📋 Key Information Summary
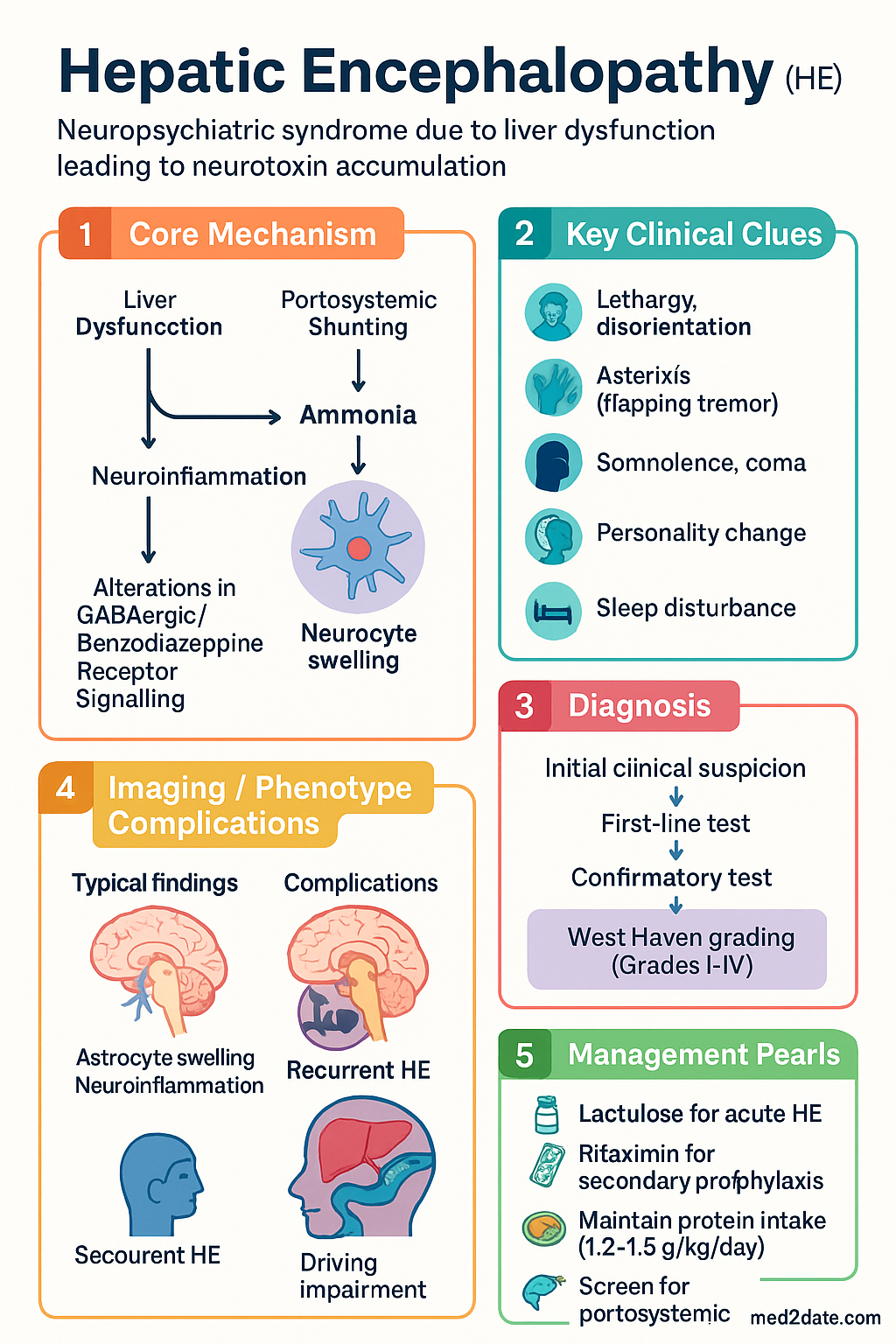
- Hepatic encephalopathy (HE) is a neuropsychiatric syndrome caused by liver dysfunction or portosystemic shunting, resulting in accumulation of neurotoxins — principally ammonia — that cross a compromised blood–brain barrier.
- West Haven grading classifies HE into covert (minimal HE + Grade I, detected only by testing) and overt (Grades II–IV, clinically apparent).
- Every new episode of overt HE mandates systematic search for a precipitant — most commonly infection (especially SBP), GI bleeding, electrolyte disturbance, constipation, and sedative use.
- First-line treatment of acute HE is lactulose (oral or rectal enema if obtunded), titrated to 2–3 soft bowel motions per day.
- Rifaximin 550 mg PO BD is added to lactulose for secondary prophylaxis after ≥1 episode of overt HE (NNT 4 to prevent one additional episode).
- Do NOT restrict protein intake — maintain 1.2–1.5 g/kg/day; protein restriction worsens sarcopenia and outcomes.
- Screen for large spontaneous portosystemic shunts in recurrent/refractory HE; consider coil embolisation or BATO.
- After TIPS, if HE is refractory despite medical therapy, consider TIPS reduction or closure.
- Refer early for liver transplant assessment if HE is refractory to combined lactulose + rifaximin ± shunt embolisation.
- Driving must cease during overt HE; the treating physician has a legal duty to notify the relevant state/territory licensing authority.
- Aboriginal and Torres Strait Islander patients experience higher cirrhosis burden; culturally safe care, AMS engagement, and addressing barriers to specialist access are essential.
🎧 Audio Brief
Precipitants & Grading
Pathophysiology
HE results from the accumulation of neurotoxins — principally ammonia (NH₃) — in the setting of impaired hepatic clearance and/or portosystemic shunting. Ammonia, generated predominantly by gut urease-producing bacteria (Enterobacteriaceae, Streptococcaceae), is normally cleared by hepatic urea-cycle conversion to urea. In cirrhosis, reduced hepatocyte mass and portosystemic collaterals allow ammonia to reach the systemic circulation and cross the blood–brain barrier. Astrocyte swelling from glutamine accumulation, neuroinflammation (TNF-α, IL-1β, IL-6), manganese deposition, and alterations in GABAergic/benzodiazepine receptor signalling collectively produce the neuropsychiatric manifestations. The gut–liver–brain axis is central, explaining why therapies targeting gut ammonia production (lactulose, rifaximin) are effective.
West Haven Grading System
The West Haven Criteria remain the standard bedside classification for HE severity:
| Classification | Grade | Clinical Features |
|---|---|---|
| Covert HE | Minimal HE | No clinical abnormality on standard exam; detected only by psychometric or neurophysiological testing (impaired attention, working memory, psychomotor speed) |
| Grade I | Lack of awareness, shortened attention span, impaired addition/subtraction, sleep disturbance, euphoria or anxiety; may be detected only by careful questioning | |
| Overt HE | Grade II | Lethargy, disorientation to time, personality change, inappropriate behaviour, asterixis (flapping tremor) |
| Grade III | Somnolence but rousable, gross disorientation, bizarre behaviour, muscular rigidity, hyperreflexia, upgoing plantars | |
| Grade IV | Coma — unresponsive to verbal or noxious stimuli; decerebrate or decorticate posturing possible |
Minimal (Covert) HE — Diagnostic Testing
Minimal HE affects 20–80% of patients with cirrhosis and is associated with impaired quality of life, increased fall risk, poor driving performance, and progression to overt HE. It is not detectable by standard neurological examination. Recommended screening tools in Australia include:
Screen with PHES or EncephalApp Stroop in all patients with cirrhosis — particularly those with driving or occupational safety concerns, prior episodes of overt HE, or TIPS.
Precipitants of Overt HE
Always search for and treat reversible precipitants before or concurrently with HE-specific therapy. More than one precipitant is present in up to 60% of episodes.
Treatment
General Principles
- Identify and treat precipitants first — HE-specific therapy alone is insufficient if an untreated precipitant persists.
- Do NOT restrict protein — malnutrition and sarcopenia are near-universal in decompensated cirrhosis and independently worsen prognosis.
- Aim for caloric intake 35 kcal/kg/day and protein 1.2–1.5 g/kg/day with small, frequent meals and a late-evening snack.
- Review and stop all non-essential sedatives, opioids, and psychoactive medications.
Pharmacotherapy — Acute Overt HE
Nutritional Management
Historical advice to restrict protein is outdated and harmful. Evidence demonstrates that protein restriction worsens sarcopenia, increases infection risk, and does not improve HE outcomes.
- Target 1.2–1.5 g/kg/day protein (adjusted body weight in obesity).
- Provide 35 kcal/kg/day total energy.
- Small, frequent meals (4–6 per day) plus a late-evening snack (complex carbohydrate-rich) to reduce overnight protein catabolism.
- Vegetable and dairy protein may be better tolerated than meat-based protein in some patients (lower ammonia generation).
- Consider dietitian referral for all hospitalised cirrhotics.
Supportive Care
- Nursing observation every 1–2 hours for Grade II–III HE; continuous monitoring in Grade IV.
- Aspiration precautions — head of bed ≥ 30°; consider NG tube for enteral lactulose if unable to swallow safely.
- Pressure area care; DVT prophylaxis with LMWH if no active bleeding.
- Minimise sedation; avoid antipsychotics (haloperidol contraindicated in hepatic disease).
Recurrent & Refractory HE
Recurrent HE is defined as ≥2 episodes of overt HE within 6 months despite treatment of precipitants. Refractory HE is persistent or rapidly recurring HE despite optimal medical therapy (lactulose + rifaximin). These patients require a systematic escalation strategy.
1. Optimise Long-Term Medical Therapy
- Lactulose — ensure ongoing adherence; titrate to 2–3 soft bowel motions/day. Review compliance (palatability is a common issue).
- Rifaximin 550 mg PO BD — continuous therapy; requires PBS Authority approval. Reduces HE recurrence by 58% (NNT = 4) based on the Bass et al. 2010 RCT.
- Confirm absence of ongoing precipitants (recurrent SBP prophylaxis with norfloxacin 400 mg daily or ciprofloxacin 500 mg daily if indicated).
2. Screen for Large Spontaneous Portosystemic Shunts
Large spontaneous portosystemic shunts (SPSS) — particularly splenorenal, gastrorenal, and paraumbilical shunts — allow ammonia-rich portal blood to bypass the liver, perpetuating HE despite adequate hepatic reserve. They are present in 25–40% of cirrhotics and are increasingly recognised as a treatable cause of recurrent/refractory HE.
- Investigation: Multiphase CT abdomen or MRI with portal venous phase; interventional radiology assessment for shunt calibre and anatomy.
- Intervention: Balloon-occluded retrograde transvenous obliteration (BATO) or coil embolisation of large SPSS.
- Evidence: Case series show 50–80% reduction in HE episodes after SPSS embolisation in selected patients. Australian tertiary centres (RPA, Austin, Alfred) perform this procedure.
- Risk: Re-bleeding of varices, procedure-related portal hypertension — requires multidisciplinary hepatology–interventional radiology discussion.
3. TIPS-Related Refractory HE
If HE develops or worsens after TIPS placement (25–50% within 3 months):
- Optimise lactulose + rifaximin as above.
- Exclude other precipitants.
- Consider TIPS reduction (using stent-graft reduction or parallel stent placement to decrease shunt diameter from 10–12 mm to 5–8 mm) — reduces portal flow diversion while maintaining some portal decompression.
- In severe cases, TIPS occlusion/closure may be necessary, but this risks recurrent variceal bleeding or refractory ascites — transplant referral should accompany this decision.
4. Liver Transplant Referral
Refractory HE is an indication for liver transplant evaluation. Key points:
- Refer early — before irreversible neurocognitive damage (hepatocerebral degeneration).
- Persistent HE accounts for 10–20% of liver transplant indications in Australia.
- Repeat episodes cause cumulative neurocognitive impairment that may not fully reverse post-transplant.
- Discuss with a transplant hepatologist at the nearest liver transplant centre (RPA/Concord NSW, Austin VIC, PAH QLD, Sir Charles Gairdner WA, Royal Adelaide SA).
- Include MELD score and HE frequency in referral documentation.
5. Driving & Occupational Counselling
- Patients with overt HE (any grade) must cease all driving immediately — this includes private and commercial licences.
- Minimal HE / covert HE — assess formally (PHES, EncephalApp Stroop); impaired patients must not drive.
- The treating physician has a duty to notify the relevant state/territory licensing authority (e.g., Transport for NSW, VicRoads, TMR QLD).
- Fitness to drive may be reassessed after ≥3 months of sustained freedom from overt HE on stable therapy, with normal cognitive testing.
- Commercial/heavy vehicle licence holders: stricter criteria; may require formal neuropsychological assessment.
Occupational counselling: Patients with HE should avoid occupations involving heavy machinery, working at heights, or safety-critical decision-making until formally assessed. Occupational therapy and neuropsychological assessment may be useful for return-to-work planning. Centrelink/NDIS referral may be appropriate for refractory cases.
Aboriginal and Torres Strait Islander peoples experience a significantly higher burden of liver disease and its complications compared with non-Indigenous Australians. HE management must be embedded in culturally safe, community-centred care.
📚 References
- 1. Vilstrup H, Amodio P, Bajaj J, et al. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology. 2014;60(2):715–735.
- 2. Rose CF, Amodio P, Bajaj JS, et al. Hepatic encephalopathy: novel insights into classification, pathophysiology and therapy. J Hepatol. 2020;73(6):1526–1547.
- 3. Bass NM, Mullen KD, Sanyal A, et al. Rifaximin treatment in hepatic encephalopathy. N Engl J Med. 2010;362(12):1071–1081.
- 4. Sharma BC, Sharma P, Lunia MK, et al. A randomized, double-blind, controlled trial comparing rifaximin plus lactulose with lactulose alone in treatment of overt hepatic encephalopathy. Am J Gastroenterol. 2013;108(9):1458–1463.
- 5. Gluud LL, Dam G, Borre M, et al. Lactulose, rifaximin or branched chain amino acids for hepatic encephalopathy: a meta-analysis. BMJ Open Gastroenterol. 2016;3(1):e000099.
- 6. Bai M, He T, Chai PY, et al. L-ornithine-L-aspartate for hepatic encephalopathy: a meta-analysis of randomised controlled trials. BMJ Open Gastroenterol. 2022;9(1):e000969.
- 7. Bajaj JS, Wade JB, Sanyal AJ. Spectrum of neurocognitive impairment in cirrhosis: implications for the assessment of hepatic encephalopathy. Hepatology. 2009;50(6):2014–2021.
- 8. Bajaj JS, Cordoba J, Mullen KD, et al. Review article: the design of clinical trials in hepatic encephalopathy — an International Society for Hepatic Encephalopathy and Nitrogen Metabolism (ISHEN) consensus statement. Aliment Pharmacol Ther. 2011;33(7):739–747.
- 9. Latt N, Bhat S, Patel P, et al. Australian burden of liver disease study: cirrhosis mortality in Aboriginal and Torres Strait Islander peoples. Med J Aust. 2022;216(6):299–304.
- 10. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework 2020 summary report. Canberra: AIHW; 2020.
- 11. RHDAustralia (Northern Territory Department of Health and Menzies School of Health Research). 2022 Australian national guidelines for the management of hepatitis B in Aboriginal and Torres Strait Islander peoples. Darwin: RHDAustralia; 2022.
- 12. European Association for the Study of the Liver (EASL). EASL Clinical Practice Guidelines on the management of hepatic encephalopathy. J Hepatol. 2022;77(3):807–824.