📋 Key Information Summary
- Ascites is the most common complication of cirrhosis, present in ~50% of patients at 10 years; its development marks a critical turning point with ~50% 2-year mortality without transplant.
- Diagnostic paracentesis is mandatory in ALL new-onset ascites and on every hospital admission — do not delay for coagulopathy or thrombocytopenia; serious bleeding occurs in <1%.
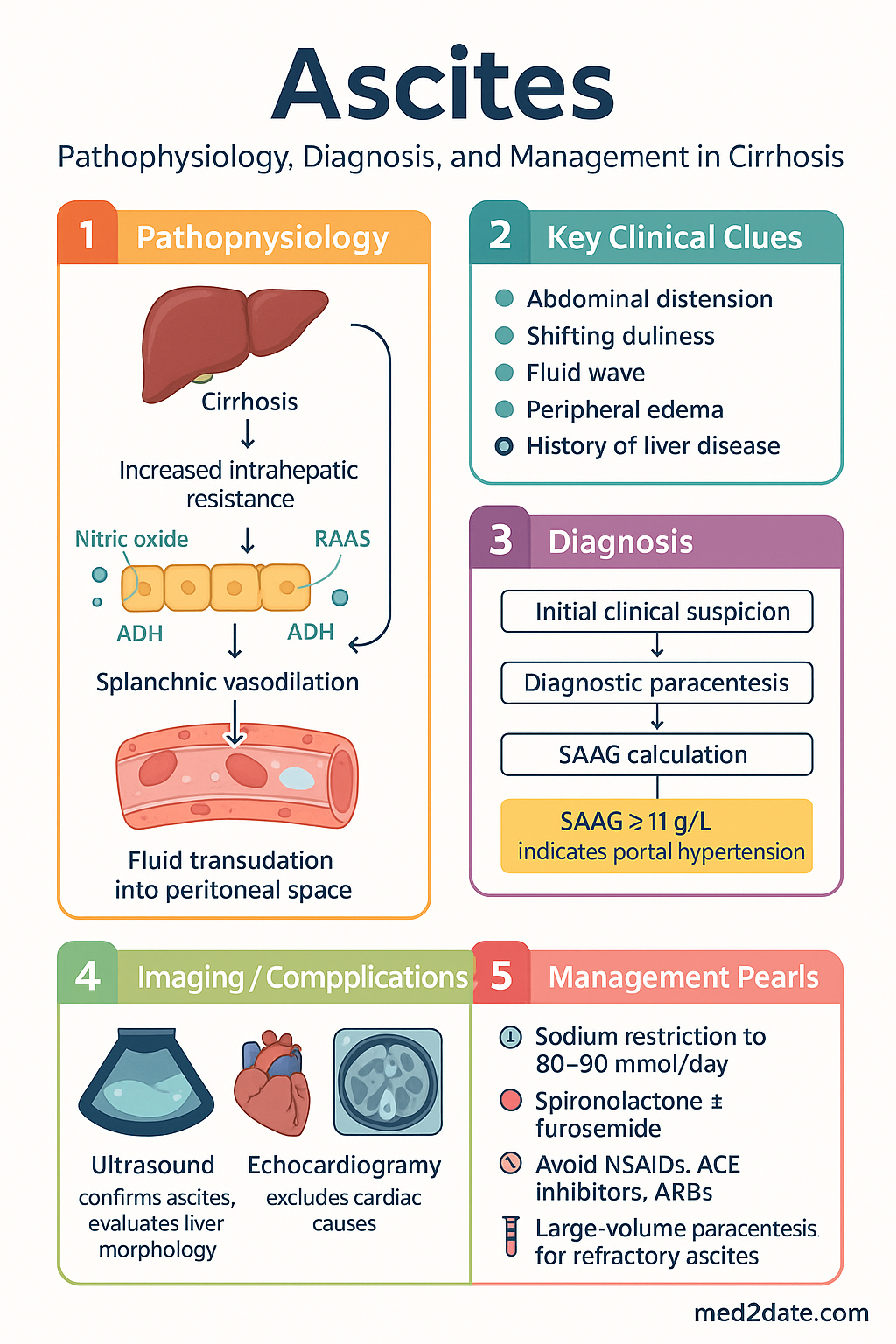
- Calculate the serum–ascites albumin gradient (SAAG) = serum albumin minus ascitic fluid albumin; SAAG ≥11 g/L indicates portal hypertension as the cause.
- Ascitic fluid cell count >250 polymorphonuclear cells/µL is diagnostic of spontaneous bacterial peritonitis (SBP) — start empirical antibiotics immediately.
- First-line medical management: sodium restriction to 80–90 mmol/day (~5 g salt) plus spironolactone 100 mg daily, adding furosemide 40 mg daily if needed; maintain 100:40 ratio, maximum 400:160 mg daily.
- Target weight loss of 0.5 kg/day without peripheral oedema, 1.0 kg/day with oedema; monitor daily weights, serum electrolytes, creatinine, and urea.
- Avoid NSAIDs, ACE inhibitors, ARBs, and aminoglycosides in cirrhotic ascites — these precipitate hepatorenal syndrome or worsen sodium retention.
- Fluid restriction is only necessary when serum sodium falls below 125 mmol/L; routine fluid restriction is not required.
- Refractory ascites (diuretic-resistant or diuretic-intractable) occurs in ~10% and requires large-volume paracentesis (LVP) with albumin replacement (8 g per litre removed when >5 L drained).
- TIPS reduces re-accumulation in refractory ascites but increases hepatic encephalopathy risk — patient selection requires MELD score, Child-Pugh assessment, and echocardiographic evaluation.
- Early transplant referral is essential once ascites develops; all patients with cirrhotic ascites should be assessed for liver transplantation.
- Aboriginal and Torres Strait Islander peoples experience higher rates of cirrhosis and its complications; culturally safe care and addressing geographic barriers are central to equitable management.
🎧 Audio Brief
Introduction & Australian Epidemiology
Ascites — the pathological accumulation of fluid within the peritoneal cavity — is the most frequent major complication of cirrhosis and the commonest cause of ascites in Australia, accounting for approximately 85% of all cases. The development of ascites in a patient with cirrhosis signals a transition from compensated to decompensated disease, with a dramatic reduction in survival from a median of >12 years (compensated) to approximately 2 years without liver transplantation.
In Australia, liver disease is the tenth leading cause of death, and cirrhosis accounts for a growing proportion of hepatology referrals nationwide. The AIHW reports that chronic liver disease mortality is increasing, driven predominantly by alcohol-related liver disease, metabolic dysfunction-associated steatotic liver disease (MASLD, formerly NAFLD), and viral hepatitis (hepatitis B and C). Ascites is the presenting feature in a significant proportion of these hospitalisations.
Aboriginal and Torres Strait Islander peoples experience cirrhosis at rates 3–5 times higher than non-Indigenous Australians, with alcohol-related liver disease and hepatitis B being the predominant aetiologies. Remote and regional communities face additional challenges in accessing timely diagnostic paracentesis, specialist hepatology input, and liver transplantation services.
This guideline provides a practical, evidence-based approach to the diagnosis, medical management, and management of refractory ascites in the Australian healthcare context, aligned with AASLD/EASL recommendations and adapted for local resource availability and PBS-listed medications.
Pathophysiology
The formation of ascites in cirrhosis is driven by portal hypertension and the resulting haemodynamic derangements. Increased intrahepatic resistance to portal flow (due to architectural distortion, fibrosis, and dynamic vasoconstriction) raises sinusoidal hydrostatic pressure, promoting transudation of fluid into the peritoneal space.
Two complementary theories explain the systemic sodium and water retention:
- Peripheral arterial vasodilation hypothesis: Portal hypertension triggers splanchnic vasodilation via nitric oxide and other vasodilators, reducing effective arterial blood volume. This activates the renin–angiotensin–aldosterone system (RAAS), sympathetic nervous system, and non-osmotic release of antidiuretic hormone (ADH/vasopressin), leading to renal sodium and water retention.
- Overflow hypothesis: Renal sodium retention may also be a primary hepatorenal reflex, with the liver itself signalling the kidneys to retain sodium independent of effective circulating volume.
As cirrhosis progresses, the balance shifts — ascites becomes refractory when splanchnic vasodilation is so severe that renal perfusion falls to critical levels, limiting the efficacy and tolerability of diuretics. This underpins the rationale for TIPS (reducing portal pressure) and liver transplantation (definitive correction).
Diagnosis
Diagnostic Paracentesis
Paracentesis should be performed using a 22-gauge needle under ultrasound guidance when available. The preferred site is the left lower quadrant (2 cm medial and 2 cm cephalad to the anterior superior iliac spine), where the abdominal wall is thinner and fluid is often maximal.
Essential Ascitic Fluid Tests
| Test | Purpose & Interpretation |
|---|---|
| Cell count & differential | PMN ≥250 cells/µL is diagnostic of SBP — start empirical antibiotics immediately. Red cell count >10,000/µL suggests traumatic tap or haemorrhage. |
| Total protein & albumin | Calculate SAAG (serum albumin minus ascitic fluid albumin). SAAG ≥11 g/L = portal hypertension with ~97% accuracy. SAAG <11 g/L suggests non-portal hypertensive cause (malignancy, TB, nephrotic syndrome). |
| Serum albumin (simultaneous) | Required for SAAG calculation. Must be drawn on the same day as paracentesis. |
| Cytology | Send if peritoneal carcinomatosis or hepatocellular carcinoma with peritoneal seeding is suspected. Sensitivity increases with ≥1 L of fluid collected. |
| Amylase | Elevated if ascites is due to pancreatic disease or pancreaticopleural fistula. Not routinely required unless clinically suspected. |
| Culture (bedside inoculation) | Inoculate 10 mL into aerobic and anaerobic blood culture bottles at the bedside — more sensitive than sending fluid to the laboratory in a sterile container. |
Serum–Ascites Albumin Gradient (SAAG)
• SAAG ≥11 g/L → Portal hypertension (cirrhosis, alcoholic hepatitis, Budd-Chiari, cardiac ascites)
• SAAG <11 g/L → Non-portal hypertensive (malignancy, TB peritonitis, nephrotic syndrome, pancreatic ascites, serositis)
Supportive Laboratory Investigations
Imaging
- Abdominal ultrasound with Doppler: Confirms the presence and volume of ascites, evaluates liver parenchyma (cirrhotic morphology), portal vein patency and flow direction, splenomegaly, and hepatic vein patency (excludes Budd-Chiari syndrome). MBS Item 55034.
- Echocardiography: Essential when cardiac ascites is considered and in assessment for TIPS candidacy (to exclude significant pulmonary hypertension, diastolic dysfunction, or heart failure).
- CT abdomen/pelvis: Useful if malignancy is suspected or for pre-TIPS anatomical assessment. Not a first-line investigation for uncomplicated cirrhotic ascites.
Differential Diagnosis of Ascites by SAAG
| SAAG ≥11 g/L (Portal Hypertensive) | SAAG <11 g/L (Non-Portal Hypertensive) |
|---|---|
| Cirrhosis (most common) | Peritoneal carcinomatosis |
| Alcoholic hepatitis | Tuberculous peritonitis |
| Budd-Chiari syndrome | Pancreatic ascites |
| Cardiac ascites | Nephrotic syndrome |
| Massive hepatic metastases | Serositis (SLE, vasculitis) |
Medical Management
Sodium Restriction
Dietary sodium restriction is the cornerstone of ascites management. The target is 80–90 mmol sodium per day, equivalent to approximately 5 g of table salt (NaCl). This is best achieved by avoiding added salt, processed foods, canned goods, and takeaway meals. A referral to a dietitian with experience in liver disease is recommended — patients commonly find this level of restriction difficult to maintain long-term.
Diuretic Therapy
Diuretics should be commenced once sodium restriction is initiated. The goal is to mobilise ascitic fluid through net negative sodium balance.
Weight Loss Targets & Monitoring
Medications to Avoid
- NSAIDs (ibuprofen, naproxen, diclofenac) — inhibit renal prostaglandin synthesis, precipitate renal failure, and antagonise diuretic response
- ACE inhibitors & ARBs — further reduce systemic vascular resistance, worsen effective circulating volume, and precipitate hypotension/renal failure
- Aminoglycosides — high nephrotoxicity risk in cirrhosis; use alternative antibiotics
- Iodinated contrast — use with extreme caution; ensure adequate hydration and consider alternative imaging if possible
Refractory Ascites
Refractory ascites develops in approximately 10% of patients with cirrhotic ascites and is defined by the inability to mobilise ascites with maximum-tolerated diuretic therapy or the development of diuretic-induced complications that preclude their continued use.
Definitions
| Type | Definition |
|---|---|
| Diuretic-resistant ascites | Unresponsive to sodium restriction (<90 mmol/day) and maximum-dose diuretics (spironolactone 400 mg/day + furosemide 160 mg/day) for at least 4 weeks, or inability to achieve >1.0 kg/day weight loss with adequate diuresis. |
| Diuretic-intractable ascites | Development of diuretic-induced complications — progressive renal impairment (hepatorenal syndrome), hyponatraemia (Na <120 mmol/L), hyperkalaemia (K⁺ >6.0 mmol/L), or hepatic encephalopathy — that mandate discontinuation or dose reduction of diuretics. |
Large-Volume Paracentesis (LVP)
LVP is the first-line treatment for refractory ascites and provides rapid symptomatic relief.
Transjugular Intrahepatic Portosystemic Shunt (TIPS)
TIPS creates a low-resistance channel between the portal vein and hepatic vein, reducing portal pressure and ascites formation. It is more effective than repeated LVP at controlling ascites but carries a higher risk of hepatic encephalopathy.
Patient Selection for TIPS
Other Therapies for Refractory Ascites
| Intervention | Indication & Notes |
|---|---|
| Midodrine | Alpha-1 agonist (2.5–12.5 mg PO TDS) — increases effective arterial blood volume as adjunct to diuretics or LVP; improves short-term outcomes. PBS: Not listed (private prescription). |
| Peritoneo-venous shunt (Denver shunt) | Rarely used due to high complication rates (DIC, shunt occlusion, infection). Consider only in patients who are not TIPS or transplant candidates and have recurrent symptomatic ascites. |
| Tunnelled peritoneal drain (PleurX® catheter) | Appropriate in palliative settings where repeated paracentesis is burdensome and TIPS/transplant is not indicated. Allows home drainage of ascites by the patient or carer. |
| Liver transplantation | Definitive treatment. The development of ascites is an indication for transplant evaluation. MELD score determines listing priority. Early referral to a transplant centre is essential. |
Early Transplant Referral
All patients with cirrhotic ascites should be referred to a liver transplant centre for assessment. Key indicators for urgent referral include:
- Refractory ascites (diuretic-resistant or diuretic-intractable)
- MELD score ≥15
- Hepatorenal syndrome (type 1 or type 2)
- Recurrent SBP (≥2 episodes)
- Recurrence of ascites after TIPS
- Progressive hepatic synthetic failure (Child-Pugh ≥10)
Australian liver transplant centres: Royal Prince Alfred Hospital (Sydney), Austin Hospital (Melbourne), Princess Alexandra Hospital (Brisbane), Sir Charles Gairdner Hospital (Perth), Royal Adelaide Hospital (Adelaide). Living donor liver transplant is available at selected centres and may reduce wait times.
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience chronic liver disease and cirrhosis at rates 3–5 times higher than non-Indigenous Australians. Alcohol-related liver disease and chronic hepatitis B (particularly in Northern Australia and remote communities) are the predominant causes of cirrhosis and ascites in this population. The AIHW reports that liver disease is among the top contributors to the gap in life expectancy.
📚 References
- 1. European Association for the Study of the Liver (EASL). EASL Clinical Practice Guidelines on the management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis. J Hepatol. 2010;53(3):397–417.
- 2. Runyon BA. Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline: management of adult patients with ascites due to cirrhosis 2012. Hepatology. 2013;57(4):1651–1653.
- 3. Adebayo D, Neong UP, Wong F. Refractory ascites in liver cirrhosis. Am J Gastroenterol. 2019;114(1):40–47.
- 4. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol. 2018;69(2):406–460.
- 5. Biggins SW, Angeli P, Garcia-Tsao G, et al. Diagnosis, evaluation, and management of ascites, spontaneous bacterial peritonitis and hepatorenal syndrome: 2021 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology. 2021;74(2):1014–1048.
- 6. Bureau C, Thabut D, Oberti F, et al. Transjugular intrahepatic portosystemic shunts with covered stents increase transplant-free survival of patients with cirrhosis and recurrent ascites. Gastroenterology. 2017;152(1):157–163.
- 7. Bernardi M, Caraceni P, Navickis RJ, Wilkes MM. Albumin infusion in patients undergoing large-volume paracentesis: a meta-analysis of randomized trials. Hepatology. 2012;55(4):1172–1181.
- 8. Australian Institute of Health and Welfare (AIHW). Chronic liver disease and cirrhosis. AIHW Bulletin 128. Canberra: AIHW; 2023.
- 9. Dwyer JM, Macdonald GA, O'Beirne J. Liver disease in Indigenous Australians. Med J Aust. 2021;214(8):355–360.
- 10. Moore KP, Aithal GP. Guidelines on the management of ascites in cirrhosis. Gut. 2006;55(Suppl 6):vi1–vi12.
- 11. Fernández J, Angeli P, Trebicka J, et al. Efficacy of albumin treatment for patients with cirrhosis and infections unrelated to spontaneous bacterial peritonitis. Clin Gastroenterol Hepatol. 2020;18(4):963–973.
- 12. National Hepatitis B Strategy 2023–2030. Australian Government Department of Health and Aged Care. Canberra; 2023.