this rises sharply in the elderly and those with systemic inflammatory response syndrome (SIRS) or organ failure.
Gallstone pancreatitis accounts for approximately 40% of cases nationally and is more prevalent in women over 40 years. Alcoholic pancreatitis, representing 30–35% of cases, is more common in men aged 30–50 and is disproportionately over-represented in Aboriginal and Torres Strait Islander communities. Idiopathic pancreatitis, diagnosed when no clear cause is identified after initial workup, accounts for 15–25% of presentations; a proportion of these have a genetic or anatomical basis (e.g., pancreas divisum, SPINK1/PRSS1 mutations) identifiable with specialist evaluation.
| Aetiology | Proportion (%) | Key Associations |
|---|---|---|
| Gallstones | 40% | Female sex, obesity, age >40, Aboriginal and Torres Strait Islander populations |
| Alcohol | 30–35% | Chronic heavy use (>50 g/day), binge drinking, male predominance |
| Idiopathic | 15–25% | Requires further workup; consider genetic, anatomical, microlithiasis |
| Hypertriglyceridaemia | 5–7% | Triglycerides >11.3 mmol/L; diabetes, metabolic syndrome, familial |
| Drug-induced | 2–5% | Azathioprine, valproate, GLP-1 RAs, thiazides, mesalazine |
| Other | 3–5% | Post-ERCP, trauma, autoimmune (IgG4), hereditary, malignancy |
Recognition & Risk Factors
Clinical Presentation
Acute pancreatitis classically presents with the acute onset of severe, constant epigastric pain that radiates to the back (present in 50–60% of cases). The pain is typically worse after eating and may be partially relieved by sitting forward. Associated symptoms include nausea, vomiting (often persistent and not relieving pain), anorexia, and abdominal distension.
On examination, patients may be tachycardic (reflecting SIRS and hypovolaemia), febrile (low-grade; high fever suggests infected necrosis or cholangitis), and have marked tenderness in the epigastrium with or without guarding. Cullen's sign (periumbilical ecchymosis) and Grey Turner's sign (flank ecchymosis) are rare but indicate severe haemorrhagic pancreatitis.
Diagnostic Criteria
The diagnosis of acute pancreatitis requires two of the following three criteria (Revised Atlanta Classification 2012):
- Characteristic abdominal pain (acute onset, severe, epigastric, often radiating to the back)
- Serum lipase (or amylase) ≥3 times the upper limit of normal
- Characteristic findings on cross-sectional imaging (CT, MRI, or ultrasound)
Risk Factors for Acute Pancreatitis
Medications Implicated in Drug-Induced Pancreatitis
| Drug Class | Examples | Evidence Strength | Typical Latency |
|---|---|---|---|
| Immunosuppressants | Azathioprine, 6-mercaptopurine | Definite (Class Ia) | Days to months |
| Antiepileptics | Valproate | Definite (Class Ia) | Weeks to months |
| GLP-1 Receptor Agonists | Exenatide, liraglutide, semaglutide, dulaglutide | Probable (Class II) | Weeks to years |
| Diuretics | Thiazides, furosemide | Probable (Class II) | Weeks to months |
| 5-ASA compounds | Mesalazine, sulfasalazine | Probable (Class II) | Days to months |
| NRTIs | Didanosine, stavudine | Definite (Class Ia) | Weeks to years |
| Statins | Simvastatin, atorvastatin | Possible (Class III) | Months |
Pathophysiology
Acute pancreatitis is initiated by premature intracellular activation of trypsinogen to trypsin within pancreatic acinar cells. This triggers a cascade of digestive enzyme activation (elastase, phospholipase A2, kallikrein) leading to autodigestion of the pancreas and peripancreatic tissues. The resultant injury activates nuclear factor-κB (NF-κB) signalling, amplifying local and systemic inflammatory responses.
In gallstone pancreatitis, obstruction of the common bile duct or pancreatic duct by a migrating stone causes ductal hypertension and enzyme reflux. In alcohol-related disease, ethanol metabolites (fatty acid ethyl esters) are directly toxic to acinar cells, promote intracellular calcium overload, and impair autophagy. In hypertriglyceridaemia, free fatty acids released by pancreatic lipase from excess triglycerides cause direct lipotoxic injury to acinar cells and vascular endothelium.
Two-Phase Model of Severe Pancreatitis
The Revised Atlanta Classification (2012) classifies local complications based on time course and content: acute peripancreatic fluid collection (APFC, <4 weeks, homogeneous), pseudocyst (>4 weeks, encapsulated, no solid debris), acute necrotic collection (ANC, <4 weeks, heterogeneous), and walled-off necrosis (>4 weeks, encapsulated, heterogeneous).
Investigations
Initial Laboratory Assessment
Investigations should be performed in the emergency department or hospital setting. The primary care clinician should request these if the patient presents to general practice acutely, alongside arranging transfer.
Imaging
Risk Stratification & Severity Scoring
Risk stratification should be performed at presentation and at 48 hours. The Revised Atlanta Classification is the standard framework, and the BISAP score is a practical bedside tool for primary care and emergency settings.
Revised Atlanta Classification — Severity
BISAP Score (Bedside Index for Severity in Acute Pancreatitis)
Score calculated within first 24 hours. Score ≥3 indicates high risk of mortality (5–20%).
| Parameter | Criterion | Points |
|---|---|---|
| BUN | >8.2 mmol/L (25 mg/dL) | 1 |
| Impaired mental status | GCS <15 or disorientation | 1 |
| SIRS | ≥2 of: T <36 or >38°C, HR >90, RR >20, WCC <4 or >12×10⁹/L, PaCO₂ <32 mmHg | 1 |
| Age | >60 years | 1 |
| Pleural effusion | Present on imaging or CXR | 1 |
Ranson's Criteria (Revised)
| At Admission | At 48 Hours |
|---|---|
| Age >55 years | HCT fall >10% |
| WCC >16×10⁹/L | BUN rise >1.8 mmol/L |
| Glucose >10 mmol/L | Ca²⁺ <2.0 mmol/L |
| LDH >350 IU/L | PaO₂ <60 mmHg |
| AST >250 IU/L | Base deficit >4 mEq/L |
| Fluid sequestration >6 L |
Gallstone pancreatitis (non-operated): ≥3 criteria = severe. Alcoholic pancreatitis: ≥6 criteria = severe. Mortality rises significantly with increasing scores.
Immediate Management
Most patients with suspected acute pancreatitis require emergency department assessment and hospital admission. The primary care clinician's role is early recognition, initial resuscitation measures, and rapid referral. The following management should be initiated in the ED and continued on the ward.
1. Fluid Resuscitation
Aggressive goal-directed fluid therapy is the single most important intervention in the first 24–48 hours. Inadequate fluid resuscitation is the most common preventable cause of organ failure.
Fluid resuscitation targets (goal-directed): Target BUN <7.1 mmol/L, decreasing haematocrit, urine output >0.5 mL/kg/hr, improving heart rate, and normalising lactate. Avoid aggressive fluid overload in elderly patients and those with cardiac or renal comorbidities — reassess volume status every 4–6 hours using clinical, biochemical, and point-of-care ultrasound parameters.
2. Analgesia
Pain management is a priority. Pancreatitis pain can be severe and undertreated. A stepwise multimodal approach is recommended. There is no evidence that opioids cause sphincter of Oddi spasm clinically relevant to pancreatitis outcomes — pain relief should not be withheld due to this theoretical concern.
3. Antiemetic Therapy
4. Nil by Mouth & Nutritional Support
Traditional management mandated nil by mouth until pain resolved and enzymes normalised. Current evidence supports early oral feeding (within 24–48 hours) in mild pancreatitis with a low-fat solid diet — there is no benefit of prolonged fasting or clear-fluid diet stepping. Nasogastric feeding should be initiated if the patient cannot eat by 48–72 hours. Enteral nutrition (via nasojejunal tube if NG feeding not tolerated) is preferred over parenteral nutrition, which increases infectious complications.
5. Gallstone Pancreatitis — Urgent ERCP
Urgent ERCP (within 24–72 hours) is indicated for patients with concurrent cholangitis (fever, jaundice, right upper quadrant pain — Charcot's triad) or persistent biliary obstruction (bilirubin >40 µmol/L, dilated CBD on imaging). ERCP is not indicated for uncomplicated gallstone pancreatitis without cholangitis or persistent obstruction — early cholecystectomy during the same admission is the standard of care.
6. Prophylactic Antibiotics
Prophylactic antibiotics are not recommended for sterile necrotising pancreatitis (multiple RCTs, including the landmark Dutch and German trials, show no mortality benefit). Antibiotics are indicated for confirmed or strongly suspected infected necrosis (gas in necrosis on CT, positive FNA culture, persistent sepsis ≥7–10 days after onset) and for concurrent infections (cholangitis, pneumonia, UTI, line sepsis).
7. Specific Interventions by Aetiology (Acute Phase)
| Aetiology | Acute Intervention | Timing |
|---|---|---|
| Gallstone with cholangitis | Urgent ERCP + sphincterotomy ± stone extraction | Within 24 hours |
| Gallstone without cholangitis | Same-admission cholecystectomy (laparoscopic) | Before discharge (once pain resolved, enzymes trending down) |
| Hypertriglyceridaemia (>11.3 mmol/L) | Insulin infusion 0.1–0.3 U/kg/hr ± heparin 500 U bolus; plasmapheresis if TG >22.6 mmol/L or refractory | Immediate |
| Alcohol-related | Supportive care; alcohol withdrawal protocol if at risk; thiamine 100–300 mg IV/PO daily | Immediate; ongoing |
| Drug-induced | Immediate cessation of suspected agent; document and counsel | As soon as identified |
| Post-ERCP | Aggressive IV fluids, standard analgesia; usually self-limiting | Immediate |
Primary Care Follow-Up
After discharge from hospital, the patient's ongoing care should be managed in close coordination with their general practitioner. The primary care clinician is central to addressing the underlying cause, preventing recurrence, monitoring for complications, and managing long-term sequelae such as pancreatic exocrine insufficiency and new-onset diabetes.
First Visit After Discharge (Within 1–2 Weeks)
Addressing Underlying Causes — Long-Term Management
Alcohol Cessation
For patients with alcohol-related pancreatitis, complete abstinence is the single most effective intervention to prevent recurrence. Even moderate alcohol resumption (1–2 standard drinks/day) significantly increases recurrence risk. The GP should:
- Provide brief intervention and motivational interviewing (using the FRAMES approach or 5As framework)
- Refer to community alcohol and drug services, counselling, or rehabilitation as appropriate
- Consider pharmacotherapy for alcohol dependence: naltrexone (Revia®) 50 mg PO daily or acamprosate (Campral®) 666 mg PO TDS
- Screen for alcohol withdrawal risk at discharge; ensure community-based withdrawal management if not completed in hospital
- Monitor LFTs (GGT trend), CDT (carbohydrate-deficient transferrin) as objective markers of abstinence
Gallstone Management
- Same-admission cholecystectomy: Current evidence (PONCHO trial) supports laparoscopic cholecystectomy during the index admission for mild gallstone pancreatitis. This reduces readmission for recurrent biliary events from 17% (delayed cholecystectomy at 2–4 weeks) to 5%.
- If cholecystectomy was not performed: Ensure the patient is on the surgical waiting list. Urgent referral if there is recurrent biliary colic or pancreatitis. A low-fat diet should be advised in the interim.
- In patients unfit for surgery: Endoscopic sphincterotomy reduces recurrence risk but is less effective than cholecystectomy. Ursodeoxycholic acid (UDCA) may reduce gallstone recurrence.
Hypertriglyceridaemia Management
Patients with pancreatitis secondary to hypertriglyceridaemia require aggressive lipid management to prevent recurrence. Target triglyceride level: <1.7 mmol/L (ideally), <5.6 mmol/L (absolute minimum to prevent recurrence).
- Dietary modification: Very low-fat diet (<20% of calories from fat), eliminate simple sugars and alcohol, Mediterranean-style diet. Dietitian referral essential.
- Weight loss: If overweight/obese, even 5–10% weight reduction significantly lowers triglycerides.
- Diabetes optimisation: Tight glycaemic control (HbA1c target <53 mmol/mol / <7%).
- Fibrate therapy: First-line pharmacotherapy. Fenofibrate reduces triglycerides by 30–50%.
- Icosapent ethyl (Vascepa®): EPA-based omega-3 fatty acid; reduces triglycerides by 20–30%. PBS listed for severe hypertriglyceridaemia.
- Combination therapy: Fibrates + omega-3s ± niacin for refractory cases. Avoid statin + fibrate combinations (increased myopathy risk) — if needed, fenofibrate is the preferred fibrate with statins.
Medication Review
If drug-induced pancreatitis is suspected, permanently discontinue the offending agent and document the reaction. If the medication is essential (e.g., azathioprine for IBD or transplant), specialist discussion regarding rechallenge or alternative is required. Document pancreatitis as an adverse drug reaction in the patient's record and the Australian Adverse Drug Reaction Reporting System (ADRAC/TGA) if appropriate.
Monitoring Schedule in Primary Care
| Timepoint | Assessment | Investigations |
|---|---|---|
| 1–2 weeks post-discharge | Clinical review, pain, diet tolerance, wound check (if surgical), medication reconciliation | Repeat lipase if symptomatic, LFTs, glucose, renal function |
| 6 weeks | Weight, alcohol status, lipid profile review, diabetes screening, specialist follow-up compliance | HbA1c, fasting lipids, faecal elastase if symptoms of steatorrhoea |
| 3 months | Ongoing cause-specific management (alcohol abstinence, triglycerides), psychological wellbeing | Lipids (if hypertriglyceridaemia), CDT (if alcohol-related), HbA1c |
| 6 months | Long-term disease burden assessment, ongoing specialist liaison, recurrence risk review | Full metabolic panel, lipids, HbA1c, faecal elastase if indicated |
| Annually (ongoing) | Preventive care, recurrence vigilance, diabetes screening, exocrine function, cholecystectomy follow-up | HbA1c, lipids, faecal elastase, nutritional markers (albumin, B12, fat-soluble vitamins) |
When to Re-Refer
- Recurrent acute pancreatitis (≥2 episodes) — for specialist evaluation including genetic testing (PRSS1, SPINK1, CFTR, CTRC), autoimmune serology (IgG4), and cross-sectional imaging
- Persistent pain beyond 4–6 weeks — consider chronic pancreatitis, pseudocyst, or ductal complications
- Steatorrhoea, weight loss, or nutritional deficiency — consider exocrine pancreatic insufficiency (faecal elastase <200 µg/g); initiate pancreatic enzyme replacement therapy (PERT)
- New-onset diabetes mellitus — endocrinology referral if insulin-dependent or difficult to control
- Pancreatic mass or cystic lesion discovered on imaging — urgent gastroenterology/oncology referral
Recurrence Prevention — Patient Counselling Points
- Complete alcohol abstinence (if alcohol-related aetiology) or moderation (<2 standard drinks/day, <10/week)
- Low-fat diet with gradual liberalisation; avoid high-fat meals and fried foods
- Smoking cessation — smoking is an independent risk factor for recurrent and chronic pancreatitis
- Regular exercise and weight management (BMI target 18.5–25)
- Maintain hydration, especially during illness or fasting
- Return of severe epigastric pain radiating to the back
- Persistent vomiting preventing oral intake for >12 hours
- Fever (>38.5°C) with abdominal pain
- Jaundice (yellow skin/eyes, dark urine, pale stools)
- Signs of dehydration (dizziness, reduced urine output, confusion)
Special Populations
Pregnancy
Paediatrics
Elderly (≥65 Years)
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander Australians experience a disproportionately high burden of acute pancreatitis, with hospitalisation rates approximately 2–3 times those of the non-Indigenous population, and significantly higher mortality. This disparity is driven by a convergence of higher rates of gallstone disease, harmful alcohol use, metabolic syndrome, hypertriglyceridaemia, and barriers to timely healthcare access in rural and remote communities.
📚 References
- 1. Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis — 2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62(1):102-111.
- 2. Tenner S, Baillie J, DeWitt J, Vege SS. American College of Gastroenerology guideline: management of acute pancreatitis. Am J Gastroenterol. 2013;108(9):1400-1415.
- 3. Working Group IAP/APA Acute Pancreatitis Guidelines. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology. 2013;13(4 Suppl 2):e1-e15.
- 4. Crockett SD, Wani S, Gardner TB, Falck-Ytter Y, Barkun AN; American Gastroenterological Association Institute Clinical Guidelines Committee. American Gastroenterological Association Institute guideline on initial management of acute pancreatitis. Gastroenterology. 2018;154(4):1096-1101.
- 5. Bakker OJ, van Brunschot S, van Santvoort HC, et al. Early versus on-demand nasenteric feeding in acute pancreatitis. N Engl J Med. 2014;371(21):1983-1993. (PANTHER trial)
- 6. van Santvoort HC, Besselink MG, Bakker OJ, et al. A step-up approach or open necrosectomy for necrotizing pancreatitis. N Engl J Med. 2010;362(16):1491-1502. (PANTER trial)
- 7. da Costa DW, Bouwense SA, Schepers NJ, et al. Same-admission versus interval cholecystectomy for mild gallstone pancreatitis (PONCHO): a multicentre randomised controlled trial. Lancet. 2015;386(10000):1261-1268.
- 8. Yadav D, Lowenfels AB. The epidemiology of pancreatitis and pancreatic cancer. Gastroenterology. 2013;144(6):1252-1261.
- 9. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework: Summary report 2023. Canberra: AIHW; 2023.
- 10. Navarro S, Cubiella J, Feu F, et al. Hypertriglyceridemic acute pancreatitis. Diagnosis and treatment. Pancreatology. 2020;20(4):571-577.
- 11. Working Group of the International Association of Pancreatology (IAP). IAP guidelines for the surgical management of acute pancreatitis. Pancreatology. 2013;13(4 Suppl 2):e16-e22.
- 12. Garg PK, Singh VP. Organ failure due to systemic injury in acute pancreatitis. Gastroenterology. 2019;156(7):2008-2023.
- 13. Talukdar R, Vege SS. Recent developments in acute pancreatitis. Clin Gastroenterol Hepatol. 2017;15(6):799-806.
- 14. Buxbaum JL, Quezada M, Chong B, et al. Early aggressive hydration hastens clinical improvement in mild acute pancreatitis. Am J Gastroenterol. 2017;112(5):797-803.
- 15. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.