📋 Key Information Summary
- Hepatitis B (HBV) and hepatitis C (HCV) are leading causes of cirrhosis, hepatocellular carcinoma (HCC), and liver-related mortality in Australia — most infected individuals remain undiagnosed.
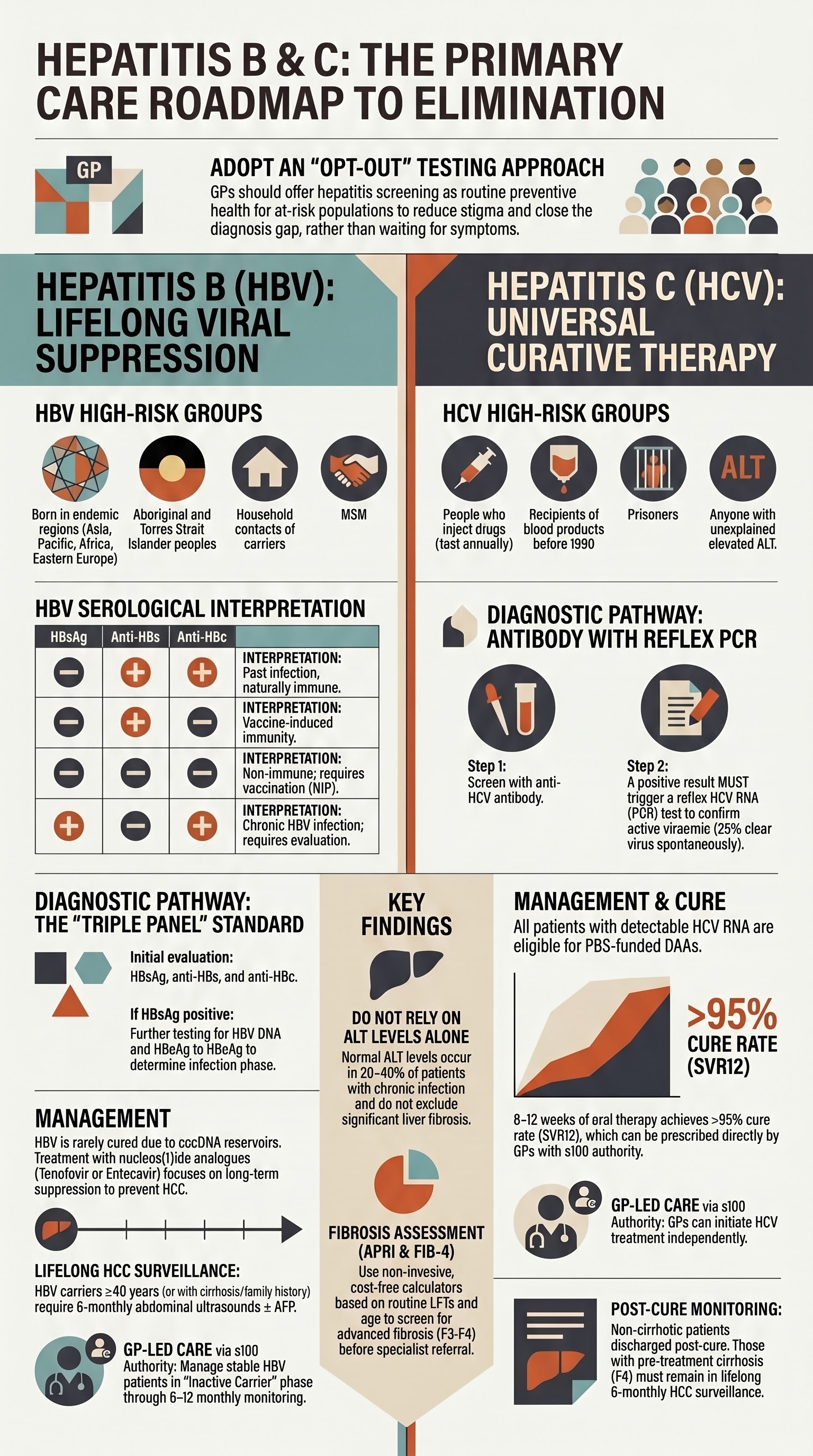
- HBV screening is recommended for all people born in endemic regions (Asia, Pacific Islands, sub-Saharan Africa, Eastern Europe), Aboriginal and Torres Strait Islander peoples, people who inject drugs (PWID), men who have sex with men (MSM), prisoners, HIV/HCV co-infected individuals, dialysis patients, pregnant women, and household/sexual contacts of known carriers.
- HCV screening is recommended for all PWID (test at least annually), recipients of blood products before February 1990, people on haemodialysis, people with HIV, prisoners, children born to HCV-positive mothers, and anyone with unexplained elevated ALT.
- Initial HBV evaluation uses a serological panel: HBsAg, anti-HBs, anti-HBc (± HBeAg/anti-HBe, HBV DNA). HCV screening uses anti-HCV antibody with reflex HCV PCR (RNA) to confirm active infection.
- All patients with confirmed HBV or HCV infection require LFTs, full blood count, coagulation studies, and fibrosis assessment (APRI score, FIB-4, or transient elastography).
- HCV is now curable in >95% of cases with 8–12 weeks of direct-acting antivirals (DAAs) — treatment is PBS-listed and can be initiated by GPs with s100 authority.
- HBV is rarely cured but can be effectively suppressed with long-term nucleos(t)ide analogues (tenofovir or entecavir); treatment decisions require specialist input.
- All newly diagnosed HBV/HCV patients must be linked to a hepatologist, gastroenterologist, or infectious disease specialist for antiviral eligibility assessment and long-term HCC surveillance planning.
- Vaccinate all susceptible household and sexual contacts of HBV carriers against hepatitis B (HBV vaccine is funded under the NIP).
- No HCV vaccine exists — harm-reduction counselling (needle exchange, safe injecting practices) is essential for PWID to prevent reinfection and onward transmission.
- Aboriginal and Torres Strait Islander peoples have significantly higher rates of HBV and HCV — proactive, culturally safe screening in primary care and correctional settings is critical to closing the gap.
- HBV-positive patients require lifelong HCC surveillance with 6-monthly abdominal ultrasound ± AFP, even if not on antiviral therapy.
Introduction & Australian Epidemiology
Hepatitis B virus (HBV) and hepatitis C virus (HCV) are the most common chronic blood-borne viral infections in Australia. Together they account for the majority of chronic liver disease, cirrhosis, and hepatocellular carcinoma (HCC) nationally. Despite the availability of an effective HBV vaccine and curative HCV therapies, both infections remain significantly underdiagnosed and undertreated in the Australian population.
Primary care plays a central role in hepatitis elimination. The Australian Government has committed to the WHO targets of eliminating viral hepatitis as a public health threat by 2030, requiring a substantial scale-up of testing, linkage to care, and treatment in general practice settings.
Hepatitis B in Australia
- An estimated 223,000–300,000 people are living with chronic HBV in Australia (prevalence ~1%).
- Approximately 38–50% remain undiagnosed.
- The most affected populations include people born in endemic countries (China, Vietnam, Philippines, Korea, sub-Saharan Africa, Pacific Islands), Aboriginal and Torres Strait Islander peoples, and people with a history of injecting drug use.
- Mother-to-child transmission (MTCT) remains the most important route in endemic populations; sexual and percutaneous transmission predominate in Australian-born populations.
- HBV-related HCC incidence is increasing and is now the fastest-rising cause of cancer death in Australian males.
- The NIP funds HBV vaccination for all infants (since 2000), catch-up for adolescents, and for high-risk adults (Aboriginal and Torres Strait Islander peoples from 15 years, PWID, MSM, household contacts, dialysis patients, healthcare workers).
Hepatitis C in Australia
- An estimated 115,000–175,000 people are living with chronic HCV; approximately 20% remain undiagnosed.
- Over 90% of new HCV infections in Australia are acquired through sharing of injecting equipment among PWID.
- Since the introduction of PBS-funded DAAs in March 2016, over 100,000 Australians have been treated and cured, but treatment uptake has plateaued since 2020.
- Reinfection rates among PWID are 2–8% per year, underscoring the need for ongoing harm-reduction services post-cure.
- HCV-related cirrhosis and HCC remain significant causes of liver transplant and liver-related mortality.
Screening Indications
Screening for HBV and HCV should be offered proactively to individuals meeting defined risk criteria. Testing should be framed as routine and non-stigmatizing — a standard part of preventive healthcare rather than an indicator of assumed behaviour.
Who to Screen for Hepatitis B
The following groups should be tested for HBsAg, anti-HBs, and anti-HBc (the "HBV triple panel"):
| Risk Category | Details |
|---|---|
| Country of origin | All people born in HBV-endemic regions: East and Southeast Asia (China, Vietnam, Philippines, Cambodia, Korea), Pacific Islands (PNG, Fiji, Samoa, Tonga), sub-Saharan Africa, Central/South America, Middle East, Eastern Europe, Central Asia. HBV prevalence ≥2% in country of birth warrants testing. |
| Aboriginal and Torres Strait Islander peoples | Particularly those from remote and very remote communities in the NT, WA, and QLD where HBV prevalence is 3–6× the national average. Offer HBV serology as part of Adult Health Checks (MBS Item 715). |
| People who inject drugs (PWID) | Current or past injecting drug use — high prevalence of both HBV and HCV co-infection. Include those on opioid substitution therapy. |
| Men who have sex with men (MSM) | Higher rates of HBV acquisition through sexual transmission. |
| Household and sexual contacts of HBV carriers | Test for HBsAg, anti-HBs, anti-HBc; vaccinate if non-immune. |
| Pregnant women | HBsAg testing is recommended for all pregnancies (funded in most states/territories). Essential to identify candidates for neonatal immunoprophylaxis to prevent MTCT. |
| Haemodialysis patients | Screen at dialysis commencement and periodically (every 6–12 months). |
| Immunosuppression candidates | Prior to chemotherapy, biologics (anti-TNF, rituximab), or corticosteroid courses — risk of HBV reactivation. |
| HIV-positive individuals | Co-infection is common; test at HIV diagnosis and if unvaccinated. |
| Correctional facility inmates | High prevalence of HBV (and HCV); offer screening on reception. |
| Recipients of blood/tissue before 1990 | Prior to universal screening of blood products in Australia. |
Who to Screen for Hepatitis C
| Risk Category | Details |
|---|---|
| People who inject drugs (PWID) | Current or past injecting drug use — test at least annually; re-test every 6–12 months if ongoing risk. This is the single largest risk group in Australia. |
| Recipients of blood products before February 1990 | Before HCV screening of the Australian blood supply commenced. |
| Recipients of unscreened tissue/organs | Including those who received organs or tissues before HCV testing was routine. |
| Haemodialysis patients | Screen at commencement and every 6 months. |
| People living with HIV | Particularly MSM with HIV — rising incidence of sexually transmitted HCV in this population. |
| Children born to HCV-positive mothers | Maternal antibodies persist until 18 months; HCV PCR testing from 3 months of age, or anti-HCV after 18 months. |
| Inmates of correctional facilities | HCV prevalence 20–40% in Australian prisons. |
| Unexplained elevated ALT | Persistently elevated ALT after excluding alcohol, metabolic dysfunction-associated steatotic liver disease (MASLD), autoimmune, and drug causes. |
| Tattooing / body piercing in unregulated settings | Especially in correctional settings or overseas. |
MBS Item Numbers for Screening
- MBS Item 715 — Aboriginal and Torres Strait Islander Adult Health Check (includes viral hepatitis screening as a recommended component).
- MBS Item 69330 — Hepatitis B serology (HBsAg, anti-HBs, anti-HBc).
- MBS Item 69335 — Hepatitis C antibody.
- MBS Item 69345 — Hepatitis C RNA / PCR.
- MBS Item 721 / 723 — GP Management Plan / Team Care Arrangement — useful for chronic HBV patients requiring ongoing monitoring.
Initial Evaluation
Once a patient is identified as HBV or HCV seropositive, a structured initial evaluation is required to determine infection status, disease phase, degree of liver injury, and eligibility for antiviral therapy or specialist referral.
Hepatitis B — Serological Panel Interpretation
The initial HBV evaluation requires a "triple panel" plus supplementary tests:
| Test | MBS Item | Interpretation |
|---|---|---|
| HBsAg | 69330 | Positive = current infection (acute or chronic). Negative = no active infection. |
| Anti-HBs | 69330 | Positive (≥10 IU/L) = immune (vaccine-induced or natural). Negative = non-immune — consider vaccination. |
| Anti-HBc (total) | 69330 | Positive = past or current exposure. Negative = never infected. Isolated anti-HBc positivity may indicate resolved infection with waning anti-HBs, occult HBV, or false positive — check HBV DNA. |
| HBeAg | 69332 | Positive = active viral replication, high infectivity (immune-active or immune-tolerant phase). Negative = lower replication (may be immune-control or pre-core mutant). |
| Anti-HBe | 69332 | Positive = seroconversion (immune-control phase). Usually accompanies HBeAg loss. |
| HBV DNA (viral load) | 69342 | Quantitative PCR. Key for determining infection phase and treatment eligibility. >2,000 IU/mL generally indicates significant viral replication; >20,000 IU/mL typical of immune-active phase. |
| HBV genotype | 69342 | Useful for treatment planning (not always required). Genotype C predominant in Asian-born patients; genotype D in European/Middle Eastern; genotype A/C in ATSI communities. |
Interpreting the HBV Triple Panel — Common Patterns
| HBsAg | Anti-HBs | Anti-HBc | Interpretation |
|---|---|---|---|
| − | + | + | Past infection, immune. No further action unless immunosuppressed (check HBV DNA to exclude occult HBV). |
| − | + | − | Vaccine-induced immunity. Protected. |
| − | − | − | Non-immune, never infected. Vaccinate. |
| − | − | + | Isolated anti-HBc. Possible: resolved infection with waning anti-HBs, occult HBV, or false positive. Check HBV DNA; vaccinate if at ongoing risk. |
| + | − | + | Chronic HBV infection. Requires further evaluation (HBeAg, HBV DNA, LFTs, fibrosis assessment) and specialist referral. |
| + | − | − | Acute HBV (early). Rare in primary care — check IgM anti-HBc to distinguish from chronic. |
Hepatitis C — Antibody with Reflex PCR
HCV screening follows a two-step process:
Liver Function Tests (LFTs) & Baseline Bloods
For all patients with confirmed HBV or HCV infection, request:
- Liver function tests: ALT, AST, GGT, ALP, bilirubin, albumin — ALT is the most sensitive marker of hepatic inflammation in viral hepatitis.
- Full blood count (FBC): Low platelets may indicate advanced fibrosis/cirrhosis (portal hypertension).
- Coagulation studies: INR — elevated INR with low albumin suggests decompensated liver disease.
- Renal function (eGFR): Required before tenofovir (HBV) — nephrotoxic risk.
- HIV serology: All HBV/HCV-positive patients should be tested for HIV co-infection.
- Hepatitis A serology: Test for HAV IgG; vaccinate if non-immune (HAV superinfection in chronic liver disease carries high mortality).
- AFP: Baseline alpha-fetoprotein (useful for HCC surveillance but not diagnostic alone).
Fibrosis Assessment
Staging liver fibrosis is essential for prognosis and treatment decisions. Available tools in primary care:
Pathophysiology
Hepatitis B
HBV is a partially double-stranded DNA virus (Hepadnaviridae family) that infects hepatocytes via the sodium taurocholate co-transporting polypeptide (NTCP) receptor. It replicates through an RNA intermediate (reverse transcriptase), resulting in the formation of covalently closed circular DNA (cccDNA) in the hepatocyte nucleus — a stable episomal reservoir that persists for the life of the cell and explains why HBV is rarely "cured" even after HBsAg loss.
Liver damage in HBV is predominantly immune-mediated — the virus itself is not directly cytopathic. Cytotoxic T lymphocyte (CTL) activity against infected hepatocytes drives hepatic inflammation and fibrosis. The balance between viral replication (immune-tolerant phase) and host immune clearance (immune-active phase) determines disease progression.
Natural History Phases of Chronic HBV
| Phase | HBeAg | HBV DNA | ALT | Liver Histology |
|---|---|---|---|---|
| Immune-tolerant | + | Very high (>10⁷ IU/mL) | Normal | Minimal inflammation/fibrosis |
| Immune-active (HBeAg+) | + | High (10⁴–10⁷ IU/mL) | Elevated (flares) | Moderate–severe inflammation, progressive fibrosis |
| Inactive carrier | − | Low (<2,000 IU/mL) | Normal | Variable — may have residual fibrosis |
| HBeAg-negative chronic hepatitis | − | Moderate–high (>2,000 IU/mL) | Elevated (fluctuating) | Active inflammation, progressive fibrosis — pre-core/basal core promoter mutants |
| HBsAg-negative (functional cure) | − | Undetectable (or very low cccDNA) | Normal | Resolved; may have residual fibrosis; HCC risk persists if cirrhosis was present |
Hepatitis C
HCV is a single-stranded RNA virus (Flaviviridae family) with 7 genotypes and >80 subtypes. It replicates in the cytoplasm of hepatocytes using the NS5B RNA-dependent RNA polymerase. Unlike HBV, HCV has no nuclear reservoir and no cccDNA equivalent — hence the possibility of complete virological cure (SVR).
HCV causes both direct cytopathic injury (via viral proteins and lipid metabolism disruption) and immune-mediated hepatocyte destruction. Chronic infection leads to progressive hepatic fibrosis over 20–30 years, with 10–20% of untreated patients developing cirrhosis. Established cirrhosis confers a 1–5% annual risk of HCC. Extrahepatic manifestations (mixed cryoglobulinaemia, membranoproliferative glomerulonephritis, porphyria cutanea tarda, non-Hodgkin lymphoma) are driven by chronic immune stimulation.
Clinical Presentation & Diagnostic Criteria
Acute Hepatitis B
- Incubation 45–160 days (mean 90 days).
- 70% of adults have subclinical or anicteric illness; 30% present with jaundice, malaise, nausea, RUQ pain, and hepatomegaly.
- Fulminant hepatic failure occurs in <1% — higher risk with HBV/HDV co-infection.
- Diagnosis: HBsAg+ and IgM anti-HBc+ (distinguishes acute from chronic flares).
- 95–99% of immunocompetent adults clear acute HBV spontaneously → HBsAg loss by 6 months.
Chronic Hepatitis B
- Most patients are asymptomatic for decades — detected only through screening.
- Non-specific symptoms when present: fatigue, RUQ discomfort, anorexia.
- Signs of advanced disease/cirrhosis: spider naevi, palmar erythema, jaundice, ascites, hepatosplenomegaly, gynaecomastia, caput medusae.
- Diagnosis: HBsAg positive for >6 months (or HBsAg+ on a single occasion with no clinical context suggesting acute infection, given most chronic carriers are asymptomatic).
Acute Hepatitis C
- Incubation 2–12 weeks (mean 6–7 weeks).
- 80% of cases are asymptomatic — rarely diagnosed in the acute phase.
- When symptomatic: mild fatigue, jaundice (uncommon), elevated ALT (often >10× ULN).
- Spontaneous clearance occurs in ~25% of acute infections (higher in females, IL28B CC genotype, symptomatic presentation).
Chronic Hepatitis C
- 75% of acute HCV infections become chronic.
- Most patients are asymptomatic for years to decades.
- Non-specific symptoms: fatigue, cognitive difficulties ("brain fog"), arthralgia, depression.
- Extrahepatic manifestations: mixed cryoglobulinaemia (vasculitis, purpura, arthralgia), membranoproliferative GN, porphyria cutanea tarda, type 2 diabetes (increased risk), B-cell non-Hodgkin lymphoma.
- Signs of cirrhosis as per HBV above.
- Diagnosis: anti-HCV positive + HCV RNA positive (PCR).
Investigations
Summary of investigations for patients with confirmed HBV or HCV infection, including Australian availability and MBS funding:
Risk Stratification & Severity Assessment
Hepatitis B Risk Stratification
The decision to treat chronic HBV is based on a combination of HBV DNA level, ALT, fibrosis stage, age, family history of HCC, and pregnancy status. Stratification guides urgency of specialist referral:
Hepatitis C — Treatment is Universal
Unlike HBV, all patients with detectable HCV RNA are eligible for DAA treatment — there are no ALT, fibrosis, or viral load thresholds required. The goal is universal treatment to achieve micro-elimmination. However, fibrosis staging remains important for:
- Determining treatment urgency (F3–F4 treated preferentially).
- Guiding DAA regimen duration (some regimens require 16 weeks for F4 or prior treatment failure).
- Post-SVR surveillance planning — patients with pre-treatment cirrhosis retain HCC risk and require lifelong 6-monthly surveillance.
| Fibrosis Stage | APRI | FIB-4 | FibroScan (KPa) | Treatment Urgency |
|---|---|---|---|---|
| F0–F1 (None–Mild) | <0.5 | <1.45 | <7.0 | Treat to prevent onward transmission and long-term complications |
| F2 (Moderate) | 0.5–1.5 | 1.45–3.25 | 7.0–9.5 | Treat promptly — fibrosis progressing |
| F3 (Severe) | >1.0 | >2.67 | 9.5–12.5 | Treat urgently — high risk of progression to cirrhosis |
| F4 (Cirrhosis) | >1.5 | >3.25 | >12.5 | Treat urgently — lifelong HCC surveillance required post-SVR |
Directed / Pathogen-Specific Therapy
Hepatitis C — Direct-Acting Antivirals (DAAs)
All Australians with chronic HCV (HCV RNA positive) are eligible for PBS-funded DAA treatment. Treatment is initiated by GPs (with s100 authority) or specialists. The choice of regimen depends on genotype, fibrosis stage, prior treatment history, and renal function.
Hepatitis B — Nucleos(t)ide Analogues
Treatment of chronic HBV is initiated by or in consultation with a hepatologist, gastroenterologist, or infectious disease specialist. The goal is viral suppression (HBV DNA undetectable), not cure — long-term (often indefinite) therapy is required. First-line agents are:
HBV Treatment Indications (Summary for Referral)
| Indication for Treatment | Criteria |
|---|---|
| Cirrhosis | Any HBsAg+ patient with cirrhosis, regardless of HBV DNA or ALT — treat immediately |
| Immune-active HBeAg+ chronic hepatitis | HBV DNA >20,000 IU/mL AND ALT >2× ULN persisting >3–6 months |
| HBeAg-negative chronic hepatitis | HBV DNA >2,000 IU/mL AND ALT >1× ULN persisting >3–6 months |
| Family history of HCC | Lower thresholds for treatment — discuss with specialist even with normal ALT |
| Extrahepatic manifestations | Polyarteritis nodosa, HBV-associated GN |
| Immunosuppression planned | Prophylactic antiviral before and during immunosuppressive therapy (chemotherapy, biologics, high-dose corticosteroids) to prevent reactivation |
| Pregnancy — high viral load | HBV DNA >200,000 IU/mL in 3rd trimester — tenofovir from 28–32 weeks gestation to prevent MTCT |
HBV Vaccination for Non-Immune Contacts
All susceptible (anti-HBs <10 IU/L) household and sexual contacts of HBV carriers should receive hepatitis B vaccination:
If a non-immune sexual contact of an HBV carrier presents within 72 hours of a high-risk exposure, consider hepatitis B immunoglobulin (HBIG) in addition to commencing vaccination.
Monitoring
Chronic Hepatitis B — Long-Term Monitoring
Hepatitis C — Post-Treatment Monitoring
Special Populations
Pregnancy
Paediatrics
Elderly
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health
📚 References
- 1. Australian Government Department of Health and Aged Care. National Hepatitis B Strategy 2023–2030. Canberra: Commonwealth of Australia; 2023.
- 2. Australian Government Department of Health and Aged Care. National Hepatitis C Strategy 2023–2030. Canberra: Commonwealth of Australia; 2023.
- 3. The Kirby Institute. HIV, Viral Hepatitis and Sexually Transmissible Infections in Australia: Annual Surveillance Report 2023. Sydney: UNSW; 2023.
- 4. Terrault NA, Lok ASF, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology. 2018;67(4):1560–1599.
- 5. European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol. 2017;67(2):370–398.
- 6. Pawlotsky JM, Negro F, Aghemo A, et al. EASL recommendations on treatment of hepatitis C: Final update of the series. J Hepatol. 2020;73(5):1170–1218.
- 7. AASLD-IDSA. Recommendations for Testing, Managing, and Treating Hepatitis C. Accessed at hcvguidelines.org. Updated 2024.
- 8. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework: Hepatitis B and C. AIHW Canberra; 2023.
- 9. National Aboriginal Community Controlled Health Organisation (NACCHO). Communicable Diseases in Aboriginal and Torres Strait Islander Peoples: Best Practice Guidelines. Canberra: NACCHO; 2022.
- 10. RHDAustralia (ASHM). Recommendations for Testing, Treating and Managing Hepatitis B — Australian Commentary on AASLD Guidelines. Darwin: Menzies School of Health Research; 2022.
- 11. Australian Technical Advisory Group on Immunisation (ATAGI). Australian Immunisation Handbook. Australian Government Department of Health, Canberra. Updated 2024.
- 12. Hajarizadeh B, Grebely J, Dore GJ. Epidemiology and natural history of HCV infection. Nat Rev Gastroenterol Hepatol. 2013;10(9):553–562.
- 13. Dore GJ, Hajarizadeh B. Elimination of hepatitis C virus in Australia: Laying the foundation. Infect Dis Clin North Am. 2020;34(3):577–596.
- 14. Wiegand J, van Bömmel F, Berg T. Management of acute hepatitis B and chronic hepatitis B in special patient populations. Lancet Gastroenterol Hepatol. 2019;4(5):384–397.
- 15. MacLachlan JH, Cowie BC. Hepatitis B virus epidemiology. Cold Spring Harb Perspect Med. 2015;5(5):a021410.