📋 Key Information Summary
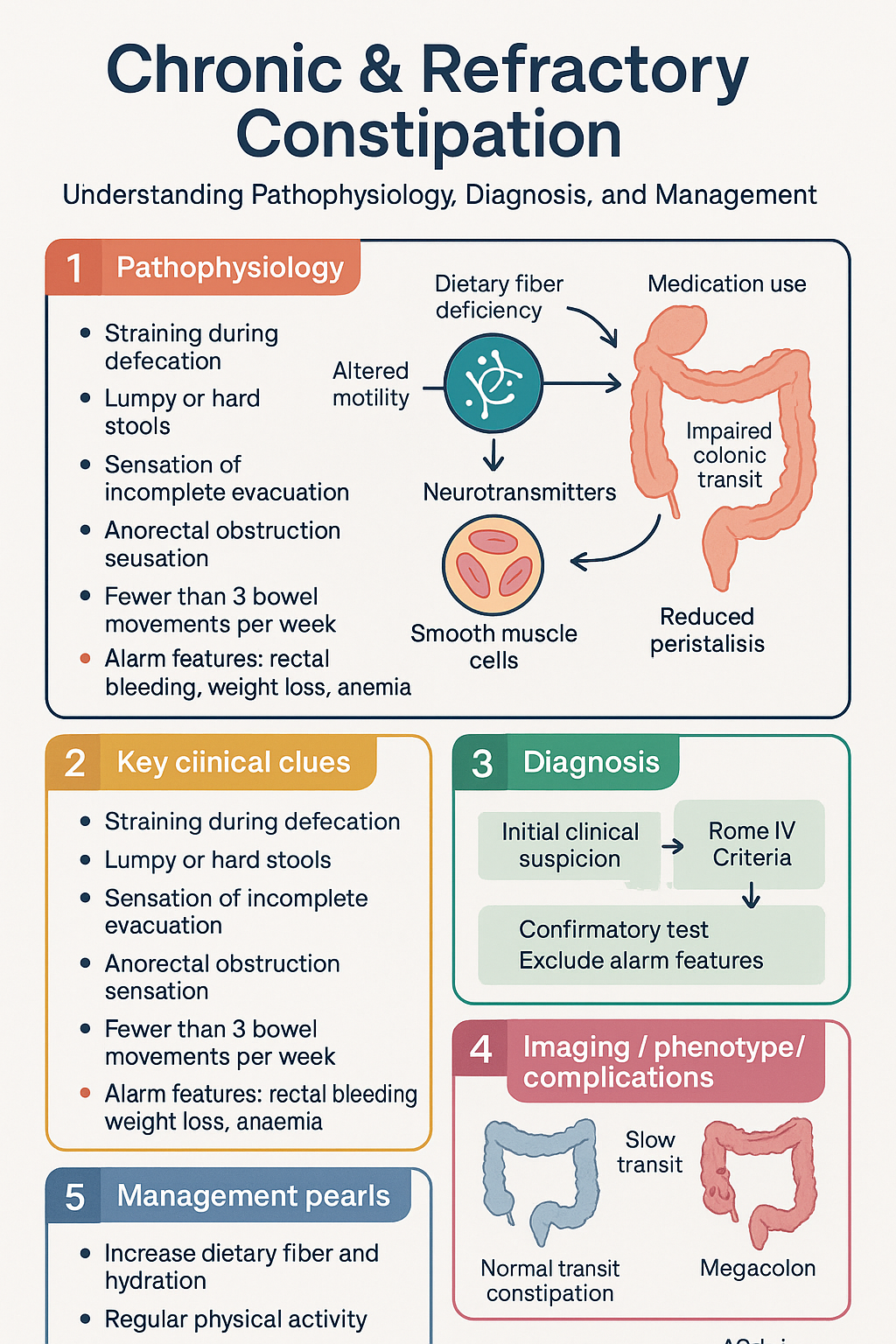
- Chronic constipation is defined by Rome IV criteria: ≥2 of 6 symptoms for ≥3 months with symptom onset ≥6 months prior — straining, lumpy/hard stools, sensation of incomplete evacuation, anorectal obstruction, manual manoeuvres, <3 spontaneous bowel movements per week.
- Always exclude alarm features before diagnosing functional constipation: rectal bleeding, unintentional weight loss, iron-deficiency anaemia, new onset age ≥50 years, acute change in bowel habit in older adults, family history of colorectal cancer, or a palpable abdominal/rectal mass.
- Medication review is critical — opioids, anticholinergics, calcium-channel blockers, iron supplements, calcium supplements, and serotonergic agents are the most common iatrogenic causes in Australian practice.
- First-line management centres on dietary fibre (≥30 g/day), adequate hydration (≥1.5–2 L/day), regular physical activity, and osmotic laxatives — polyethylene glycol (PEG/Movicol®) is the preferred first-choice laxative.
- Titrating PEG: start with 1 sachet (13.8 g) daily and increase by half to one sachet every 2–3 days until soft, easy-to-pass stools are achieved; doses up to 3 sachets/day may be required.
- Second-line therapy includes stimulant laxatives (senna, bisacodyl) — either as rescue or scheduled adjunct — and newer agents including prucalopride (Resotrans®) and linaclotide (Constella®) for refractory cases.
- Pelvic floor dysfunction (dyssynergic defaecation) should be suspected when patients strain excessively, report incomplete emptying, or have a normal transit study; anorectal manometry and biofeedback therapy are the gold standard for diagnosis and treatment.
- Prucalopride (5-TH4 agonist) is PBS-listed for women with chronic constipation refractory to laxatives (Authority Required); linaclotide (guanylate cyclase-C agonist) is also PBS-listed for patients failing standard laxative therapy.
- Refer to gastroenterology if symptoms persist despite ≥3 months of optimised therapy, if there is suspicion of mechanical obstruction or secondary cause, or for patients aged ≥45–50 years without recent colonoscopic evaluation.
- Special populations: pregnancy (PEG preferred, avoid stimulant laxatives long-term), paediatrics (PEG first-line per PIPES guideline), elderly (increased fall risk with straining, review polypharmacy), renal/hepatic (magnesium and sodium caution in renal impairment).
- Aboriginal and Torres Strait Islander populations have higher rates of constipation linked to low dietary fibre intake, remote access barriers, and limited specialist availability — culturally safe education and community-level interventions are essential.
- Ongoing monitoring: Bristol Stool Form Scale (target type 3–4), reassess fibre and fluid intake at each visit, audit laxative use, and screen for secondary causes if initial response is poor.
Introduction & Australian Epidemiology
Chronic constipation is one of the most common gastrointestinal complaints managed in Australian primary care, affecting an estimated 14–20% of the adult population. It is associated with significant reductions in quality of life, increased healthcare utilisation, and substantial economic burden. The condition encompasses functional constipation (FC), opioid-induced constipation (OIC), constipation-predominant irritable bowel syndrome (IBS-C), and secondary constipation arising from systemic disease, medications, or anatomical causes.
In Australia, chronic constipation accounts for approximately 1.2 million general practice consultations annually and is responsible for a significant proportion of over-the-counter laxative sales. The condition is more prevalent in women (OR 2.2), older adults, those with low dietary fibre intake, sedentary individuals, and those in lower socioeconomic groups. Aboriginal and Torres Strait Islander Australians experience disproportionately higher rates of gastrointestinal disease and may face additional barriers to timely diagnosis and management.
This guideline provides an evidence-based framework for the evaluation and management of chronic and refractory constipation in the Australian healthcare context, with emphasis on the stepped-care approach endorsed by the Gastroenterological Society of Australia (GESA), Royal Australian College of General Practitioners (RACGP), and Therapeutic Guidelines (eTG).
Initial Evaluation & Alarm Features
Rome IV Diagnostic Criteria for Functional Constipation
Functional constipation is diagnosed when the patient reports ≥2 of the following 6 criteria for ≥3 months, with symptom onset at least 6 months prior to diagnosis:
| Criterion | Description |
|---|---|
| 1. Straining | Straining during >25% of defaecations |
| 2. Lumpy stools | Lumpy or hard stools (Bristol type 1–2) in >25% of defaecations |
| 3. Incomplete evacuation | Sensation of incomplete evacuation in >25% of defaecations |
| 4. Anorectal obstruction | Sensation of anorectal obstruction/blockage in >25% of defaecations |
| 5. Manual manoeuvres | Need for manual manoeuvres (digital evacuation, perineal/pelvic support) in >25% of defaecations |
| 6. Few bowel movements | Fewer than 3 spontaneous bowel movements per week |
Loose stools should rarely be present without the use of laxatives, and insufficient criteria for IBS should be met. The Bristol Stool Form Scale should be used routinely to characterise stool consistency (target types 3–4 with treatment).
Medication Review — Iatrogenic Causes
A thorough medication review is a cornerstone of initial evaluation. The following commonly prescribed and over-the-counter agents in Australian practice may cause or exacerbate constipation:
| Drug Class | Examples | Mechanism |
|---|---|---|
| Opioids | Codeine, oxycodone, morphine, tapentadol, tramadol | μ-receptor activation in GI tract; reduced motility and secretion |
| Anticholinergics | Oxybutynin, solifenacin, amitriptyline, benztropine, hyoscine | Reduced parasympathetic GI motility |
| Calcium-channel blockers | Verapamil, nifedipine, diltiazem | Smooth muscle relaxation in GI tract |
| Iron supplements | Ferrous sulfate, ferrous fumarate | Direct irritant effect and altered gut motility |
| Calcium supplements | Calcium carbonate (Caltrate®) | Reduced colonic motility |
| Serotonergic agents | SSRIs (paroxetine most common), ondansetron | 5-HT3 antagonism; reduced GI motility |
| Others | Clonidine, bile acid sequestrants (cholestyramine), aluminium antacids, NSAIDs | Variable mechanisms |
Alarm Features (Red Flags) Requiring Urgent Investigation
The presence of any alarm feature mandates prompt investigation — typically with colonoscopy — before attributing symptoms to a functional aetiology:
- Rectal bleeding or blood in stool (not attributable to haemorrhoids)
- Unintentional weight loss (>5% body weight in 6 months)
- Iron-deficiency anaemia (low ferritin, low Hb, low MCV)
- New-onset constipation in a patient aged ≥50 years
- Acute change in bowel habit in an older adult (≥65 years)
- Family history of colorectal cancer (first-degree relative)
- Palpable abdominal or rectal mass
- Progressive worsening despite appropriate treatment
- Symptoms suggesting obstruction: vomiting, colicky abdominal pain, distension
Initial History and Examination
A comprehensive evaluation should include:
- Onset, duration, frequency, and consistency of bowel movements (use Bristol Stool Form Scale)
- Associated symptoms: straining, incomplete evacuation, abdominal pain, bloating
- Dietary history — fibre and fluid intake (average Australian intake ~20–25 g/day, target ≥30 g/day)
- Physical activity level
- Complete medication and supplement review (including over-the-counter)
- Obstetric and gynaecological history in women (pelvic floor injury, hysterectomy)
- Previous investigations and treatments tried
- Abdominal examination for masses, distension, tenderness
- Digital rectal examination (DRE) — essential to assess resting and squeeze anal tone, rectal mass, faecal impaction, and paradoxical contraction of the puborectalis
First-Line Management
First-line management of chronic constipation follows a structured, stepwise approach incorporating lifestyle modification and osmotic laxative therapy. This approach aligns with Therapeutic Guidelines (eTG), GESA recommendations, and international consensus (AGA, ACG).
Lifestyle and Dietary Modification
First-Line Laxative Therapy: Osmotic Laxatives
Polyethylene glycol (PEG) is the recommended first-choice osmotic laxative for chronic constipation. It is an iso-osmotic, non-absorbable agent with a strong evidence base, good tolerability, and PBS availability.
Psyllium Husk (Bulk-Forming Agent)
Lactulose (Alternative Osmotic Laxative)
Note: Lactulose is generally less well-tolerated than PEG due to bloating, flatulence, and sweet taste. PEG is preferred as first-line per eTG and AGA guidelines. Lactulose may be used as an alternative in patients who cannot tolerate PEG or in the management of hepatic encephalopathy (dual indication).
Second-Line & Refractory Management
When first-line measures (fibre, fluids, exercise, and optimised osmotic laxative therapy) have been trialled for an adequate duration (4–6 weeks at maximum tolerated dose) without satisfactory response, a stepwise escalation to second-line therapies is warranted. The management approach depends on whether the underlying issue is slow transit constipation, pelvic floor dysfunction (dyssynergic defaecation), or both.
Stimulant Laxatives
Stimulant laxatives are the most common second-line agents. They may be used as rescue therapy (prn) or as scheduled adjunctive therapy in patients with refractory symptoms.
Secretagogues (for Refractory Functional Constipation)
Prokinetic Agent
Pelvic Floor Dysfunction (Dyssynergic Defaecation)
Pelvic floor dysfunction is present in up to 50% of patients with refractory constipation. It is characterised by paradoxical contraction (dyssynergia) or inadequate relaxation of the puborectalis and external anal sphincter during defaecation, or inadequate rectal propulsive force (inadequate defaecation propulsion).
Clinical suspicion: Patients report excessive straining, sensation of incomplete evacuation, need for perineal or vaginal splinting to defaecate, and normal or near-normal stool frequency but difficulty with actual evacuation.
Diagnostic approach:
- Anorectal manometry (ARM) — Gold standard for diagnosing dyssynergic defaecation. Measures resting and squeeze anal pressures, rectoanal inhibitory reflex, and balloon expulsion test (inability to expel a 50 mL balloon in ≤1 minute is abnormal).
- Defaecography (evacuating proctography) — Identifies anatomical causes: rectocoele, intussusception, sigmoidocoele. Available in major tertiary centres (MBS item 32158).
- Colonic transit study (radiopaque marker study) — Distinguishes slow transit constipation from outlet obstruction. Patients stop laxatives 72 hours prior and ingest radiopaque markers (Sitz markers); an abdominal X-ray is performed on day 5 (MBS item 57713).
Opioid-Induced Constipation — Specific Agents
Stepwise Approach Summary
Investigations
Investigations should be guided by clinical suspicion. Most patients with functional constipation can be diagnosed and managed without extensive investigations. The following tests should be considered based on clinical context:

Monitoring
Ongoing monitoring is essential for patients with chronic constipation to ensure treatment adequacy, medication safety, and early detection of secondary causes:
Monitoring Tools
- Bristol Stool Form Scale (BSFS): Patient self-report of stool consistency on a 1–7 scale. Target types 3 (soft, sausage-shaped with cracks) to 4 (smooth, sausage-shaped). Available as a patient handout.
- Patient Assessment of Constipation Symptoms (PAC-SYM): Validated 12-item questionnaire assessing abdominal, rectal, and stool symptoms. Useful for tracking treatment response in research and clinical practice.
- Patient Assessment of Constipation Quality of Life (PAC-QOL): 28-item questionnaire measuring quality of life across four domains — physical discomfort, psychosocial discomfort, worries and concerns, and satisfaction.
- Bowel diary: Record of daily stool frequency, consistency (BSFS type), straining episodes, laxative use, fibre and fluid intake. Recommended for 1–2 weeks before clinic review.
Special Populations
Pregnancy
Paediatrics
Elderly (≥65 years)
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health Considerations
When to Refer
Timely referral to gastroenterology or colorectal surgery is essential for patients who meet the following criteria:
- Persistent symptoms despite ≥3 months of optimised first- and second-line therapy (fibre, fluids, PEG at adequate dose ± stimulant laxatives)
- Suspected secondary cause: hypothyroidism, hypercalcaemia, neurological disease (e.g., spinal cord injury, multiple sclerosis, Parkinson's disease), systemic sclerosis
- Suspected pelvic floor dysfunction: excessive straining, incomplete evacuation, need for manual manoeuvres — requires anorectal manometry and biofeedback assessment
- Age ≥45–50 years without colonoscopy performed within the previous 5 years — colonoscopic evaluation recommended before attributing symptoms to functional constipation
- Failure to respond to secretagogues or prokinetics, or need for specialist access to these agents (Authority Required PBS prescriptions may require specialist initiation)
- Consideration of colonic transit studies to distinguish slow transit from outlet dysfunction
- Suspected bowel obstruction: colicky abdominal pain, vomiting, absolute constipation, abdominal distension, absent bowel sounds
- Acute-onset constipation with alarm features (rectal bleeding, weight loss, mass) in older adults
- Faecal impaction not responding to oral disimpaction regimens in community setting — may require hospital admission for manual disimpaction or rectal interventions
- Toxic megacolon (rare but critical): abdominal distension, tenderness, systemic toxicity
Colorectal Surgery Referral
- Significant rectocoele or intussusception identified on defaecography causing obstructive defaecation symptoms
- Severe slow transit constipation refractory to all medical therapy — subtotal colectomy with ileorectal anastomosis may be considered in highly selected patients (requires multidisciplinary team assessment)
- Large rectal mass or significant anatomical pathology identified on colonoscopy
Other Referral Pathways
- Pelvic floor physiotherapy: For patients with dyssynergic defaecation confirmed or suspected on clinical grounds; biofeedback therapy is first-line for pelvic floor dysfunction
- Dietitian: For individualised fibre and fluid counselling, particularly in patients with food insecurity, complex dietary needs, or comorbid conditions limiting fibre intake (e.g., gastroparesis, strictures)
- Pain medicine / Palliative care: For patients with opioid-induced constipation requiring complex laxative management and opioid dose optimisation
📚 References
- 1. Bharucha AE, Pemberton JH, Locke GR. American Gastroenterological Association technical review on constipation. Gastroenterology. 2013;144(1):218–238.
- 2. Lacy BE, Mearin F, Chang L, et al. Bowel disorders. Gastroenterology. 2016;150(6):1393–1407.e5. (Rome IV criteria)
- 3. Ford AC, Suares NC. Effect of laxatives and pharmacological therapies in chronic idiopathic constipation: systematic review and meta-analysis. Gut. 2011;60(2):209–218.
- 4. Gastroenterological Society of Australia (GESA). Constipation: Clinical Practice Guideline. Melbourne: GESA; 2023.
- 5. National Institute for Health and Care Excellence (NICE). Constipation in over 12s: diagnosis and management. Clinical guideline CG61 (updated 2024). London: NICE.
- 6. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework: Measures of gastrointestinal health. Canberra: AIHW; 2023.
- 7. Paediatric Integrated Program for Evaluation of Symptoms (PIPES). Management of constipation in children: evidence-based guideline. The Royal Children's Hospital Melbourne; 2022.
- 8. Rao SS, Bharucha AE, Chiarioni G, et al. Anorectal disorders. Gastroenterology. 2016;150(6):1430–1442.e4.
- 9. Wald A. Constipation: advances in diagnosis and treatment. JAMA. 2016;315(2):185–195.
- 10. Camilleri M, Ford AC, Mawe GM, et al. Chronic constipation. Nat Rev Dis Primers. 2017;3:17095.
- 11. Royal Australian College of General Practitioners (RACGP). Prescribing drugs of dependence in general practice: Part B — Opioids. Melbourne: RACGP; 2022.
- 12. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.
- 13. Dimidi E, Christodoulides S, Fragkos KC, et al. The effect of probiotics on functional constipation in adults: a systematic review and meta-analysis of randomised controlled trials. Am J Clin Nutr. 2014;100(4):1075–1084.
- 14. Pharmaceutical Benefits Scheme (PBS). Australian Government Department of Health. Available at: https://www.pbs.gov.au. Accessed 2024.
- 15. Drossman DA, Hasler WL. Rome IV — functional GI disorders: disorders of gut-brain interaction. Gastroenterology. 2016;150(6):1257–1261.