📋 Key Information Summary
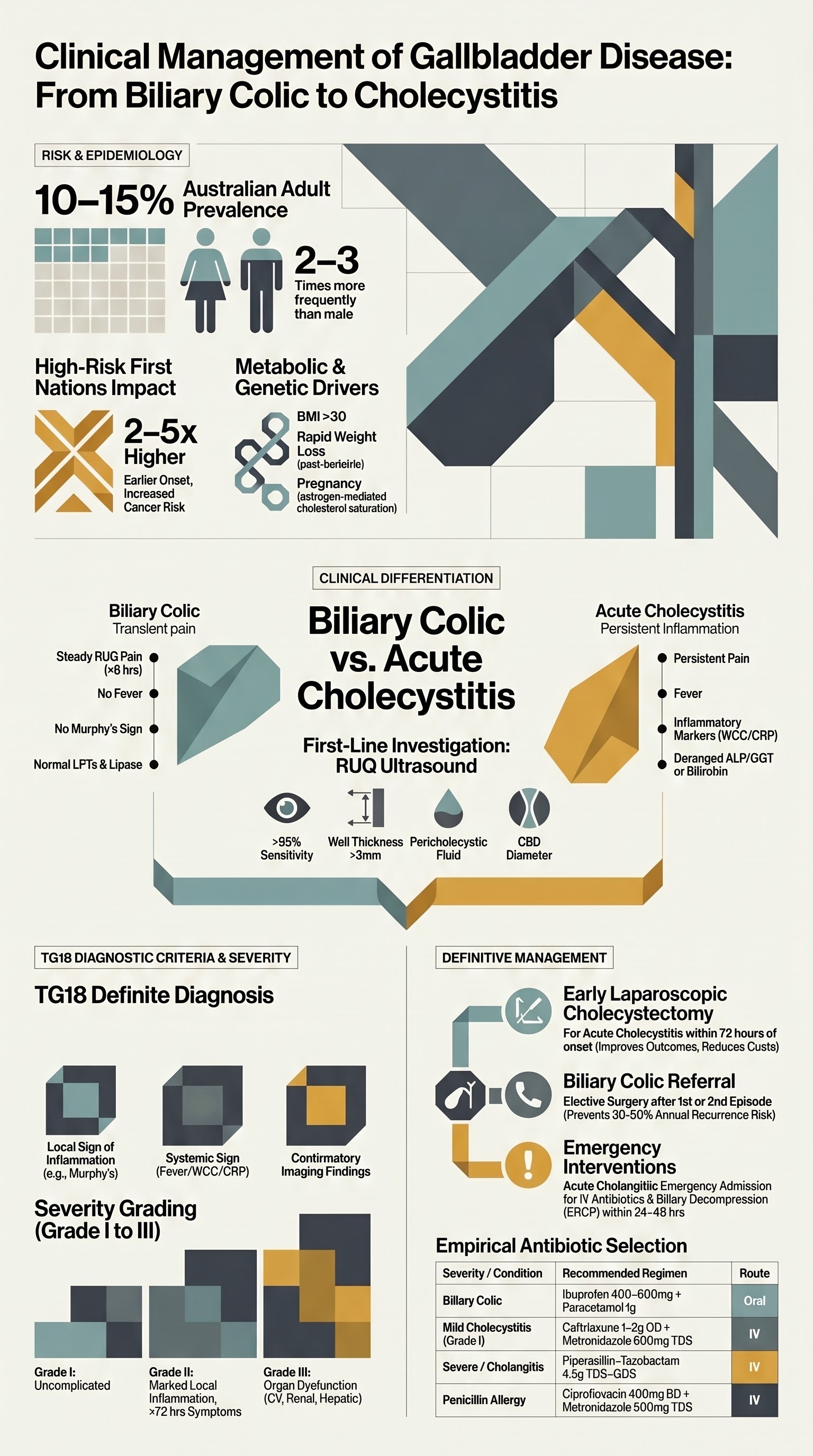
- Gallstone disease affects approximately 10–15% of Australian adults; prevalence is higher in women, older adults, people with obesity, and Aboriginal and Torres Strait Islander populations.
- Biliary colic presents as episodic, steady RUQ or epigastric pain lasting 30 minutes to several hours, often triggered by fatty meals, radiating to the right scapula or back; resolves spontaneously without residual tenderness.
- Between attacks, clinical examination and liver biochemistry are typically normal — if fever, marked leukocytosis, or persistently deranged LFTs are present, consider acute cholecystitis or cholangitis rather than simple biliary colic.
- Transabdominal RUQ ultrasound is the first-line investigation with sensitivity >95% for gallstones; it identifies stone size, gallbladder wall thickness, pericholecystic fluid, and common bile duct (CBD) diameter.
- Liver function tests (ALP, GGT, ALT, bilirubin) and serum lipase/amylase should be performed at presentation to exclude choledocholithiasis and acute pancreatitis.
- Acute cholecystitis is distinguished from biliary colic by persistent pain >4–6 hours, positive Murphy's sign, fever, and inflammatory markers; the Tokyo Guidelines (TG18) provide diagnostic criteria.
- Definitive management of symptomatic gallstones is laparoscopic cholecystectomy, ideally performed within the same admission for acute cholecystitis (early cholecystectomy within 72 hours).
- Expectant management is appropriate for asymptomatic gallstones discovered incidentally; however, patients with biliary colic should be counselled regarding elective cholecystectomy to prevent complications.
- Ursodeoxycholic acid (UDCA) is not recommended as primary treatment for symptomatic cholesterol gallstones in Australian guidelines but may be used for gallstone prophylaxis during rapid weight loss or in patients unfit for surgery.
- Acute cholangitis requires urgent IV antibiotics (e.g., piperacillin–tazobactam per eTG Antibiotic guidelines) and biliary decompression (ERCP) within 24–48 hours.
- Aboriginal and Torres Strait Islander Australians have significantly higher rates of gallstone disease and gallbladder cancer; culturally safe care, earlier referral, and community-based screening are essential.
- Post-cholecystectomy patients should be counselled regarding dietary modification and the risk of post-cholecystectomy syndrome (bile salt diarrhoea, persistent pain).
Introduction & Australian Epidemiology
Gallbladder disease encompasses a spectrum of conditions ranging from asymptomatic gallstones (cholelithiasis) to symptomatic biliary colic, acute and chronic cholecystitis, choledocholithiasis, cholangitis, and gallstone pancreatitis. Gallstones are the most common biliary pathology and represent one of the most frequent reasons for elective and emergency surgical admission in Australia.
In Australia, gallstone disease is estimated to affect 10–15% of the adult population. The prevalence increases with age, female sex (female-to-male ratio approximately 2–3:1), obesity (BMI >30 kg/m²), rapid weight loss, pregnancy, diabetes mellitus, and certain ethnic backgrounds. Gallstone-related admissions account for over 60,000 hospital separations annually, with laparoscopic cholecystectomy being one of the most commonly performed general surgical procedures nationally.
Aboriginal and Torres Strait Islander Australians experience gallstone disease at rates 2–5 times higher than the non-Indigenous population, with earlier age of onset and higher rates of gallbladder cancer. The AIHW reports that biliary disease is among the top 10 reasons for hospitalisation in First Nations Australians, particularly in remote and very remote communities.
| Risk Factor | Mechanism | Population Impact |
|---|---|---|
| Female sex | Oestrogen increases biliary cholesterol secretion; progesterone reduces gallbladder motility | F:M ratio 2–3:1 |
| Obesity (BMI >30) | Increased hepatic cholesterol secretion and supersaturated bile | Prevalence up to 20–30% |
| Rapid weight loss | Gallbladder stasis and cholesterol crystal precipitation | Up to 25% within 3–6 months of bariatric surgery |
| Pregnancy | Oestrogen effect + gallbladder hypomotility | 5–12% prevalence |
| First Nations heritage | Genetic predisposition (p.C456Y variant in hepatic phospholipid transporter), high prevalence of metabolic syndrome | 2–5× higher prevalence than non-Indigenous Australians |
| Haemolytic disorders | Pigment stone formation (increased unconjugated bilirubin) | Sickle cell disease, hereditary spherocytosis, thalassaemia |
| Increasing age | Cumulative cholesterol saturation and gallbladder dysmotility | Prevalence >20% over age 60 |
| Diabetes mellitus | Autonomic neuropathy → gallbladder dysmotility; associated obesity | 1.5–2× increased risk |
Typical Biliary Colic
Biliary colic is the cardinal symptom of uncomplicated gallstone disease. The term "colic" is a misnomer — the pain is typically steady (not colicky) and results from transient cystic duct obstruction by a gallstone, producing gallbladder distension. Understanding the characteristic presentation is critical for distinguishing biliary colic from more serious complications such as acute cholecystitis, cholangitis, and gallstone pancreatitis.
Clinical Features of Biliary Colic
- Pain character: Sudden-onset, steady (not colicky), intense visceral pain in the RUQ or epigastrium; the patient is typically restless and unable to find a comfortable position.
- Timing: Often begins 30–60 minutes after a fatty meal (e.g., fried foods, full-cream dairy); may also occur nocturnally (gallbladder stasis during fasting).
- Duration: Typically 30 minutes to 4–6 hours; if pain persists beyond 6 hours, suspect acute cholecystitis or other complications.
- Radiation: Classic radiation to the right shoulder tip (via phrenic nerve irritation) or interscapular region (referred pain via T7–T10 dermatomes).
- Associated symptoms: Nausea, vomiting, bloating; no fever, no jaundice.
- Resolution: Spontaneous resolution as the stone disimpacts from the cystic duct; between attacks the patient is entirely well with a normal examination.
- Examination between attacks: Normal — no RUQ tenderness, no Murphy's sign, no fever, no jaundice.
Differential Diagnosis
| Condition | Key Distinguishing Features | Investigation |
|---|---|---|
| Acute cholecystitis | Persistent pain >6 h, fever, positive Murphy's sign, raised WCC/CRP | RUQ USS, inflammatory markers |
| Choledocholithiasis | Obstructive jaundice, pale stools, dark urine, raised ALP/GGT/bilirubin | RUQ USS (dilated CBD >6 mm), MRCP |
| Acute cholangitis | Charcot's triad (fever, RUQ pain, jaundice); ± Reynold's pentad (add hypotension, confusion) | Blood cultures, LFTs, RUQ USS, urgent CT/MRCP |
| Gallstone pancreatitis | Severe epigastric pain radiating to back, vomiting; markedly elevated lipase (>3× ULN) | Serum lipase, CT abdomen if diagnostic uncertainty |
| Peptic ulcer disease | Epigastric burning, relationship to meals (relieved by food in duodenal ulcer), NSAID/H. pylori association | Gastroscopy, H. pylori testing |
| Acute coronary syndrome | Substernal chest pain, exertional, diaphoresis, dyspnoea; cardiovascular risk factors | ECG, troponin |
| Fitz-Hugh-Curtis syndrome | RUQ pain in setting of PID/peritonitis; sexually active young women | STI screen, pelvic USS |
| Functional dyspepsia | Chronic epigastric discomfort, bloating, early satiety; normal investigations | Diagnosis of exclusion; gastroscopy if alarm features |
Natural History
Approximately 70–80% of patients with a single episode of biliary colic will have recurrent symptoms. The natural history of untreated symptomatic gallstones is progression to complications: approximately 1–2% per year develop acute cholecystitis, 0.5–1% develop choledocholithiasis, and 0.1–0.5% develop gallstone pancreatitis. Early elective cholecystectomy is therefore recommended after the first or second confirmed episode of biliary colic to prevent complications and repeated emergency presentations.
Initial Workup
The initial workup for suspected gallbladder disease is guided by the clinical presentation — asymptomatic incidental gallstones, suspected biliary colic, or possible complicated gallstone disease (cholecystitis, cholangitis, pancreatitis). The goals of investigation are to confirm gallstones, assess for complications, and exclude alternative diagnoses.
First-Line Investigations
Second-Line and Specialist Investigations
Excluding Acute Cholecystitis and Cholangitis
The following findings on initial workup should prompt consideration of complicated gallstone disease rather than simple biliary colic:
- Acute cholecystitis indicators: Pain >6 hours, fever (≥37.8°C), positive Murphy's sign on examination, gallbladder wall thickening (>3 mm) or pericholecystic fluid on ultrasound, leukocytosis (WCC >11 × 10⁹/L), elevated CRP.
- Acute cholangitis indicators: Charcot's triad (RUQ pain + fever + jaundice) — sensitivity approximately 50–70%; Reynold's pentad adds hypotension and altered mental status indicating suppurative cholangitis. Deranged LFTs with obstructive pattern (elevated ALP, GGT, conjugated bilirubin). Requires urgent blood cultures and IV antibiotics.
- Gallstone pancreatitis indicators: Severe epigastric pain radiating to the back, nausea/vomiting, lipase >3× ULN. Can be distinguished from biliary colic by the severity and location of pain, markedly elevated lipase, and the absence of spontaneous resolution within 4–6 hours.
Pathophysiology
Gallstones form when the concentration of cholesterol, bile salts, or bilirubin in bile becomes supersaturated, leading to crystal nucleation and stone growth within the gallbladder. The three main types of gallstones are:
- Cholesterol stones (80–85%): Formed from supersaturated bile with excess cholesterol relative to bile salts and lecithin. Associated with obesity, high-fat diets, female sex, pregnancy, and certain medications (e.g., oral contraceptives, fibrates).
- Pigment stones (15–20%): Composed of calcium bilirubinate. Black pigment stones are associated with haemolytic disorders (sickle cell disease, hereditary spherocytosis, thalassaemia), cirrhosis, and Gilbert syndrome. Brown pigment stones are associated with biliary infection (Clonorchis, Ascaris) and are more common in East Asian populations.
- Mixed stones: Combination of cholesterol and calcium components; most common in clinical practice.
Biliary colic occurs when a gallstone transiently impacts in the cystic duct, causing gallbladder wall distension and visceral pain mediated by C-fibre afferents. The stone typically disimpacts spontaneously (within hours) as gallbladder contraction ceases, allowing the stone to fall back into the gallbladder lumen or pass into the CBD.
Acute cholecystitis develops when persistent cystic duct obstruction (beyond 4–6 hours) leads to gallbladder wall ischaemia, inflammation, bacterial infection (50–75% of cases), and potentially gangrene or perforation. Common organisms include Escherichia coli, Klebsiella, Enterococcus, and Bacteroides species.
Choledocholithiasis occurs when stones migrate from the gallbladder through the cystic duct into the common bile duct, causing mechanical obstruction. This can lead to obstructive jaundice, cholangitis (if bacterial infection ascends), or gallstone pancreatitis (if stones impact at the ampulla of Vater, obstructing the pancreatic duct).
Clinical Presentation & Diagnostic Criteria
Tokyo Guidelines (TG18) — Diagnostic Criteria for Acute Cholecystitis
The Tokyo Guidelines provide internationally validated diagnostic criteria for acute cholecystitis, which are widely used in Australian practice:
| Criterion | Finding |
|---|---|
| A. Local signs of inflammation | Murphy's sign, RUQ mass, pain, or tenderness |
| B. Systemic signs of inflammation | Fever (>37.8°C), elevated CRP (>3 mg/dL), elevated WCC (>11 × 10⁹/L) |
| C. Imaging findings | Characteristic findings of acute cholecystitis on ultrasound, CT, MRI, or HIDA scan (gallbladder wall thickening, pericholecystic fluid, gallbladder distension, sonographic Murphy's sign) |
Suspected diagnosis: One item in A + one item in B.
Definite diagnosis: One item in A + one item in B + C.
Severity Grading (TG18)
Charcot's Triad and Reynold's Pentad — Acute Cholangitis
- RUQ pain
- Fever / rigors
- Jaundice
Sensitivity approximately 50–70% for acute cholangitis.
- Charcot's triad +
- Hypotension
- Altered mental status
Indicates suppurative (ascending) cholangitis — life-threatening emergency.
Investigations — Detailed
Interpreting Laboratory Results in Gallstone Disease
| Condition | LFTs | Lipase | FBC / CRP | Blood Cultures |
|---|---|---|---|---|
| Biliary colic | Normal | Normal | Normal | Not indicated |
| Acute cholecystitis | Mildly elevated ALT/ALP in 30–50% | Normal or mildly elevated | Leukocytosis, elevated CRP | If severe/febrile |
| Choledocholithiasis | Obstructive pattern: ↑↑ALP, ↑↑GGT, ↑bilirubin, ↑ALT | Normal or mildly elevated | May be normal | Not indicated initially |
| Acute cholangitis | Obstructive pattern: ↑↑ALP, ↑↑GGT, ↑↑bilirubin | Normal or mildly elevated | ↑↑WCC, ↑↑CRP | Mandatory (x2 sets before antibiotics) |
| Gallstone pancreatitis | ↑ALT >150 IU/L (marker of biliary aetiology), ↑bilirubin | ↑↑↑ >3× ULN | Leukocytosis, ↑CRP | Not indicated initially |
Imaging — When to Order What
Australian MBS Item Numbers — Key Investigations
| Investigation | MBS Item | Notes |
|---|---|---|
| RUQ Ultrasound | 55038 | Abdominal ultrasound; widely available including most regional centres |
| CT Abdomen ± Pelvis | 56104 / 56108 | With or without IV contrast |
| MRI Abdomen | 63540 | Including MRCP sequences; may require specialist request |
| LFTs | 66518 | Liver function panel |
| Lipase / Amylase | 66554 | Serum lipase preferred over amylase |
| HIDA Scan | 61325 | Nuclear medicine; limited availability in regional areas |
| Laparoscopic cholecystectomy | 30443 | With intraoperative cholangiography: 30445 |
| ERCP | 30470 / 30473 | Diagnostic / Therapeutic (sphincterotomy ± stone extraction) |
Risk Stratification & Severity Scoring
Risk of Complications in Untreated Gallstones
| Complication | Annual Risk | Risk Factors |
|---|---|---|
| Recurrent biliary colic | ~30–50% per year after first episode | Prior episode, stone size 2–5 mm or >10 mm |
| Acute cholecystitis | 1–2% | Impacted stone in cystic duct, stone >5 mm |
| Choledocholithiasis | 0.5–1% | Small stones (<5 mm), dilated CBD |
| Gallstone pancreatitis | 0.1–0.5% | Small stones, multiple stones, gallbladder sludge |
| Acute cholangitis | Rare (secondary to choledocholithiasis) | CBD stones, biliary stent, prior ERCP |
| Gallbladder cancer | 0.01–0.03% | Porcelain gallbladder, gallstones >3 cm, polyps >10 mm |
When to Recommend Elective Cholecystectomy vs Watchful Waiting
Empirical & Acute Management
Biliary Colic — Acute Symptom Management
Acute management of biliary colic in the primary care or emergency setting focuses on symptom relief with analgesia and antiemetics, followed by definitive management (cholecystectomy) once the acute episode resolves.
Acute Cholecystitis — Empirical Antibiotics
Antibiotics are indicated for acute cholecystitis and should be initiated after blood cultures are obtained. Empirical coverage targets enteric Gram-negatives (E. coli, Klebsiella) and anaerobes (Bacteroides). The following regimens align with eTG Antibiotic guidelines:
Directed & Definitive Therapy
Laparoscopic Cholecystectomy — The Definitive Treatment
Laparoscopic cholecystectomy is the gold-standard treatment for symptomatic gallstones and is one of the most commonly performed procedures in Australia, with approximately 55,000–60,000 performed annually. The procedure is funded by Medicare (MBS Item 30443) and is performed across metropolitan and regional hospitals.
CBD Stone Management
- Preoperative ERCP: For confirmed CBD stones, ERCP with sphincterotomy and stone extraction is performed preoperatively, followed by laparoscopic cholecystectomy.
- Intraoperative CBD exploration: Some centres perform laparoscopic CBD exploration at the time of cholecystectomy, particularly for stones discovered on intraoperative cholangiogram. This avoids the need for a separate ERCP.
- Postoperative ERCP: If CBD stones are identified postoperatively (e.g., on postoperative LFTs), ERCP is performed as a secondary procedure.
Pharmacological Alternatives (Selected Patients)
Monitoring
Postoperative Monitoring
- Day-surgery / overnight stay: Most uncomplicated laparoscopic cholecystectomies are performed as day surgery or with an overnight stay. Patients should be observed for 4–6 hours post-procedure for pain control, nausea, and early complications.
- Postoperative LFTs: Check LFTs at 4–6 weeks post-cholecystectomy to ensure normalisation if preoperative LFTs were deranged. Persistent elevation may indicate retained CBD stones.
- Follow-up: GP review at 2–4 weeks post-discharge. Assess for resolution of preoperative symptoms, wound healing, and dietary tolerance.
Post-Cholecystectomy Syndrome
Up to 10–40% of patients report some GI symptoms after cholecystectomy, collectively termed post-cholecystectomy syndrome:
- Bile salt diarrhoea: Occurs in 5–10% due to continuous bile flow into the duodenum. Managed with cholestyramine (Questran®) 4 g PO OD–BD before meals. PBS General Benefit.
- Persistent or recurrent pain: If biliary-type pain persists post-cholecystectomy, consider retained CBD stones, sphincter of Oddi dysfunction, or functional GI disorders. Further workup may include MRCP, EUS, or ERCP with manometry.
- Dietary advice: Advise a gradual return to normal diet. Some patients tolerate small, frequent, low-fat meals better in the initial weeks post-cholecystectomy. There is no requirement for long-term fat restriction.
Monitoring Patients on Expectant Management
- Patients with asymptomatic gallstones do not require routine ultrasound surveillance.
- Advise patients to present if they develop RUQ/epigastric pain, fever, jaundice, or unexplained GI symptoms.
- Annual clinical review is reasonable for patients with known gallstones, with attention to weight management and cardiovascular risk factors (metabolic syndrome overlap).
- Gallbladder polyps <10 mm — repeat ultrasound at 6 months, then annually; refer for cholecystectomy if growth >2 mm per year or size >10 mm.
Special Populations
Pregnancy
Paediatrics
Elderly (≥65 years)
Renal Impairment
Hepatic Impairment
Immunocompromised
Referral & Surgical Consideration
Indications for Surgical / Gastroenterology Referral
Timely referral is critical to prevent complications and reduce emergency presentations. The following indications warrant specialist referral:
Referral Pathways in Australia
| Scenario | Referral To | Urgency | Considerations |
|---|---|---|---|
| Symptomatic gallstones (elective) | General Surgeon (public or private) | Semi-urgent (Category 2: within 90 days) | Public hospital wait times may be 3–12 months; private health insurance enables earlier surgery |
| Acute cholecystitis | Emergency Department → Acute Surgical Unit | Emergency (within 24–72 h for early cholecystectomy) | All metropolitan and most regional hospitals have surgical capability |
| CBD stones / cholangitis | Gastroenterologist / Interventional endoscopist | Urgent (ERCP within 24–48 h for cholangitis) | ERCP services available at most tertiary and many regional hospitals; may require interhospital transfer from remote areas |
| Gallstone pancreatitis | Acute medical/surgical unit ± gastroenterology | Emergency | Cholecystectomy during same admission for mild pancreatitis; deferred for severe pancreatitis |
| Suspected gallbladder cancer | Hepatobiliary surgical oncologist | Urgent (within 2 weeks) | Refer to specialised HPB unit; staging CT required |
Surgical Risk Assessment
Laparoscopic cholecystectomy is generally safe with a mortality rate of <0.1% in low-risk patients. Key surgical risks include:
- Bile duct injury: 0.3–0.5% (most feared complication). Risk increased in acute cholecystitis, male sex, obesity, and aberrant biliary anatomy. Routine or selective intraoperative cholangiography may reduce risk.
- Bile leak: 0.2–1% from cystic duct stump or accessory ducts (ducts of Luschka).
- Conversion to open: 5–10% in acute cholecystitis; <3% in elective surgery.
- Port-site hernia: 1–2% (reduced with fascial closure of port sites ≥10 mm).
- General surgical risks: Bleeding, infection, DVT/PE, anaesthetic complications, retained CBD stones.
Aboriginal and Torres Strait Islander Health Considerations
Gallbladder disease represents a significant health disparity for Aboriginal and Torres Strait Islander Australians. First Nations Australians experience gallstone disease at rates 2–5 times higher than non-Indigenous Australians, with earlier age of onset (often in the 20s and 30s), higher rates of complicated gallstone disease, and a substantially elevated incidence of gallbladder cancer. Understanding and addressing these disparities is essential for equitable clinical care.
Key Disparities
- Prevalence: Gallstone disease is one of the top reasons for hospitalisation among First Nations Australians. Community-based studies in remote Northern Territory communities report gallstone prevalence of 25–50% in adults over 30.
- Genetic predisposition: A missense variant in the ABCB4 gene (p.C456Y), encoding the hepatic phospholipid transporter MDR3, is found at high frequency in Aboriginal Australians and predisposes to low-phospholipid-associated cholelithiasis (LPAC syndrome) with early-onset, recurrent, and complicated gallstone disease.
- Gallbladder cancer: Incidence rates of gallbladder cancer in First Nations Australians are 3–5 times higher than in non-Indigenous Australians. Late diagnosis and limited access to specialist HPB surgery contribute to poorer outcomes.
Quick Reference — Empirical Regimens
📚 References
- 1. Yokoe M, Hata J, Takada T, et al. Tokyo Guidelines 2018: diagnostic criteria and severity grading of acute cholecystitis (with videos). J Hepatobiliary Pancreat Sci. 2018;25(1):41–54.
- 2. Gurusamy KS, Davidson BR. Surgical treatment of gallstones. Gastroenterol Clin North Am. 2010;39(2):229–244.
- 3. National Institute for Health and Care Excellence (NICE). Gallstone disease: diagnosis and management. Clinical Guideline CG188. London: NICE; 2014 (updated 2023).
- 4. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework: Summary report. Canberra: AIHW; 2023.
- 5. Gutt C, Schläfer J, Lammert F. The treatment of gallstone disease. Dtsch Arztebl Int. 2020;117(9):148–158.
- 6. European Association for the Study of the Liver (EASL). EASL Clinical Practice Guidelines on the prevention, diagnosis and treatment of gallstones. J Hepatol. 2016;65(1):146–181.
- 7. Schernhammer E, Beresford SAA, Curhan GC, et al. Cholecystectomy and the risk for developing colorectal cancer and distal colorectal adenomas. Br J Cancer. 2012;107(1):177–180.
- 8. Steiner CA, Bass EB, Talamini MA, Pitt HA, Steinberg EP. Laparoscopic cholecystectomy: clinical and economic analysis. Ann Surg. 2014;219(6):694–701.
- 9. Gurusamy KS, Koti R, Fusai G, Davidson BR. Early versus delayed laparoscopic cholecystectomy for uncomplicated biliary colic. Cochrane Database Syst Rev. 2013;(6):CD007196.
- 10. Loozen CS, van Santvoort HC, van Duijvendijk P, et al. Laparoscopic cholecystectomy versus best supportive care for acute cholecystitis (CHOCOLATE): a multicentre randomised controlled trial. Lancet. 2018;391(10131):1693–1701.
- 11. Royal Australian College of General Practitioners (RACGP). Guidelines for preventive activities in general practice (Red Book). 9th ed. Melbourne: RACGP; 2018.
- 12. Harvey PR, Bhatt DL, Wasan S, et al. Gallstone disease in Aboriginal Australians: epidemiology and genetics. Aust N Z J Surg. 2019;89(5):512–518.
- 13. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.
- 14. Mayo Clinic. Gallstones — Diagnosis and treatment. Rochester, MN: Mayo Foundation for Medical Education and Research; 2024. Available at: https://www.mayoclinic.org/diseases-conditions/gallstones/diagnosis-treatment/
- 15. Miura F, Okamoto K, Takada T, et al. Tokyo Guidelines 2018: initial management of acute biliary infection and flowchart for acute cholangitis. J Hepatobiliary Pancreat Sci. 2018;25(1):31–40.