📋 Key Information Summary
- Haemorrhoids and anal fissures are the most common benign anorectal conditions presenting to Australian GPs, with haemorrhoids affecting up to 40% of adults over 50 years.
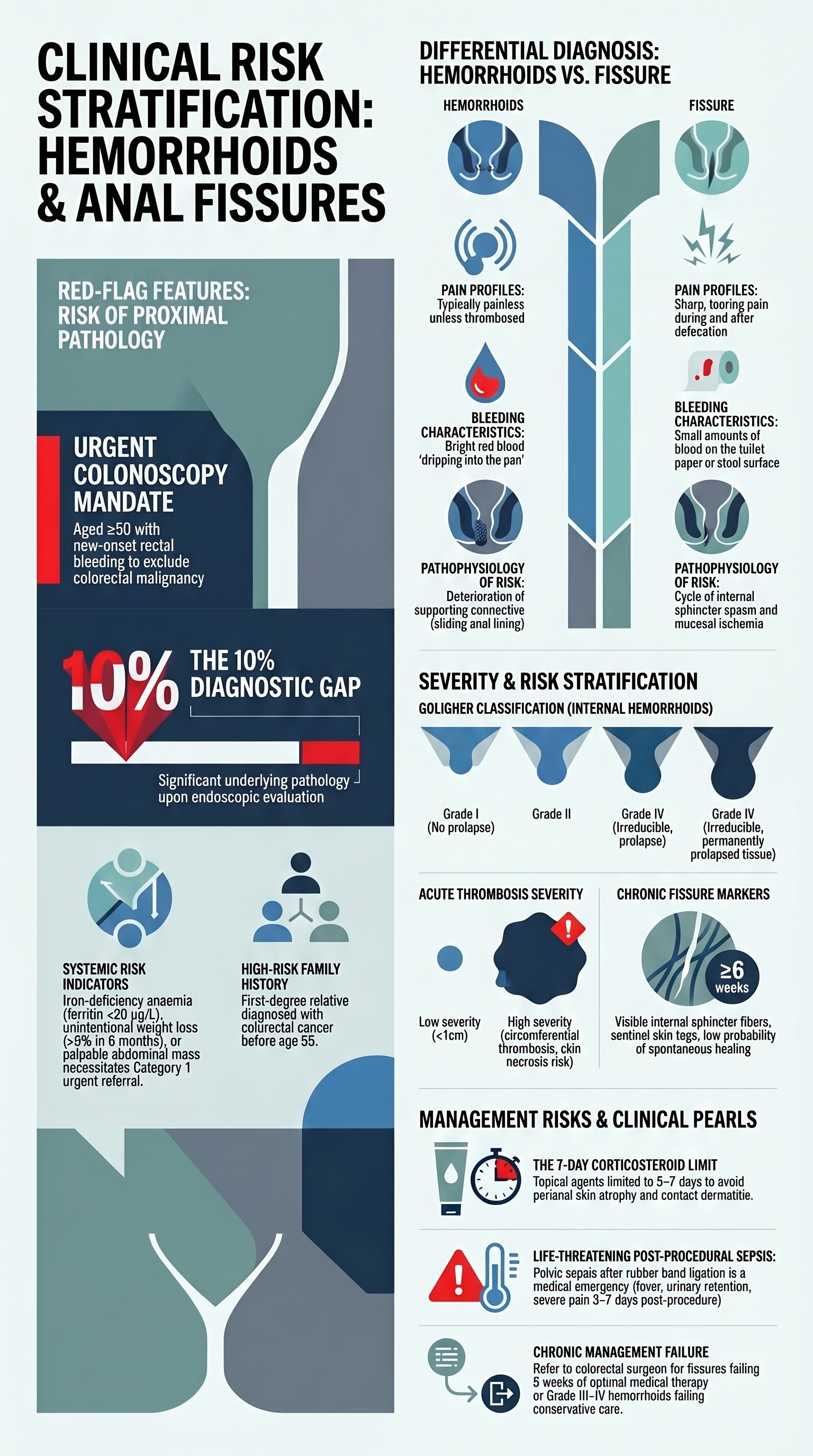
- Red-flag features requiring urgent colonoscopy or specialist referral include rectal bleeding with iron-deficiency anaemia, change in bowel habit, weight loss, family history of colorectal cancer in a first-degree relative <55 years, and age ≥50 with new-onset bleeding.
- History must characterise bleeding (colour, volume, relationship to defecation), pain (acute vs chronic, relationship to defecation), prolapse, and bowel habit to distinguish haemorrhoids from fissure and exclude proximal pathology.
- Perianal inspection and digital rectal examination are essential first-line; proctoscopy/anoscopy should be performed in the primary care setting where trained, with flexible sigmoidoscopy or colonoscopy for red-flag evaluation.
- Conservative management is first-line for both conditions: dietary fibre supplementation (psyllium 3.5 g BD), adequate fluids (≥1.5 L/day), sitz baths (warm water 10–15 min TDS), topical agents, and toilet habit modification.
- Topical GTN (0.4% rectal ointment, Rectogesic®) or topical calcium-channel blocker (diltiazem 2% ointment) are first-line pharmacological therapy for anal fissures, achieving healing in 60–70% of cases.
- Haemorrhoid-specific topical agents containing corticosteroids should be limited to 5–7 days to avoid perianal skin atrophy and contact dermatitis.
- Rubber band ligation (RBL) is the most common office-based procedure for grade II–III haemorrhoids, with success rates of 70–80% per session; it is PBS-indicated for specialist use.
- Referral to a colorectal surgeon is indicated for: grade III–IV haemorrhoids failing conservative therapy, recurrent or chronic fissures not healing after 8 weeks of optimal medical therapy, and suspected fistula-in-ano or abscess.
- Aboriginal and Torres Strait Islander peoples experience higher rates of constipation and anorectal disease due to healthcare access barriers; culturally safe education and accessible primary care pathways are essential.
- Special populations require modified management: avoid systemic decongestants in pregnancy, cautious corticosteroid use in immunocompromised patients, and dose-adjustment considerations in the elderly with polypharmacy.
Introduction & Australian Epidemiology
Haemorrhoids and anal fissures represent the two most prevalent benign anorectal conditions encountered in Australian general practice and gastroenterology clinics. Together, they account for the vast majority of perianal complaints and rectal bleeding presentations in adults. Despite their benign nature, these conditions significantly impair quality of life, cause considerable anxiety (particularly regarding rectal bleeding), and impose a substantial burden on the Australian healthcare system.
Haemorrhoids — vascular cushions of the anal canal that become symptomatic when engorged, prolapsing, or thrombosed — affect an estimated 4.4% of the general population globally, with Australian studies suggesting a prevalence of 25–40% in adults over 50 years of age. The true prevalence is likely higher, as many patients self-manage without seeking medical attention. Risk factors include constipation, straining, low-fibre diets, prolonged sitting, pregnancy, obesity, and increasing age. Haemorrhoids are classified by the Goligher system: grade I (no prolapse), grade II (prolapse that reduces spontaneously), grade III (prolapse requiring manual reduction), and grade IV (irreducible prolapse).
Anal fissures — linear ulcers in the squamous epithelium of the anal canal, typically at the posterior midline — are the most common cause of anal pain and bright red rectal bleeding in young adults. Peak incidence occurs between 15 and 40 years, with a slight male predominance. Acute fissures (present for <6 weeks) heal spontaneously in approximately 50–60% of cases with conservative measures. Chronic fissures (≥6 weeks duration) are characterised by exposed internal sphincter fibres, sentinel skin tags, and hypertrophied anal papillae, and are less likely to resolve without targeted intervention.
The Australian Institute of Health and Welfare (AIHW) reports that anorectal conditions account for over 500,000 GP consultations annually. Rectal bleeding, the cardinal symptom of both conditions, must be carefully evaluated, as the Royal Australian College of General Practitioners (RACGP) red-book guidelines recommend colonoscopic evaluation for any patient aged ≥50 with new-onset rectal bleeding to exclude colorectal malignancy.
Pathophysiology
Haemorrhoids
The anal canal contains three principal haemorrhoidal cushions (left lateral, right anterior, and right posterior) composed of arteriovenous channels, smooth muscle (Treitz's muscle), and connective tissue. These cushions contribute to 15–20% of resting anal continence. Symptomatic haemorrhoids develop when the vascular plexus becomes engorged and the supporting connective tissue deteriorates, leading to downward displacement and prolapse. The primary mechanisms include:
- Sliding anal lining theory: Degeneration of Treitz's muscle and submucosal connective tissue allows downward displacement of the haemorrhoidal cushions.
- Hyperperfusion theory: Elevated anal canal pressures and increased arterial inflow to the haemorrhoidal plexus contribute to engorgement.
- Internal sphincter dysfunction: Raised resting anal pressures are observed in many patients, though the relationship is complex.
External haemorrhoids are covered by squamous epithelium and are innervated by somatic nerve fibres; thrombosis of external haemorrhoids causes acute severe perianal pain. Internal haemorrhoids are covered by columnar epithelium and are insensate; they typically present with painless bright red rectal bleeding.
Anal Fissures
Acute anal fissures most commonly result from mechanical trauma during passage of hard stool. The posterior midline is affected in approximately 80–90% of cases due to relatively poor vascular supply at this site. The pathophysiology of chronic fissures involves a self-perpetuating cycle:
- Mucosal trauma leads to pain → internal sphincter spasm → raised anal resting pressure.
- Elevated resting pressure reduces mucosal blood flow (ischaemia) at the posterior commissure.
- Ischaemia impairs healing → chronic ulceration → further spasm → perpetuation of the cycle.
This pathophysiological understanding underpins pharmacological treatments targeting sphincter relaxation (GTN, diltiazem, botulinum toxin) to restore mucosal blood flow. Non-healing fissures (anterior midline, multiple, off-midline, or atypical) should raise suspicion for Crohn's disease, HIV, tuberculosis, syphilis, or malignancy.
Initial Assessment
History
A thorough history is the cornerstone of the initial assessment. The presenting complaint should be carefully characterised to distinguish haemorrhoids from fissures and to exclude more serious proximal pathology.
| Symptom Domain | Haemorrhoids | Anal Fissure |
|---|---|---|
| Bleeding | Painless, bright red, on wiping or dripping into pan; coats the stool surface | Small amount of bright red blood on toilet paper or surface of stool |
| Pain | Usually absent unless thrombosed (acute severe perianal pain) or strangulated | Sharp, tearing pain during defecation; may persist for hours post-defecation |
| Prolapse | Lump at anal verge, reducible (grade II/III) or irreducible (grade IV) | Sentinel skin tag at anal verge; no true prolapse |
| Itching | Perianal pruritus common with prolapsing or mucoid discharge | Less common |
| Discharge | Mucoid discharge with internal haemorrhoids | Rarely significant |
Red-Flag Features — Exclude Proximal Pathology
- Age ≥50 years with new-onset rectal bleeding (colorectal cancer screening mandate per RACGP Red Book)
- Iron-deficiency anaemia (ferritin <30 µg/L, low MCV) with rectal bleeding
- Change in bowel habit (persistent diarrhoea or constipation >6 weeks)
- Unintentional weight loss (>5% body weight in 6 months)
- Family history of colorectal cancer in first-degree relative <55 years
- Dark or mixed rectal bleeding (melaena or maroon stool suggesting proximal source)
- Palpable abdominal or rectal mass
- New-onset symptoms in patients with inflammatory bowel disease, hereditary polyposis syndromes, or prior pelvic radiotherapy
Physical Examination
A systematic examination of the anorectal region should be performed with the patient in the left lateral position:
- Inspection: Gently part the buttocks to examine the perianal skin. Look for external haemorrhoids (bluish-purple swellings), thrombosed external haemorrhoid (tender, firm, blue nodule), sentinel skin tag (fissure), excoriation (pruritus), abscess (erythema, swelling, fluctuance), fistula opening, and any suspicious lesions.
- Digital rectal examination (DRE): Assess resting and squeeze anal tone, palpate for masses, tenderness, and induration. The posterior midline may be exquisitely tender in acute fissures (use gentle technique with adequate lubrication).
- Proctoscopy/Anoscopy: Essential to visualise internal haemorrhoids and the anal canal mucosa. Should be performed in primary care where training and equipment allow. Reveals the triad of chronic fissure: visible internal sphincter fibres, sentinel tag, and hypertrophied anal papilla.
- Flexible sigmoidoscopy/Colonoscopy: Required when red-flag features are present, or when the diagnosis is uncertain after initial assessment.
Goligher Classification of Internal Haemorrhoids
Investigations
The investigation strategy depends on clinical presentation, patient age, and presence of red-flag features.
Risk Stratification & Severity Assessment
Acute Thrombosed External Haemorrhoid
Thrombosis of an external haemorrhoid typically presents within the first 48–72 hours as a painful, firm, blue-purple perianal lump. Risk stratification determines management pathway:
Anal Fissure — Acute vs Chronic
| Feature | Acute Fissure (<6 weeks) | Chronic Fissure (≥6 weeks) |
|---|---|---|
| Appearance | Clean, linear mucosal tear | Deep ulcer with visible internal sphincter fibres, sentinel tag, hypertrophied papilla |
| Pain pattern | Brief, during defecation only | Severe, lasting hours post-defecation; may be constant |
| Spontaneous healing | 50–60% within 6–8 weeks | Rare without targeted intervention |
| First-line Rx | Conservative measures | Topical GTN or diltiazem ± botulinum toxin |
Conservative Management
Conservative management is the first-line approach for all grades of haemorrhoids and acute anal fissures. It should be trialled for a minimum of 4–6 weeks before escalation. The pillars of conservative therapy are:
1. Dietary Fibre Supplementation
Increased dietary fibre softens stool, reduces straining, and decreases intra-abdominal pressure. A systematic review (Cochrane, 2023) demonstrated that fibre supplementation significantly reduces bleeding and overall symptom scores in haemorrhoid patients. Target fibre intake: 25–30 g/day.
2. Adequate Fluid Intake
Patients should aim for ≥1.5 L (approximately 8 glasses) of non-caffeinated fluid daily. Adequate hydration is essential for the efficacy of fibre supplementation; without sufficient water, bulk-forming agents can paradoxically worsen constipation.
3. Sitz Baths
Warm water sitz baths (plain water, 37–40°C, for 10–15 minutes, 2–3 times daily and after each bowel movement) provide analgesic and muscle-relaxant effects. They are particularly beneficial for:
- Acute anal fissures — promote internal sphincter relaxation and improve mucosal blood flow
- Thrombosed external haemorrhoids — reduce pain and oedema
- Post-procedural care (e.g., after rubber band ligation or haemorrhoidectomy)
There is no evidence that adding antiseptics, salt, or other additives improves outcomes over plain warm water.
4. Topical Agents
For Haemorrhoids
For Anal Fissures — Sphincter Relaxants
5. Toilet Habit Modification
Patient education on appropriate toilet habits is a critical but often neglected component of management:
- Avoid prolonged sitting on the toilet: Limit toilet time to <5 minutes. Do not use mobile phones or read on the toilet — this leads to prolonged straining and venous engorgement of haemorrhoidal cushions.
- Avoid straining: Straining increases intra-abdominal pressure and worsens haemorrhoidal engorgement. Respond to the urge to defecate promptly (the gastrocolic reflex), and do not delay.
- Optimal positioning: A squatting position or use of a footstool to elevate the knees above the hips straightens the anorectal angle and facilitates easier defecation with less straining.
- Avoid forceful wiping: Use moist toilet paper, bidet, or gentle dabbing. Rough wiping exacerbates both fissures and external haemorrhoidal irritation.
6. Symptomatic Analgesia
Directed / Pathogen-Specific Therapy
This section covers second-line and procedural interventions for haemorrhoids and fissures that persist despite optimal conservative management.
Second-Line Pharmacological Therapy for Anal Fissures
Procedural Interventions for Haemorrhoids
| Procedure | Indication | Setting | Success Rate | Notes |
|---|---|---|---|---|
| Rubber Band Ligation (RBL) | Grade II–III haemorrhoids | Outpatient / GI specialist rooms | 70–80% per session; up to 3 sessions at 4–6 week intervals | Most common office procedure. Band placed 2 cm above the dentate line. Mild discomfort, minor bleeding expected. Rare: severe bleeding, pelvic sepsis (present with fever + urinary retention — medical emergency) |
| Injection Sclerotherapy | Grade I–II haemorrhoids | Outpatient | 70–80% for grade I; less effective for grade III | Phenol-in-almond-oil injected into submucosa. Lower recurrence rates than RBL for grade I. Useful in anticoagulated patients. |
| Haemorrhoidectomy (excisional) | Grade III–IV haemorrhoids, recurrent disease | Hospital — day case or overnight | >95% cure rate; lowest recurrence | Gold standard for advanced haemorrhoids. Open (Milligan-Morgan) or closed (Ferguson) technique. Post-operative pain is the main morbidity; 2–4 weeks recovery. |
| Haemorrhoidal Artery Ligation (HAL/THD) | Grade II–III haemorrhoids | Hospital — day case | 85–90% | Doppler-guided ligation of haemorrhoidal arteries ± mucopexy. Less post-operative pain than excisional. Increasing availability in Australian tertiary centres. |
| Stapled Haemorrhoidopexy | Grade III haemorrhoids (circumferential) | Hospital | 80–90% | Circular stapler resects prolapsing tissue and restores anatomy. Less pain than excisional but higher recurrence rate. Rare but serious: rectal perforation, retroperitoneal sepsis. |
Surgical Interventions for Anal Fissures
| Procedure | Indication | Success Rate | Key Risks |
|---|---|---|---|
| Lateral Internal Sphincterotomy (LIS) | Chronic fissure failing ≥8 weeks optimal medical therapy | 90–95% healing; gold standard surgical treatment | Faecal incontinence (flatus 5–10%, solid stool <2%); most cases are minor and transient. Risk higher in women (thinner sphincter) and elderly. |
| Advancement Flap | Chronic fissure with risk factors for incontinence (multiparous women, elderly, pre-existing sphincter weakness) | 80–90% | Sphincter-sparing option; avoids sphincterotomy risk. Longer operative time. Limited to specialist colorectal surgeons. |
Monitoring
Follow-Up Schedule
Monitoring Parameters
| Parameter | When | Action |
|---|---|---|
| FBC + iron studies | Baseline if recurrent bleeding; repeat at 3 months | If Hb falling or ferritin low → urgent colonoscopy regardless of suspected haemorrhoidal source |
| Symptom diary | Throughout treatment | Bleeding episodes, pain severity (VAS 0–10), bowel frequency, stool consistency (Bristol chart) |
| Anal examination | 6–8 weeks post-topical therapy; post-procedure | Fissure healing, haemorrhoid grade progression, exclude new pathology |
| Continence assessment | Post-LIS or post-haemorrhoidectomy | Wexner incontinence score; physiotherapy referral if faecal incontinence develops |
Special Populations
Pregnancy
- Prevalence: Haemorrhoids affect 25–35% of pregnant women, most commonly in the third trimester and postpartum period, due to progesterone-mediated venous relaxation, increased pelvic blood volume, and constipation.
- Conservative management is first-line: Dietary fibre, fluids, sitz baths, and toilet habit modification are safe and should be initiated early.
- Safe medications: Psyllium (B category), paracetamol, hydrocortisone-based rectal preparations (short course ≤5 days). Lactulose 15 mL BD is a safe osmotic laxative in pregnancy.
- Avoid: GTN 0.4% ointment (hypotension risk; not recommended in pregnancy). Diltiazem topical — limited safety data; avoid unless specialist-directed. NSAIDs (especially in the third trimester — risk of premature ductus arteriosus closure). Stimulant laxatives (senna, bisacodyl) for prolonged use.
- Procedures: Rubber band ligation should be deferred until postpartum. Acutely thrombosed external haemorrhoids may be excised under local anaesthesia if severely symptomatic.
- Postpartum: Most pregnancy-related haemorrhoids improve significantly within 6–8 weeks post-delivery. Persistent symptoms should be managed as per standard guidelines.
Paediatrics
- Haemorrhoids are rare in children. Rectal bleeding in children is more commonly due to anal fissure, Meckel's diverticulum, intussusception, juvenile polyps, or inflammatory bowel disease.
- Anal fissures are the most common cause of rectal bleeding in infancy and childhood, almost always related to constipation.
- Treatment: Address underlying constipation with dietary fibre, adequate fluids, and osmotic laxatives (macrogol 3350 — first-line in paediatrics). Topical GTN and diltiazem are not recommended in children. Barrier cream (zinc oxide, petroleum jelly) applied perianally before defecation reduces pain.
- Red flags in children: Chronic diarrhoea, bloody diarrhoea, weight loss, perianal fistula or skin tags → refer for investigation of inflammatory bowel disease. Consider child protection evaluation if perianal injury is unexplained.
Elderly (≥65 years)
- Higher prevalence of haemorrhoids due to cumulative connective tissue deterioration, chronic constipation, polypharmacy (anticholinergics, opioids, calcium-channel blockers, iron supplements).
- Increased colonoscopy threshold: All patients ≥50 with new rectal bleeding should undergo colonoscopy per RACGP red-book; lower threshold in elderly given higher CRC incidence.
- Medication considerations: GTN ointment — increased hypotension and headache risk in elderly; consider diltiazem 2% as preferred first-line topical for fissures. Review polypharmacy for constipating agents.
- Surgical caution: Lateral internal sphincterotomy carries higher risk of faecal incontinence in elderly patients due to pre-existing sphincter weakness. Advancement flap may be preferred. Assess baseline continence before any procedural intervention.
- Bleeding assessment: Iron-deficiency anaemia in the elderly should always be investigated for colorectal malignancy, even in the presence of known haemorrhoids.
Renal Impairment
- Constipation is more prevalent in CKD due to phosphate binders (calcium carbonate, sevelamer), iron supplements, and reduced fluid intake (in patients on fluid restriction).
- Safe laxatives: Psyllium, lactulose, macrogol 3350 (monitor electrolytes in severe CKD, eGFR <30). Avoid magnesium-containing laxatives in severe renal impairment (hypermagnesaemia risk).
- Topical GTN/diltiazem: No dose adjustment required; minimal systemic absorption. Safe in renal impairment.
- Avoid ibuprofen — risk of AKI. Paracetamol preferred for analgesia (no dose adjustment unless concurrent hepatic disease).
Hepatic Impairment
- Portal hypertension: Rectal varices may mimic haemorrhoids in patients with portal hypertension (cirrhosis). Differentiation is critical — biopsy or injection of haemorrhoids in portal hypertensive patients carries life-threatening haemorrhage risk.
- Topical agents: GTN and diltiazem — no dose adjustment for topical use. Short-course hydrocortisone rectal preparations are safe.
- Paracetamol: Reduce maximum dose to 2 g/24 hrs in significant hepatic impairment.
- Procedural risk: Coagulopathy must be corrected before any invasive procedure. Rubber band ligation and surgery in patients with cirrhosis and coagulopathy carry elevated bleeding risk — MDT discussion required.
Immunocompromised
- HIV/AIDS: Atypical and non-healing fissures are common. Consider CMV, HSV, and syphilis as causes of perianal ulceration. CD4 count determines investigation urgency.
- Transplant recipients and immunosuppressed patients: Poor wound healing, increased infection risk with procedural interventions. Sphincterotomy and haemorrhoidectomy should be avoided where possible; medical management preferred. If surgery is required, ensure optimisation of immunosuppression and prophylactic antibiotics.
- Corticosteroid caution: Perianal corticosteroid preparations should be used at the lowest effective dose and shortest duration in immunocompromised patients due to increased risk of perianal fungal superinfection.
Referral for Procedures
Referral to a gastroenterologist or colorectal surgeon is indicated when persistent symptomatic haemorrhoids or fissures fail optimal conservative therapy. The decision to refer should consider symptom severity, impact on quality of life, response to medical treatment, and patient preference.
Indications for Gastroenterology Referral
- Rectal bleeding requiring colonoscopic evaluation (age ≥50, iron-deficiency anaemia, change in bowel habit, family history CRC)
- Internal haemorrhoids amenable to rubber band ligation or injection sclerotherapy
- Diagnostic uncertainty — atypical fissures or lesions requiring biopsy
- Suspected inflammatory bowel disease presenting as perianal disease
Indications for Colorectal Surgery Referral
- Grade III–IV haemorrhoids failing conservative and office-based treatments
- Thrombosed external haemorrhoid presenting >72 hours or with extensive circumferential involvement
- Chronic anal fissure (>8 weeks) failing topical GTN or diltiazem therapy
- Recurrent fissures after initial healing
- Suspected fistula-in-ano, intersphincteric or perianal abscess
- Atypical fissures (off-midline, multiple, suspicious morphology) requiring biopsy
- Patients with significant faecal incontinence symptoms who may benefit from advancement flap rather than sphincterotomy
Referral Priority (Recommended Timeframes)
Preparing the Patient for Referral
Aboriginal and Torres Strait Islander Health
Aboriginal and Torres Strait Islander peoples experience a significantly higher burden of gastrointestinal disease, including anorectal conditions, compared with the non-Indigenous Australian population. The AIHW reports that Indigenous Australians have higher rates of constipation, haemorrhoidal disease, and perianal sepsis, often presenting at a later stage due to barriers in healthcare access. Culturally safe, community-centred approaches are essential for effective management.
📚 References
- 1. Lohsiriwat V. Hemorrhoids: from basic pathophysiology to clinical management. World J Gastroenterol. 2012;18(17):2009–2017.
- 2. Wald A, Bharucha AE, Cosman BC, Whitehead WE. ACG Clinical Guideline: Management of Benign Anorectal Disorders. Am J Gastroenterol. 2014;109(8):1141–1157.
- 3. Nelson RL, Thomas K, Morgan J, Jones A. Non-surgical therapy for anal fissure. Cochrane Database Syst Rev. 2012;(2):CD003431.
- 4. Royal Australian College of General Practitioners. Guidelines for Preventive Activities in General Practice (Red Book). 9th edn. Melbourne: RACGP; 2018.
- 5. Australian Institute of Health and Welfare. Cancer data in Australia. AIHW, Canberra; 2023. Cat. no. CAN 146.
- 6. Davis BR, Lee-Kong SA, Migaly J, Feingold DL, Steele SR. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Hemorrhoids. Dis Colon Rectum. 2018;61(3):284–292.
- 7. Simillis C, Thoukididou SN, Slesser AA, Rasheed S, Tan E, Tekkis PP. Systematic review and network meta-analysis comparing clinical outcomes and effectiveness of surgical treatments for haemorrhoids. Br J Surg. 2015;102(13):1603–1618.
- 8. Altomare DF, Binda G, Bottini C, et al. Topical diltiazem ointment and glyceryl trinitrate for anal fissure: a meta-analysis. Colorectal Dis. 2013;15(5):e248–e256.
- 9. Beaty JS, Shashidharan M. Anal fissure. Clin Colon Rectal Surg. 2016;29(1):30–37.
- 10. National Bowel Cancer Screening Program Monitoring Report 2023. Australian Institute of Health and Welfare. AIHW, Canberra; 2023.
- 11. Conaghan P, Figueiredo M, McGregor L, et al. Management of haemorrhoids in pregnancy: a systematic review. Int J Colorectal Dis. 2022;37(4):787–796.
- 12. Aboriginal and Torres Strait Islander Health Performance Framework — Summary Report. Australian Institute of Health and Welfare. AIHW, Canberra; 2023.
- 13. Garg P, Garg M, Menon GR. Long-term continence disturbance after lateral internal sphincterotomy for chronic anal fissure: a systematic review and meta-analysis. Colorectal Dis. 2013;15(3):e104–e117.
- 14. Cross AJ, Buchbinder R, Bourne A, et al. Gastrointestinal disease burden in Aboriginal and Torres Strait Islander peoples: a population-based study. Aust N Z J Public Health. 2021;45(3):245–251.
- 15. Perera N, Liolitsa D, Iype S, et al. Phlebotonics for haemorrhoids. Cochrane Database Syst Rev. 2012;(8):CD004322.