📋 Key Information Summary
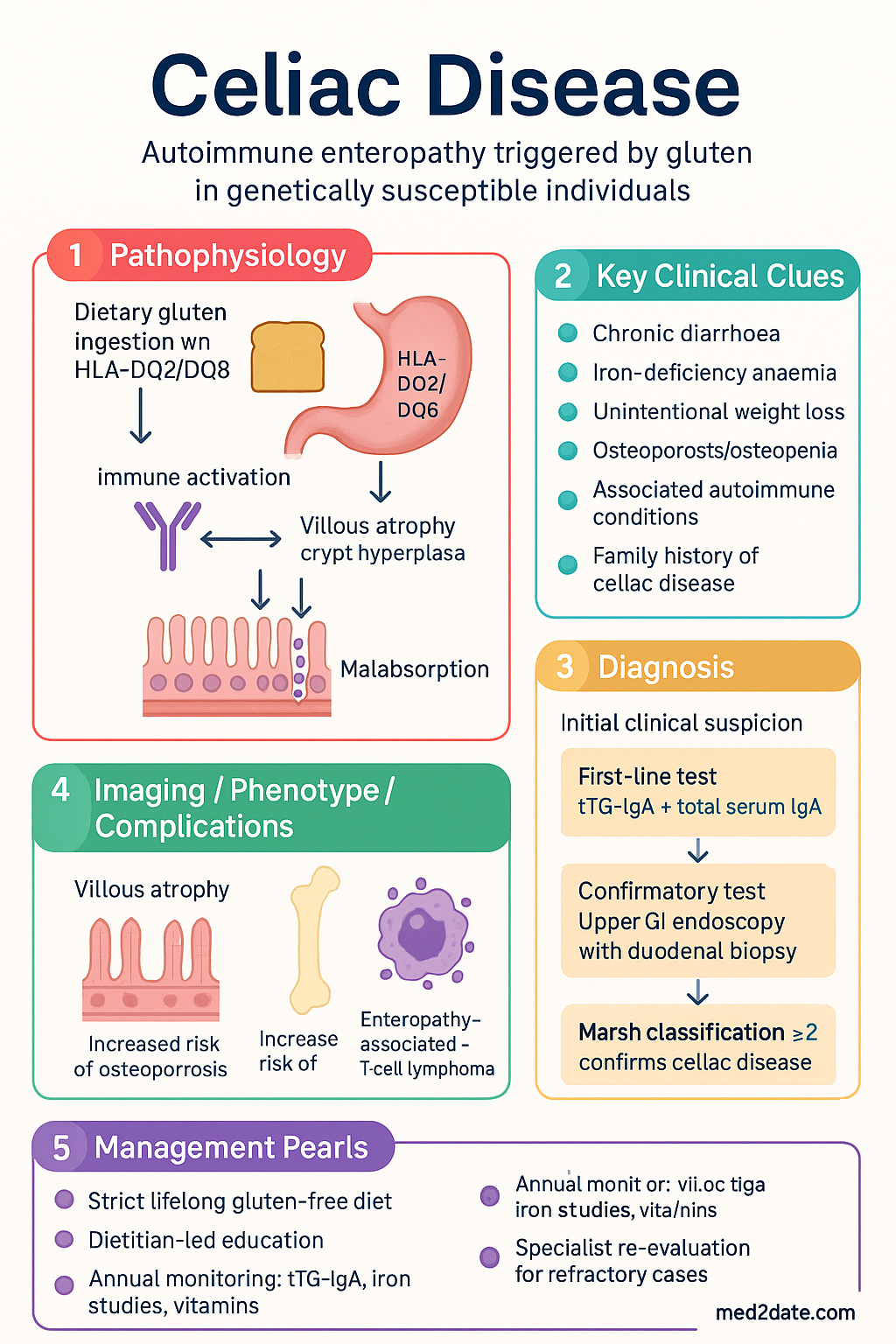
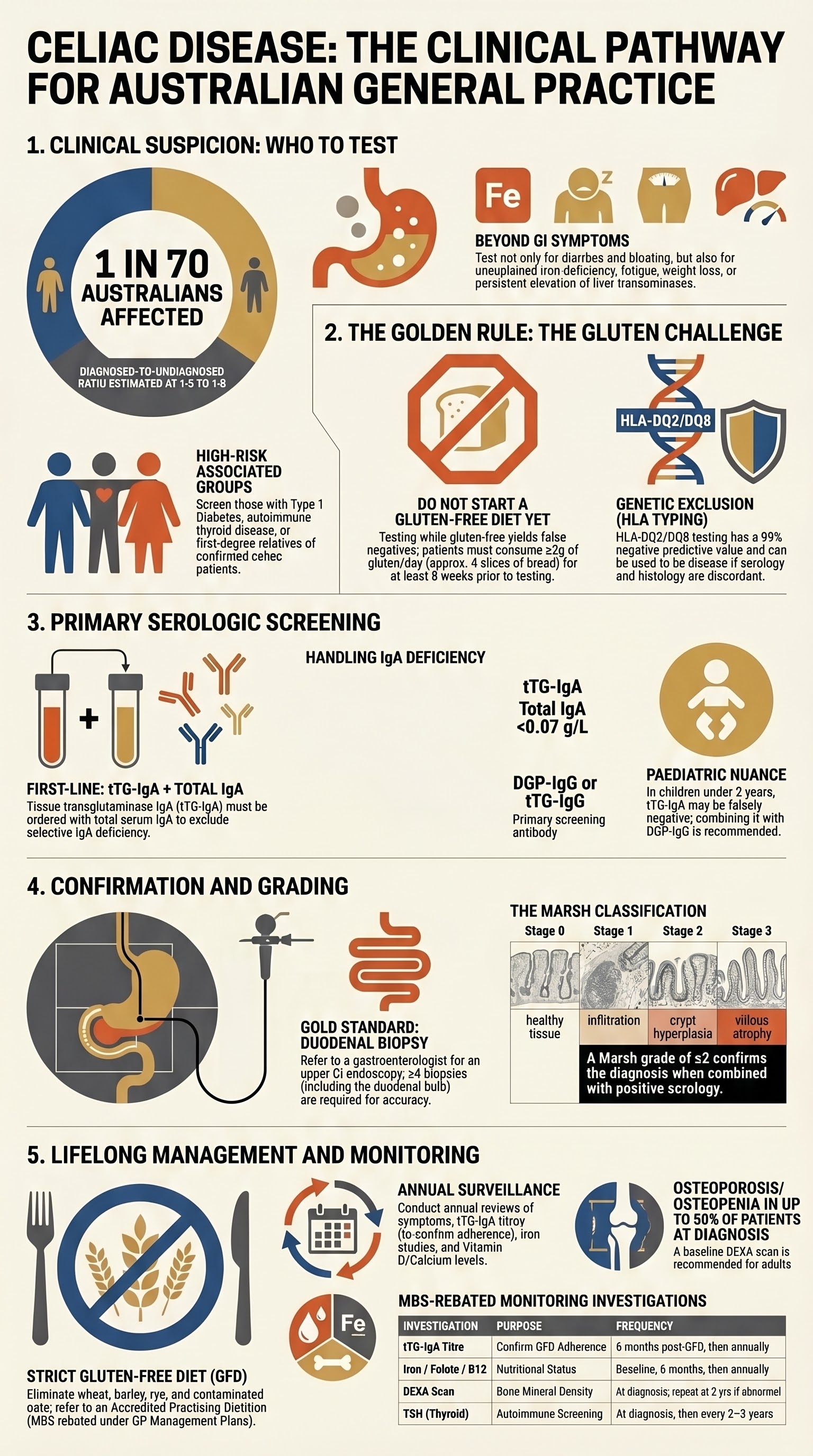
- Coeliac disease affects approximately 1 in 70 Australians, yet ~80% remain undiagnosed; it is a lifelong autoimmune enteropathy triggered by dietary gluten in genetically susceptible individuals (HLA-DQ2/DQ8).
- Test for coeliac disease in patients with chronic diarrhoea, unexplained iron-deficiency anaemia, unintentional weight loss, osteoporosis or osteopenia, unexplained persistent elevation of liver transaminases, and in those with associated autoimmune conditions (type 1 diabetes, autoimmune thyroid disease) or a first-degree family history.
- First-line serology is tissue transglutaminase IgA (tTG-IgA) combined with a total serum IgA level to exclude selective IgA deficiency — do not rely on a single test alone.
- If total IgA is deficient (<0.07 g/L), use deamidated gliadin peptide (DGP) IgG or tTG-IgG as the screening antibody; tTG-IgA will be falsely negative in IgA deficiency.
- Patients must be on a gluten-containing diet (≥2 g gluten/day for ≥6 weeks, ideally equivalent to ≥4 slices of bread daily) prior to serology and biopsy — testing while gluten-free yields false negatives.
- Positive serology requires confirmatory upper GI endoscopy with ≥4 duodenal biopsies (≥2 from the descending duodenum and ≥2 from the duodenal bulb) while the patient continues on gluten.
- Refer to a gastroenterologist for endoscopic confirmation; a Marsh classification ≥2 on histology, combined with positive serology, confirms coeliac disease.
- The only effective treatment is strict lifelong gluten-free diet (GFD), eliminating wheat, barley, rye, and contaminated oats; dietitian-led education is essential and is Medicare-rebated under GP Management Plans.
- Monitor annually: symptom review, tTG-IgA titre (falling titres confirm adherence), iron studies, folate, vitamin B12, vitamin D, calcium, zinc, and bone mineral density (DEXA) at baseline and as indicated.
- Refractory coeliac disease (RCD) — persistent symptoms and villous atrophy despite strict GFD for ≥12 months — warrants specialist re-evaluation, HLA typing, and exclusion of enteropathy-associated T-cell lymphoma.
- Aboriginal and Torres Strait Islander Australians may face barriers to diagnosis and dietary management including remote-living, limited dietitian access, and culturally inappropriate food labelling — proactive screening and supported follow-up are essential.
- Patients with coeliac disease have an increased risk of osteoporosis, enteropathy-associated T-cell lymphoma, small bowel adenocarcinoma, and other autoimmune diseases; long-term surveillance improves outcomes.
Introduction & Australian Epidemiology
Coeliac disease is a chronic immune-mediated enteropathy of the small intestine triggered by the ingestion of gluten (prolamins found in wheat, barley, and rye) in genetically predisposed individuals carrying HLA-DQ2 or HLA-DQ8 haplotypes. It is characterised by villous atrophy, crypt hyperplasia, and increased intraepithelial lymphocytes in the duodenal mucosa, leading to malabsorption and a wide spectrum of systemic manifestations.
In Australia, population-based screening studies estimate a prevalence of approximately 1 in 70 (≈1.4%) in the general population, though most cases remain undiagnosed. The Australian Coeliac Disease Epidemiology Study and the Busselton Health Study have confirmed that the diagnosed-to-undiagnosed ratio is roughly 1:5 to 1:8. This is consistent with global data showing that only 10–20% of affected individuals are clinically diagnosed.
Coeliac disease can present at any age and is equally prevalent in males and females, although diagnosed cases show a female predominance (~2:1). The median age at diagnosis in Australian adults is 40–50 years, with a second peak in the 60s. Paediatric presentation is most common between 6 months and 2 years, coinciding with the introduction of gluten-containing cereals.
The economic burden is substantial. Coeliac disease accounts for direct healthcare costs including specialist consultations, endoscopy, dietitian services, and gluten-free food costs (estimated at an additional AUD ,000–2,000 per year per household). The Australian Government partially subsidises gluten-free products under some state-based schemes, though no federal GST exemption currently applies to gluten-free foods nationally.
Who to Test
Given the high prevalence of undiagnosed coeliac disease in Australia, clinicians should maintain a high index of suspicion. Testing is recommended for the following groups, aligned with the Royal Australian College of General Practitioners (RACGP) and Gastroenterological Society of Australia (GESA) guidance:
Symptomatic Indications for Testing
Additional Indications
- Osteoporosis or osteopenia — especially in young adults or those without other risk factors; coeliac disease is found in up to 3–10% of patients with unexplained low bone mineral density.
- Unexplained raised transaminases — coeliac disease accounts for a proportion of otherwise unexplained chronic transaminitis (prevalence of coeliac disease in this group is 3–9%).
- Irritable bowel syndrome (IBS) — Australian and international data show 4–8% of patients meeting IBS criteria have undiagnosed coeliac disease; GESA recommends excluding coeliac disease before confirming an IBS diagnosis.
- Chronic fatigue — particularly when combined with other suggestive features.
Population Screening
Routine population screening of asymptomatic individuals is not currently recommended in Australia by GESA or RACGP. However, targeted case-finding in the high-risk groups listed above is strongly endorsed. For first-degree relatives, offer serologic testing at the time of the index case's diagnosis and repeat at intervals (every 2–3 years or if symptoms develop).
Serologic Testing
Serologic testing is the first-line investigation for coeliac disease in both adults and children. The choice of antibody depends on the patient's total IgA status.
Recommended First-Line Antibody Panel
| Test | When to Use | Sensitivity | Specificity | Notes |
|---|---|---|---|---|
| tTG-IgA (tissue transglutaminase IgA) | First-line screening in IgA-sufficient patients | 95–98% | 95–98% | Best single test; available through all Australian pathology providers (MBS item 69500 series). Use human recombinant tTG antigen. |
| Total serum IgA | Mandatory companion test with tTG-IgA | N/A (quantitative) | N/A | Selective IgA deficiency occurs in 1:300–1:700 coeliac patients (vs 1:600 general population). IgA <0.07 g/L = deficiency. |
| DGP IgG (deamidated gliadin peptide IgG) | Patients with selective IgA deficiency | 80–95% | 90–98% | Preferred second-line test when IgA is deficient. Superior to older gliadin antibody assays. |
| tTG-IgG | Alternative in IgA deficiency if DGP unavailable | 80–90% | 90–95% | Less sensitive than DGP IgG for IgA-deficient patients but acceptable alternative. |
| EMA IgA (endomysial antibody IgA) | Confirmatory test (second-line); near 100% specificity | 85–95% | 99–100% | Immunofluorescence-based; operator-dependent. Used to strengthen diagnostic certainty when tTG-IgA is weakly positive. |
Interpretive Algorithm
Paediatric Considerations — Potential Biopsy-Free Diagnosis
The European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) 2020 criteria, which are increasingly adopted in Australian paediatric practice, allow a biopsy-free diagnosis in symptomatic children when ALL of the following are met: (1) tTG-IgA ≥10× upper limit of normal, (2) EMA IgA positive on a separate sample, (3) HLA-DQ2 or DQ8 positive, and (4) symptoms resolve on GFD. Confirmation by a paediatric gastroenterologist is still recommended.
Confirmatory Biopsy & Referral
In Australia, upper gastrointestinal endoscopy (gastroscopy) with duodenal biopsy remains the gold standard for confirming coeliac disease in adults and most children. This should be performed by a gastroenterologist or specialist endoscopist.
Endoscopic Biopsy Protocol
- Minimum biopsies: ≥4 duodenal biopsies total — at least 2 from the distal descending (2nd part) duodenum and at least 2 from the duodenal bulb. This is because villous atrophy may be patchy, and bulbar disease can be the sole site of involvement.
- Orientation and processing: Specimens should be oriented on filter paper and sent in formalin for haematoxylin–eosin staining; CD3 immunohistochemistry for intraepithelial lymphocyte (IEL) quantification is recommended.
- Ongoing gluten intake: The patient must continue consuming gluten until the biopsy is obtained. A minimum of 2 g gluten/day (approximately 4 slices of bread) for ≥6 weeks prior to endoscopy is recommended. Initiating GFD before biopsy is the most common cause of diagnostic uncertainty.
Marsh Classification of Duodenal Histology
| Marsh Grade | IELs (per 100 enterocytes) | Crypt Hyperplasia | Villous Architecture | Interpretation |
|---|---|---|---|---|
| Marsh 0 | <25 | Normal | Normal | Normal mucosa |
| Marsh 1 | ≥25 (increased IELs) | Normal | Normal | Infiltrative — non-specific; may be seen in H. pylori, NSAIDs, other causes |
| Marsh 2 | ≥25 | Increased | Normal | Infiltrative–hyperplastic — consistent with coeliac disease when combined with positive serology |
| Marsh 3a | ≥25 | Increased | Mild partial villous atrophy | Diagnostic of coeliac disease (with positive serology) |
| Marsh 3b | ≥25 | Increased | Subtotal villous atrophy | Diagnostic of coeliac disease |
| Marsh 3c | ≥25 | Increased | Total villous atrophy | Diagnostic of coeliac disease — severe |
Referral Pathway in Australia
- Urgent GI referral if serology strongly positive (tTG-IgA >10× ULN) with classic symptoms — particularly in children per ESPGHAN criteria.
- Routine GI referral for confirmatory biopsy in all patients with positive serology. Public hospital gastroenterology waiting times vary (4–12 weeks in metropolitan areas, longer in regional/rural). Private referral may be faster.
- Telehealth GI consultation is increasingly available (MBS telehealth items) for regional and remote patients, though endoscopy still requires procedural access.
- HLA-DQ2/DQ8 typing (MBS-rebated) is useful when there is diagnostic uncertainty: a negative result effectively excludes coeliac disease. Available through major Australian pathology providers.
When Biopsy May Not Be Required
In selected paediatric patients meeting ESPGHAN 2020 non-biopsy criteria (as above) and in some adult clinical scenarios, a biopsy-free pathway may be considered in consultation with a gastroenterologist. However, in Australian practice, biopsy confirmation remains the standard approach for adults and is recommended by GESA.
Differential Diagnosis to Consider
- Small intestinal bacterial overgrowth (SIBO)
- Giardiasis
- Autoimmune enteropathy
- Crohn's disease (duodenal involvement)
- Tropical sprue
- Eosinophilic gastroenteritis
- Drug-induced villous atrophy (olmesartan, mycophenolate, NSAIDs, checkpoint inhibitors)
- Common variable immunodeficiency (CVID)
Long-Term Management
The cornerstone of coeliac disease management is strict lifelong adherence to a gluten-free diet (GFD). There are currently no approved pharmacological therapies for coeliac disease in Australia, although clinical trials of gluten-degrading enzymes, tight-junction modulators, and immunotherapy approaches are underway.
Gluten-Free Diet — Core Principles
- Eliminate: Wheat, barley, rye, and their derivatives (including spelt, kamut, triticale). Standard oats are also excluded in Australia due to significant cross-contamination risk, although pure uncontaminated oats (<20 ppm gluten) remain debated — GESA recommends individual assessment and discussion with a dietitian.
- Safe grains/starches: Rice, corn (maize), potato, quinoa, buckwheat, millet, sorghum, amaranth, tapioca, certified gluten-free oats (where tolerated).
- Labelling: The Australia New Zealand Food Standards Code (Standard 1.2.3) requires mandatory declaration of gluten-containing cereals. "Gluten-free" labelling requires <20 ppm gluten (AOAC or Codex method). The Coeliac Australia endorsement logo (crossed grain) provides additional consumer assurance.
- Hidden gluten sources: Soy sauce (use tamari), beer/lager (use gluten-free beer), stock cubes, processed meats, some medications (starch excipients — generally wheat starch is now highly processed and considered safe in some European countries, but Australian guidelines recommend caution), communion wafers.
Monitoring Framework
| Parameter | Frequency | Details |
|---|---|---|
| Symptom review | 3–6 months post-diagnosis, then annually | Gastrointestinal symptoms, energy levels, weight |
| tTG-IgA titre | 6 months post-GFD, then annually until normalised | Declining titres confirm GFD adherence; normalisation expected in 6–12 months. Persistent elevation → assess adherence or consider refractory disease. |
| Iron studies | At diagnosis, 6 months, then annually | Ferritin, transferrin saturation. Iron deficiency may persist for months despite GFD. |
| Folate, vitamin B12 | At diagnosis, then annually | Deficiency common at diagnosis, particularly proximal small bowel involvement. |
| Vitamin D, calcium | At diagnosis, then annually | Vitamin D deficiency is prevalent in Australian coeliac patients; supplementation often required. |
| Zinc | At diagnosis, then as needed | Zinc malabsorption may contribute to dermatological symptoms and impaired wound healing. |
| Thyroid function (TSH) | At diagnosis, then every 2–3 years | Autoimmune thyroiditis co-occurs in 10–30% of coeliac patients. |
| Bone mineral density (DEXA) | At diagnosis (adults); repeat at 2 years if abnormal; ongoing per risk | Osteoporosis/osteopenia present in up to 40–50% at diagnosis. Improvement expected with GFD but may be incomplete. |
| Liver function tests | At diagnosis, then as indicated | Elevated transaminases normalise in most patients with GFD adherence. |
Nutritional Supplementation
Many patients require temporary or ongoing supplementation due to malabsorption at diagnosis or ongoing micronutrient gaps:
GFD Non-Response and Refractory Coeliac Disease
Investigations
Available Investigations in Australia
Special Populations
Paediatrics
Pregnancy
Elderly
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health Considerations
The prevalence of coeliac disease in Aboriginal and Torres Strait Islander Australians is not well characterised, but available evidence suggests it is under-diagnosed. HLA-DQ2 haplotype frequency in Indigenous Australians is lower than in European-descent populations, suggesting potentially lower genetic susceptibility; however, coeliac disease does occur and may present atypically or be masked by other causes of malabsorption, chronic diarrhoea, and nutritional deficiency that are more prevalent in remote communities.
Quick Reference — Coeliac Disease Diagnostic & Monitoring Summary
📚 References
- 1. Gastroenterological Society of Australia (GESA). Coeliac disease: clinical update and practical guide. J Gastroenterol Hepatol. 2023;38(Suppl 1):1–28.
- 2. Singh P, Arora A, Strand TA, et al. Global prevalence of celiac disease: systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2018;16(6):823–836.e2.
- 3. Husby S, Koletzko S, Korponay-Szabó IR, et al. European Society for Paediatric Gastroenterology, Hepatology and Nutrition guidelines for the diagnosis of coeliac disease 2020. J Pediatr Gastroenterol Nutr. 2020;70(1):141–156.
- 4. Al-Toma A, Volta U, Auricchio R, et al. European Society for the Study of Coeliac Disease (ESsCD) guideline for coeliac disease and other gluten-related disorders. United European Gastroenterol J. 2019;7(5):583–613.
- 5. Ludvigsson JF, Leffler DA, Bai JC, et al. The Oslo definitions for coeliac disease and related terms. Gut. 2013;62(1):43–52.
- 6. Downey L, Houten R, Murch S, Longson D. Recognition, assessment, and management of coeliac disease: summary of updated NICE guidance. BMJ. 2015;351:h4513.
- 7. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework 2023. Canberra: AIHW; 2023.
- 8. Coeliac Australia. Coeliac disease: the facts. Available at: www.coeliac.org.au. Accessed 2024.
- 9. Lebwohl B, Sanders DS, Green PHR. Coeliac disease. Lancet. 2018;391(10115):70–81.
- 10. Rubio-Tapia A, Hill ID, Kelly CP, Calderwood AH, Murray JA. ACG clinical guidelines: diagnosis and management of celiac disease. Am J Gastroenterol. 2013;108(5):656–676.
- 11. Lionetti E, Francavilla R, Pavone P, et al. The neurology of coeliac disease in childhood: what is the evidence? A systematic review and meta-analysis. Dev Med Child Neurol. 2010;52(8):700–707.
- 12. RACGP. Guidelines for preventive activities in general practice (Red Book). 9th edition. Melbourne: RACGP; 2016.
- 13. Biesiekierski JR, Newnham ED, Shepherd SJ, et al. Characterization of adults with a self-diagnosis of nonceliac gluten sensitivity. Nutr Clin Pract. 2014;29(1):54–61.
- 14. Daum S, Cellier C, Mulder CJ. Refractory coeliac disease. Best Pract Res Clin Gastroenterol. 2005;19(3):413–424.
- 15. Food Standards Australia New Zealand (FSANZ). Standard 1.2.3 — Information Requirements — Food for Sale. Australia New Zealand Food Standards Code. Canberra: FSANZ; 2023.