📋 Key Information Summary
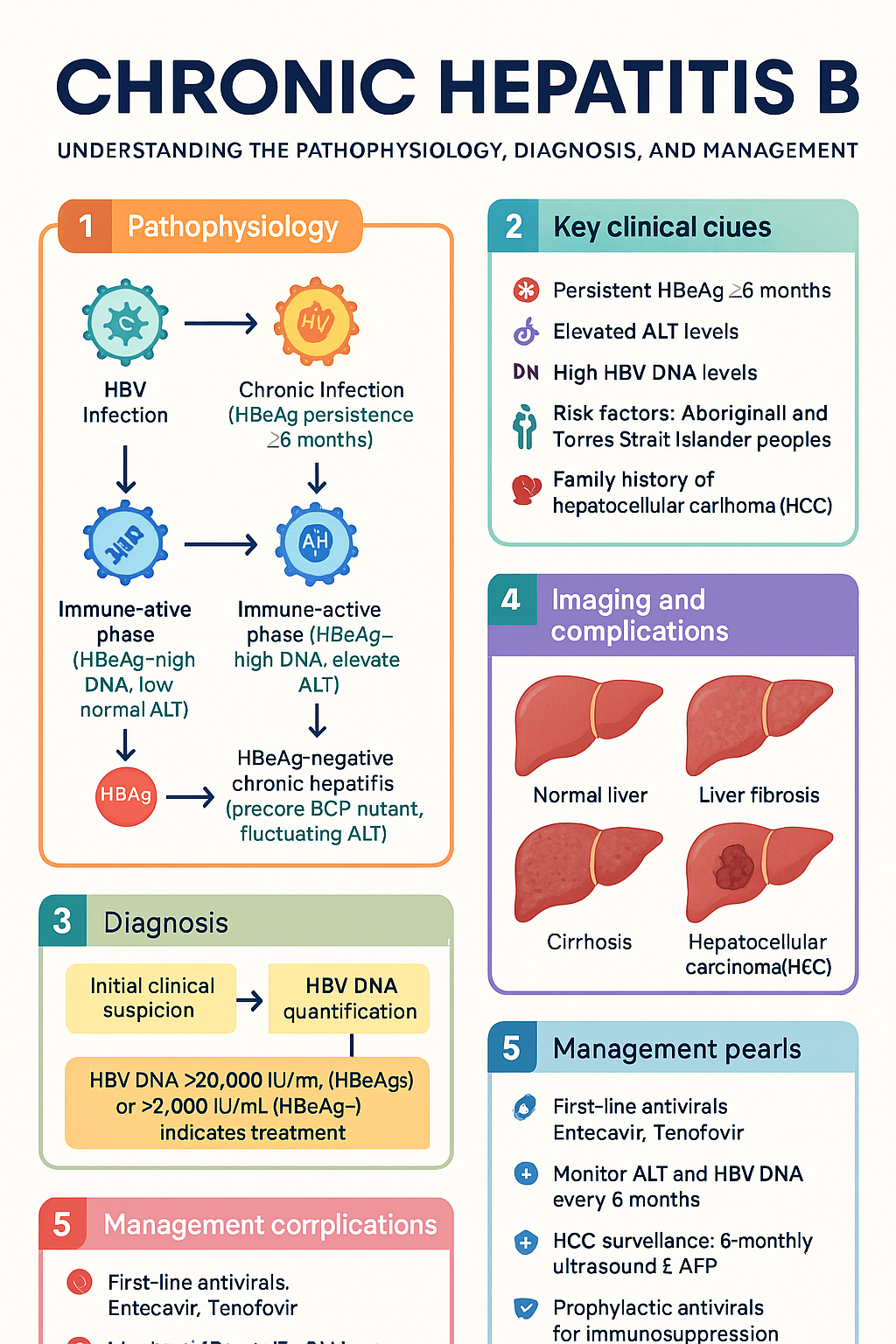
- Diagnosis: Chronic hepatitis B (CHB) defined by persistence of HBsAg for ≥6 months; approximately 230,000 people living with CHB in Australia, with significant under-diagnosis particularly among Aboriginal and Torres Strait Islander peoples and culturally diverse communities.
- Serology interpretation is critical: HBsAg indicates active infection; anti-HBs indicates immunity; anti-HBc IgM suggests acute hepatitis; anti-HBc IgG indicates past or current exposure; isolated anti-HBc may reflect resolved infection with waned anti-HBs, occult HBV, or false positive — always check HBV DNA.
- HBeAg/anti-HBe and HBV DNA guide replication status and treatment decisions; HBsAg quantification assists with phase confirmation and predicts HBsAg loss.
- Four phases of chronic infection: Immune-tolerant (HBeAg+, high DNA, normal ALT), immune-active HBeAg-positive (high DNA, elevated ALT), inactive carrier (HBeAg−, anti-HBe+, low DNA, normal ALT), and HBeAg-negative chronic hepatitis (precore/BCP mutant, fluctuating ALT).
- Treatment indicated when: ALT persistently elevated with HBV DNA >20,000 IU/mL (HBeAg+) or >2,000 IU/mL (HBeAg−), significant fibrosis (≥F2) on transient elastography or biopsy, or any cirrhosis with detectable HBV DNA.
- First-line oral antivirals: Entecavir 0.5 mg daily or tenofovir; tenofovir alafenamide (TAF) 25 mg preferred over tenofovir disoproxil (TDF) in patients with renal impairment or osteoporosis risk.
- Pegylated interferon alfa-2a offers a finite treatment course (48 weeks) in selected patients (young, high ALT, low DNA, genotype A or B) but has significant side-effect profile.
- HCC surveillance mandatory: 6-monthly abdominal ultrasound ± AFP for all patients with cirrhosis, family history of HCC, Africans aged >20 years, Asian males >40 years, and Asian females >50 years.
- Reactivation risk: B-cell depleting agents (rituximab — highest risk), anthracycline-based chemotherapy, anti-TNF therapy, and moderate-to-high dose corticosteroids can precipitate HBV reactivation; prophylactic antiviral therapy (entecavir or tenofovir) is essential regardless of HBsAg status or isolated anti-HBc.
- Aboriginal and Torres Strait Islander peoples have higher prevalence, earlier acquisition (often perinatal/childhood), and higher HCC rates — enhanced screening, culturally safe care, and government-funded antiviral access are essential.
- All antivirals are PBS-listed in Australia; entecavir and tenofovir are General Benefit; treatment is generally long-term with periodic reassessment for finite therapy cessation in selected patients.
🎧 Audio Brief
Serology Interpretation
Interpretation of hepatitis B serological markers is foundational to diagnosis, phase classification, treatment decisions, and assessment of immunity. A systematic approach combining HBsAg, anti-HBs, anti-HBc (IgM and IgG), HBeAg, anti-HBe, HBV DNA, and HBsAg quantification provides the complete clinical picture.
Core Serological Markers
| Marker | Significance | Clinical Interpretation |
|---|---|---|
| HBsAg | Surface antigen — indicates active infection | Present in both acute and chronic hepatitis B. Persistence ≥6 months defines chronic infection. Quantitative HBsAg (qHBsAg) aids phase prediction and monitoring. |
| Anti-HBs | Protective antibody — indicates immunity | ≥10 mIU/mL = protective level post-vaccination or resolved infection. Levels may wane over time; memory immunity generally persists despite serological loss. |
| Anti-HBc IgM | Marker of acute or recent infection | Present in acute hepatitis B (typically high titre). Low-level positive may occur during HBeAg-negative chronic hepatitis flare — correlation with clinical context essential. |
| Anti-HBc IgG | Marker of past or current HBV exposure | Persists lifelong. Present in resolved infection, chronic infection, and occult HBV. Does not distinguish between active and resolved — must interpret with HBsAg. |
| HBeAg | Marker of active viral replication | Positive in immune-tolerant and immune-active phases. Seroconversion to anti-HBe marks transition to inactive carrier in most patients. |
| Anti-HBe | Antibody to e antigen | Usually indicates reduced replication. However, HBeAg-negative chronic hepatitis (precore/BCP mutants) presents with anti-HBe positivity and ongoing disease activity. |
Viral Markers and Quantitative Assays
| Test | Role | Key Thresholds |
|---|---|---|
| HBV DNA (viral load) | Quantifies replication activity; critical for phase classification and treatment indication | HBeAg+ chronic: treat if >20,000 IU/mL. HBeAg− chronic: treat if >2,000 IU/mL. Inactive carrier: typically <2,000 IU/mL. Undetectable = good treatment response. |
| HBsAg quantification (qHBsAg) | Aids phase confirmation; predicts probability of HBsAg loss; guides treatment cessation decisions | qHBsAg <100 IU/mL associated with higher rates of HBsAg loss. >1,000 IU/mL suggests active immune-active phase in HBeAg− patients. |
Interpreting Common Serological Patterns
| Pattern | Interpretation | Action |
|---|---|---|
| HBsAg+, HBeAg+, anti-HBc IgG+, high DNA | Chronic HBV — likely immune-tolerant or immune-active phase | Check ALT, HBV DNA level, assess fibrosis; classify phase |
| HBsAg−, anti-HBs+, anti-HBc IgG+ | Resolved (past) infection with immunity | No treatment; document for transplant/immunosuppression screening |
| HBsAg−, anti-HBs−, anti-HBc IgG+ | Isolated anti-HBc | Check HBV DNA — may represent occult HBV infection, resolved infection with waned anti-HBs, or false positive. If HBV DNA undetectable: vaccinate if immunosuppression anticipated; monitor if high-risk immunosuppression planned. |
| HBsAg−, anti-HBs+, anti-HBc− | Vaccine-induced immunity (never infected) | No further action required |
| HBsAg−, anti-HBs−, anti-HBc− | Susceptible — no evidence of infection or immunity | Offer vaccination per Australian National Immunisation Program |
Laboratory Availability in Australia
Phases of Chronic Infection
Chronic hepatitis B (CHB) evolves through recognisable immunological phases. Accurate phase classification — combining HBeAg status, HBV DNA level, ALT, and hepatic fibrosis assessment — directly determines whether antiviral treatment is indicated. Not all patients progress sequentially through every phase, and phases may overlap or change with host immune status.
Phase 1 — Immune-Tolerant (HBeAg-Positive Chronic Infection)
HBV DNA: Very high (typically >10⁷ IU/mL)
ALT: Persistently normal
Fibrosis: Minimal to none (F0–F1)
HBsAg: High levels (>10,000 IU/mL)
Phase 2 — Immune-Active, HBeAg-Positive (HBeAg-Positive Chronic Hepatitis)
HBV DNA: High (typically 10⁵–10⁷ IU/mL, often >20,000)
ALT: Elevated (fluctuating or persistently raised)
Fibrosis: Progressive — may be F1–F4
HBsAg: >1,000 IU/mL
Phase 3 — Inactive Carrier (HBeAg-Negative Chronic Infection)
HBV DNA: Low or undetectable (<2,000 IU/mL)
ALT: Persistently normal
Fibrosis: Stable or regressing
HBsAg: Variable, often <1,000 IU/mL
Phase 4 — HBeAg-Negative Chronic Hepatitis (Precore/BCP Variant)
HBV DNA: Detectable, fluctuating (typically 10³–10⁷ IU/mL, often >2,000)
ALT: Fluctuating — may be intermittently normal (flares and remissions)
Fibrosis: Progressive — often advanced at presentation
Mechanism: Precore (G1896A) or basal core promoter (BCP) mutations prevent HBeAg synthesis
Phase 5 — Resolved Hepatitis B (HBsAg Loss)
HBV DNA: Undetectable (occult HBV: cccDNA persists in hepatocytes)
ALT: Normal
Phase Assessment Algorithm
Treatment Indications & Agents
Antiviral therapy for chronic hepatitis B aims to suppress HBV replication, reduce hepatic inflammation and fibrosis progression, prevent cirrhosis decompensation, and reduce hepatocellular carcinoma (HCC) risk. Treatment is usually long-term; finite therapy is possible in selected patients after prolonged consolidation.
Treatment Indications
- HBeAg-positive chronic hepatitis: ALT > ULN and HBV DNA >20,000 IU/mL
- HBeAg-negative chronic hepatitis: ALT > ULN and HBV DNA >2,000 IU/mL
- Significant fibrosis (≥F2 on transient elastography or liver biopsy), regardless of ALT
- Cirrhosis (compensated or decompensated) with any detectable HBV DNA
- Family history of HCC or hepatocellular carcinoma
- Extrahepatic manifestations (polyarteritis nodosa, glomerulonephritis)
- Prior to or during immunosuppressive therapy (reactivation prophylaxis)
- Pregnancy: if HBV DNA >200,000 IU/mL — antenatal tenofovir from 28–32 weeks to reduce perinatal transmission
First-Line Oral Antiviral Agents
Finite-Duration Therapy — Pegylated Interferon Alfa-2a
Agents No Longer Recommended as First-Line
| Agent | Issue | Current Role |
|---|---|---|
| Lamivudine | High resistance rate (~70% at 5 years) | Not recommended for chronic HBV monotherapy; only in combination for HIV co-infection |
| Adefovir | Weak potency, nephrotoxicity, high resistance | Obsoleted by tenofovir; not recommended |
| Telbivudine | Moderate resistance, limited availability in Australia | Not PBS-listed for HBV in Australia; not recommended |
Treatment Cessation Considerations
Most patients require long-term (often indefinite) oral antiviral therapy. However, finite therapy may be considered in carefully selected patients:
- HBeAg-positive patients: After HBeAg seroconversion (HBeAg−, anti-HBe+) with undetectable HBV DNA for ≥12 months of consolidation therapy — consider cessation with close monitoring. Risk of relapse ~50%.
- HBeAg-negative patients: Cessation may be considered if HBsAg loss achieved (functional cure) or HBsAg <100 IU/mL with undetectable HBV DNA for ≥3 years — but relapse rates remain high (~50–60%).
- Cirrhosis: Do NOT stop treatment — indefinite therapy required due to high risk of hepatic decompensation upon relapse.
- Post-cessation monitoring: ALT and HBV DNA every 3 months for ≥12 months; retreat promptly if ALT flare or HBV DNA rebound detected.
Special Treatment Considerations
HCC Surveillance & Reactivation Prevention
Hepatocellular carcinoma (HCC) is the most serious long-term complication of chronic hepatitis B, even in the absence of cirrhosis. Concurrently, HBV reactivation during immunosuppressive therapy represents an acute, potentially fatal complication that is entirely preventable with appropriate prophylaxis.
HCC Surveillance Programme
Who Requires HCC Surveillance?
| Risk Group | Surveillance Criteria |
|---|---|
| All patients with cirrhosis (any aetiology including HBV) | 6-monthly ultrasound ± AFP — regardless of antiviral therapy or viral suppression |
| Family history of HCC (first-degree relative) | 6-monthly ultrasound ± AFP from age 20 or from diagnosis, whichever is later |
| African-born patients | 6-monthly ultrasound ± AFP from age 20 (higher incidence at younger age) |
| Asian-born males | 6-monthly ultrasound ± AFP from age 40 |
| Asian-born females | 6-monthly ultrasound ± AFP from age 50 |
| Aboriginal and Torres Strait Islander peoples | Lower threshold for surveillance; consider from age 40 or earlier if additional risk factors (co-infection, alcohol, diabetes) |
Surveillance Modality
- Abdominal ultrasound: Primary surveillance tool — MBS-rebated. Sensitivity ~60–80% for early-stage HCC. Perform every 6 months (not annually).
- Alpha-fetoprotein (AFP): Adjunct to ultrasound; alone has insufficient sensitivity (~60%) and specificity. Recommended combined with ultrasound.
- Multiphasic CT or MRI: Not routine surveillance; reserved for diagnostic workup of lesions detected on ultrasound (LI-RADS classification).
Australian Pathway — Abnormal Surveillance Result
HBV Reactivation During Immunosuppressive Therapy
Risk Stratification for Reactivation
• Methotrexate
• Azathioprine/6-MP
• Small molecule TKIs (e.g., imatinib)
• Anti-TNF agents (in HBsAg−/anti-HBc+ patients)
• Anti-TNF agents (in HBsAg+ patients)
• Moderate-dose corticosteroids (≥10 mg/day prednisolone ≥4 weeks)
• Tyrosine kinase inhibitors
• Other targeted therapies
• Ofatumumab, obinutuzumab (anti-CD20)
• Brentuximab vedotin
• Alemtuzumab (anti-CD52)
• High-dose corticosteroids (≥20 mg/day ≥4 weeks)
• Haematopoietic stem cell transplant
Prophylactic Antiviral Agents for Reactivation Prevention
Co-Infection Considerations
| Co-Infection | Key Management Point |
|---|---|
| HBV + HIV | Use tenofovir (TDF or TAF) + lamivudine or emtricitabine as part of antiretroviral regimen to cover both. Do not use entecavir as sole HBV-active agent in HIV co-infection (risk of HIV resistance). Coordinate with HIV specialist. |
| HBV + HCV | Direct-acting antiviral (DAA) therapy for HCV can trigger HBV reactivation. Screen HBV serology before DAAs. If HBsAg+ → start prophylactic entecavir/tenofovir before DAA and continue 12 weeks post-DAA. If isolated anti-HBc → monitor ALT and HBV DNA during/after DAA. |
| HBV + HDV | HDV co-infection (present in ~5% of HBsAg+ patients globally) causes the most aggressive form of chronic viral hepatitis. Screen all HBsAg+ patients with anti-HDV. Pegylated interferon is the only effective treatment for HDV (48+ weeks). Bulevirtide (Hepcludex®) approved in Europe but not yet PBS-listed in Australia. |
Aboriginal and Torres Strait Islander Health
Monitoring
Ongoing monitoring of patients with chronic hepatitis B serves dual purposes: assessing response to antiviral therapy and detecting disease progression, fibrosis evolution, or HCC development. Monitoring schedules vary by phase and treatment status.
Monitoring Schedule
| Clinical Scenario | Tests | Frequency |
|---|---|---|
| On oral antiviral therapy | ALT, HBV DNA, eGFR, phosphate (if on TDF) | Every 3–6 months; HBV DNA at 24 and 48 weeks to confirm virological response, then every 6 months |
| Inactive carrier (confirmed) | ALT, HBsAg quantitative (if available) | ALT every 6 months for first 2 years, then annually. HBsAg quantitative annually if accessible. |
| Immune-tolerant phase | ALT, HBV DNA, HBeAg | Every 6 months; consider fibrosis assessment if age >30 or duration >20 years |
| Treatment-naïve — phase unclear | ALT, HBV DNA, HBeAg/anti-HBe, fibrosis assessment | Every 3–6 months until phase classification confirmed |
| Post-treatment cessation | ALT, HBV DNA | Every 3 months for ≥12 months; retreat promptly if ALT flare or DNA rebound |
| On TDF long-term | eGFR, serum phosphate, urine protein/creatinine ratio, bone density (DEXA if risk factors) | Annually; more frequently if eGFR declining or risk factors present |
Defining Treatment Response
- Virological response: HBV DNA undetectable (<20 IU/mL) — primary goal of oral antiviral therapy
- Biochemical response: ALT normalisation — expected within 3–6 months of effective viral suppression
- Serological response: HBeAg seroconversion (HBeAg+/anti-HBe− → HBeAg−/anti-HBe+) or HBsAg loss/seroconversion — long-term goals
- Histological response: Fibrosis regression on serial elastography or biopsy — encouraging evidence with long-term viral suppression
Treatment Failure and Resistance
With entecavir or tenofovir as first-line agents, virological breakthrough (confirmed rise in HBV DNA >1 log₁₀ above nadir on therapy) is uncommon in treatment-naïve patients. If virological breakthrough occurs:
- First confirm adherence — non-adherence is the most common cause of apparent treatment failure
- If adherent: check for resistance (genotypic testing available through reference laboratories)
- Entecavir resistance: switch to tenofovir (TDF or TAF)
- Tenofovir resistance: extremely rare — reassess adherence; consider specialist referral
- Refer to hepatologist/gastroenterologist for complex resistance management
📚 References
- 1. World Health Organization. Guidelines for the prevention, care and treatment of persons with chronic hepatitis B infection. Geneva: WHO; 2015 (updated March 2024).
- 2. European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol. 2017;67(2):370–398.
- 3. Terrault NA, Lok ASF, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology. 2018;67(4):1560–1599.
- 4. Sarin SK, Kumar M, Lau GK, et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: a 2015 update. Hepatol Int. 2016;10(1):1–98.
- 5. Australian Institute of Health and Welfare. Chronic hepatitis B infection in Australia. Cat. no. PHE 260. Canberra: AIHW; 2023.
- 6. The Kirby Institute. HIV, viral hepatitis and sexually transmissible infections in Australia: Annual surveillance report 2023. Sydney: UNSW; 2023.
- 7. Australian Government Department of Health and Aged Care. National Hepatitis B Strategy 2023–2030. Canberra: Commonwealth of Australia; 2023.
- 8. Reddy KR, Beavers KL, Hammond SP, et al. American Gastroenterological Association Institute guideline on the prevention and treatment of hepatitis B virus reactivation during immunosuppressive drug therapy. Gastroenterology. 2015;148(1):215–219.
- 9. Revill PA, Chisari FV, Block JM, et al. A global scientific strategy to cure hepatitis B. Lancet Gastroenterol Hepatol. 2019;4(7):545–558.
- 10. Visvanathan K, Dusheiko G, Giles M, et al. Managing HBV in pregnancy. Prevention, prophylaxis, treatment and follow-up: position paper produced by Australian, UK and New Zealand key opinion leaders. Gut. 2016;65(2):340–350.
- 11. National Health and Medical Research Council. Australian Immunisation Handbook. Canberra: Australian Government Department of Health; 2022 (updated online).