📋 Key Information Summary
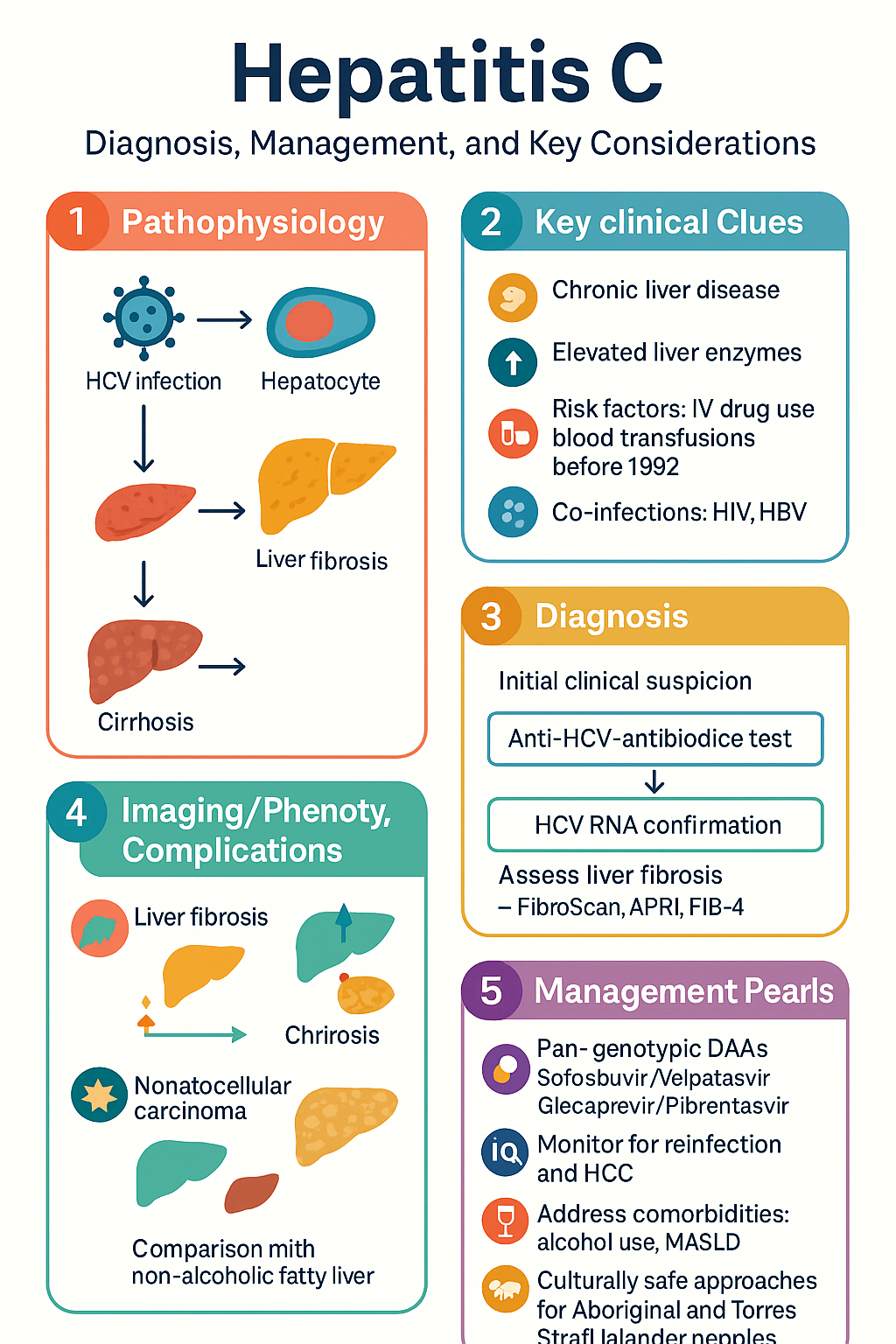
- Diagnosis requires anti-HCV antibody test followed by HCV RNA confirmation; RNA positivity defines active infection.
- All patients with chronic HCV require assessment of liver fibrosis using non-invasive tests (FibroScan, APRI, FIB-4) to guide treatment urgency and follow-up.
- Pan-genotypic direct-acting antiviral (DAA) regimens are first-line; routine genotype testing is no longer mandatory for treatment selection.
- Standard first-line regimens: Sofosbuvir/velpatasvir for 12 weeks, or glecaprevir/pibrentasvir for 8 weeks (treatment-naïve, non-cirrhotic).
- For compensated cirrhosis (Child-Pugh A), extend glecaprevir/pibrentasvir to 12 weeks; decompensated cirrhosis (Child-Pugh B/C) contraindicates protease inhibitors.
- DAA retreatment for prior failure: sofosbuvir/velpatasvir/voxilaprevir for 12 weeks is highly effective.
- HIV co-infection is not a barrier to treatment; check for drug interactions with antiretrovirals.
- Screen for and manage HBV co-infection due to risk of reactivation during DAA therapy; consider prophylactic antivirals.
- All DAAs, including those with protease inhibitors, are safe in severe renal impairment (eGFR <30 mL/min); no dose adjustment required.
- People who inject drugs should be actively offered treatment; ongoing drug use is not a contraindication.
- Achievement of SVR (sustained virological response) does not eliminate risk of hepatocellular carcinoma in those with pre-existing cirrhosis; lifelong surveillance is required.
- Post-SVR, monitor for reinfection in at-risk individuals with annual HCV RNA testing.
- Address comorbidities including alcohol use and metabolic dysfunction-associated steatotic liver disease (MASLD).
- Aboriginal and Torres Strait Islander peoples experience higher prevalence and require culturally safe, community-based approaches to testing and treatment.
Diagnosis & Assessment
Diagnostic Pathway
The diagnosis of hepatitis C virus (HCV) infection follows a two-step serological and virological pathway. Initial screening is with an anti-HCV antibody test. A positive result must be confirmed by a qualitative or quantitative HCV RNA test to distinguish resolved past infection from current active infection.
Baseline Investigations
A comprehensive baseline assessment is essential for treatment planning and safety monitoring.
Fibrosis Staging
Accurate staging of liver fibrosis is crucial as it determines treatment urgency, regimen choice, and post-treatment surveillance.
| Method | Description & Scoring | Interpretation |
|---|---|---|
| FibroScan (Transient Elastography) | Measures liver stiffness in kPa. Non-invasive, operator-dependent. | F0-2: <9.5 kPa; F3 (advanced fibrosis): 9.5-12.5 kPa; F4 (cirrhosis): >12.5 kPa. |
| APRI Score | (AST/ULN) / Platelet count (x10⁹/L) x 100. Simple laboratory-based score. | <0.5 rules out significant fibrosis; >1.5 suggests cirrhosis. |
| FIB-4 Index | (Age x AST) / (Platelet count x √ALT). Incorporates age. | <1.45 rules out advanced fibrosis; >3.25 suggests advanced fibrosis/cirrhosis. |
| Liver Biopsy | Histological assessment (METAVIR score). Gold standard but invasive. | F0: No fibrosis; F1: Portal; F2: Few septa; F3: Many septa; F4: Cirrhosis. |
DAA Therapy
Direct-acting antivirals (DAAs) are the cornerstone of HCV treatment, offering cure rates >95%. Pan-genotypic regimens have simplified treatment. Choice of regimen depends on fibrosis stage, prior treatment history, and comorbidities.
First-Line Pan-Genotypic Regimens
Special Circumstances & Retreatment
Special Populations
DAA therapy is highly effective across diverse patient groups. Treatment should not be delayed or denied based on the factors below.
- Glecaprevir/Pibrentasvir: Avoid with atazanavir, darunavir. Safe with dolutegravir, bictegravir.
- Sofosbuvir/Velpatasvir: Fewer interactions; generally safe with most INSTIs.
- Tip: Consult the Liverpool HIV Drug Interactions Database.
- HBsAg Positive: Start prophylactic entecavir or tenofovir (alongside DAAs) and continue for 12-24 weeks post-DAA.
- HBsAg Negative, anti-HBc Positive: Monitor HBV DNA monthly during and for 6 months after DAA therapy. Treat if reactivation occurs.
- Offer treatment in conjunction with harm reduction services (needle/syringe programmes, OST).
- Adherence and SVR rates in PWID are comparable to other populations with appropriate support.
- Address reinfection risk through education and ongoing engagement.
Post-SVR & Follow-up
Achievement of a Sustained Virological Response (SVR, defined as undetectable HCV RNA 12 weeks post-treatment) indicates cure. However, ongoing management is essential.
Key Follow-up Components
Aboriginal and Torres Strait Islander Health
Hepatitis C disproportionately affects Aboriginal and Torres Strait Islander peoples, with higher prevalence, incidence, and morbidity. A culturally safe, holistic, and community-controlled health service-led approach is essential.
📚 References
- 1. World Health Organization. Guidelines for the care and treatment of persons diagnosed with chronic hepatitis C virus infection. Geneva: WHO; 2024.
- 2. European Association for the Study of the Liver. EASL Recommendations on Treatment of Hepatitis C: Final update of the series. J Hepatol. 2023;79(4):1005-1036.
- 3. Australian Government Department of Health. National Hepatitis C Strategy 2023–2030. Canberra: Commonwealth of Australia; 2023.
- 4. The Kirby Institute. HIV, viral hepatitis and sexually transmissible infections in Australia: Annual surveillance report 2023. Sydney: UNSW; 2023.
- 5. Australian Society for HIV, Viral Hepatitis and Sexual Health Medicine (ASHM). Quick Reference Guide: Hepatitis C Management in the DAA Era. Sydney: ASHM; 2022.
- 6. Pharmaceutical Benefits Scheme (PBS). Sofosbuvir with velpatasvir (Epclusa). Australian Government Department of Health. Accessed 2024.
- 7. Pharmaceutical Benefits Scheme (PBS). Glecaprevir with pibrentasvir (Mavyret). Australian Government Department of Health. Accessed 2024.
- 8. Hepatitis B Virus Reactivation in Patients with Hepatitis C Virus Treated with Direct-Acting Antivirals: A Systematic Review and Meta-analysis. Clin Infect Dis. 2022;74(8):1435-1444.
- 9. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander health performance framework 2023 summary report. Canberra: AIHW; 2023.
- 10. National Aboriginal Community Controlled Health Organisation (NACCHO). Position Statement: Viral Hepatitis. Canberra: NACCHO; 2022.
- 11. Martinello M, et al. Simplified monitoring for hepatitis C virus treatment with sofosbuvir plus ribavirin in the REASON study. J Viral Hepat. 2023;30(2):156-167.
- 12. Dore GJ, et al. Glecaprevir/Pibrentasvir for 8 Weeks in Treatment-Naïve Patients with HCV Genotypes 1-6 and Compensated Cirrhosis: The EXPEDITION-8 Trial. Hepatology. 2022;75(3):670-681.