📋 Key Information Summary
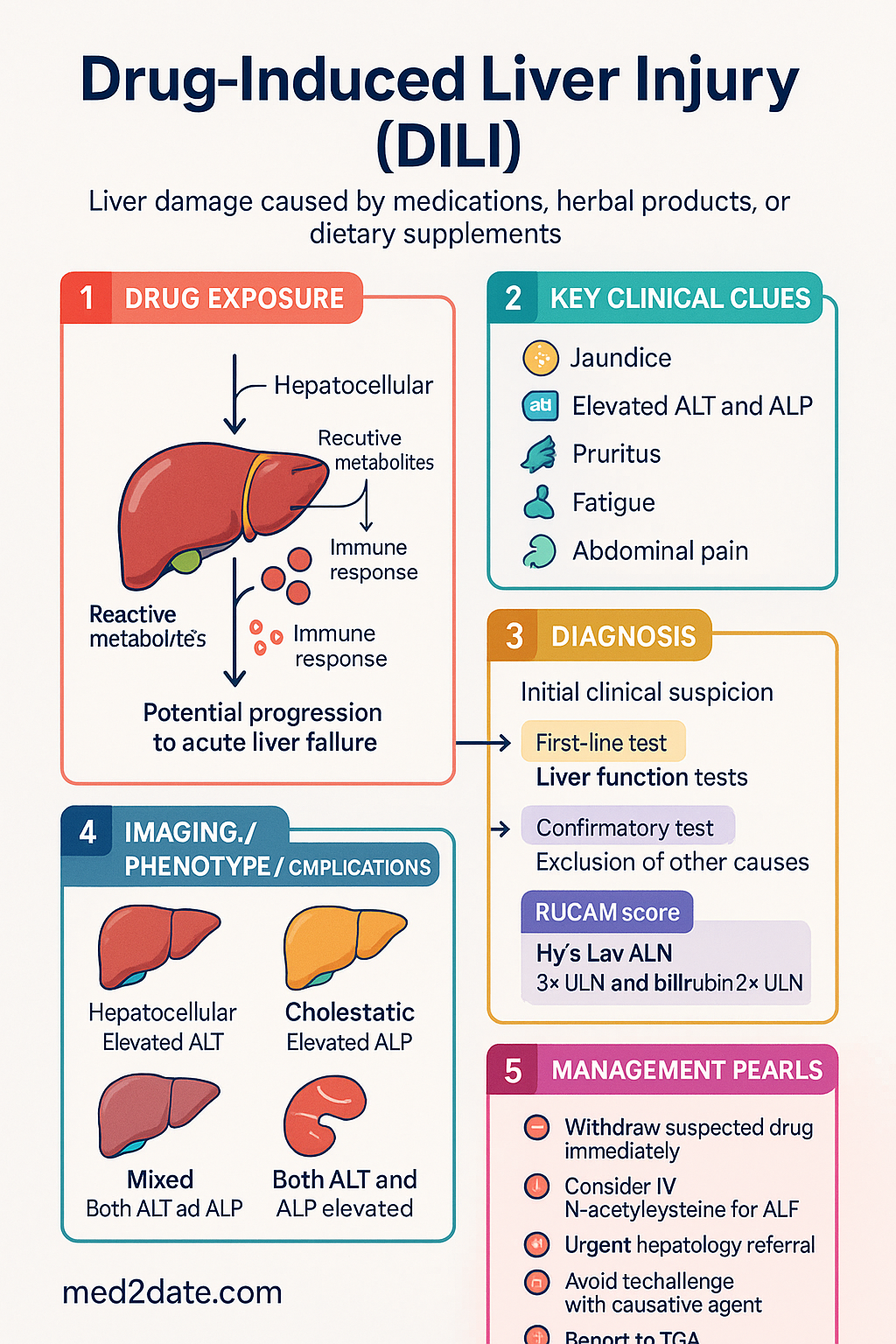
- Definition: Drug-induced liver injury (DILI) is liver damage caused by medications, herbal products, or dietary supplements, presenting as acute hepatocellular, cholestatic, or mixed injury.
- Classification by pattern: Hepatocellular (ALT >5× ULN, R ≥5), cholestatic (ALP elevation, R ≤2), or mixed (R 2–5); pattern guides differential diagnosis and prognosis.
- Intrinsic vs idiosyncratic: Intrinsic DILI (e.g., paracetamol) is dose-dependent, predictable, and reproducible; idiosyncratic DILI is unpredictable and may be immune-mediated or metabolic.
- Hy's Law: ALT >3× ULN with total bilirubin >2× ULN (without obstruction) predicts ~10% mortality — treat as a medical emergency requiring urgent specialist review.
- Commonest culprit in Australia: Amoxicillin-clavulanate is the most frequently implicated drug; other common causes include flucloxacillin, nitrofurantoin, methotrexate, statins, and herbal/dietary supplements.
- Diagnosis: DILI is a clinical diagnosis of exclusion; use the RUCAM (Roussel Uclaf Causality Assessment Method) to quantify causality; temporal relationship and dechallenge are key.
- Immediate management: Withdraw the suspected agent promptly; exclude viral hepatitis, autoimmune hepatitis, biliary obstruction, and metabolic causes.
- N-acetylcysteine (NAC): Consider IV NAC in non-paracetamol DILI with coagulopathy or early acute liver failure (ALF); evidence supports improved transplant-free survival in early-stage ALF.
- Transplant referral: Refer urgently to a liver transplant centre if INR is rising, encephalopathy develops, or King's College criteria are met.
- Avoid rechallenge: Re-exposure to the causative agent is contraindicated and may cause more severe or fatal injury.
- ATSI considerations: Aboriginal and Torres Strait Islander peoples have higher rates of herbal/alternative medicine use, limited specialist access in remote areas, and higher background rates of chronic liver disease — requiring culturally safe, proactive screening and telehealth-enabled care.
- Reporting: Report suspected DILI to the TGA via the Adverse Medicine Events Line (1300 134 237) and document in the patient's My Health Record.
Introduction & Australian Epidemiology
Drug-induced liver injury (DILI) encompasses a spectrum of hepatic dysfunction caused by prescription medications, over-the-counter drugs, herbal preparations, and dietary supplements. It is a leading cause of acute liver failure (ALF) in Australia and the most common reason for post-market withdrawal of medications worldwide.
In Australia, DILI accounts for approximately 10–15% of all cases of acute hepatitis presenting to tertiary centres. The annual incidence is estimated at 14–19 per 100,000 population, though this is likely under-reported due to diagnostic challenges and the self-limiting nature of mild cases. Amoxicillin-clavulanate is the commonest single agent implicated, consistent with its high prescribing frequency in primary care.
Paracetamol remains the most common cause of ALF in Australia, responsible for nearly 50% of all ALF referrals to transplant centres. Idiosyncratic DILI from antibiotics, anti-tuberculosis agents, and herbal products comprises the majority of non-paracetamol cases. Aboriginal and Torres Strait Islander peoples are disproportionately affected, with higher rates of traditional medicine use and reduced access to specialist hepatology services in remote and very remote communities.
Classification
DILI is classified by biochemical pattern, mechanism, chronology, and clinical course. Correct classification guides the differential diagnosis, investigation pathway, and prognosis.
Biochemical Pattern (R Value)
The R value (ratio of ALT/ULN to ALP/ULN) determines the injury pattern at presentation:
| Pattern | R Value | Key Features | Common Culprits |
|---|---|---|---|
| Hepatocellular | R ≥5 | ALT >5× ULN; ALP normal or mildly elevated; higher mortality risk | Paracetamol, isoniazid, nitrofurantoin, statins, methotrexate, herbal supplements |
| Cholestatic | R ≤2 | ALP >2× ULN dominant; ALT mildly elevated; jaundice, pruritus common | Amoxicillin-clavulanate, flucloxacillin, erythromycin, anabolic steroids |
| Mixed | R 2–5 | Both ALT and ALP significantly elevated; intermediate prognosis | Sulfonamides, phenytoin, carbamazepine, diclofenac |
Mechanism: Intrinsic vs Idiosyncratic
Hy's Law — Critical Prognostic Indicator
- Signals impending acute liver failure in up to 10–50% of affected patients
- Requires immediate discontinuation of all suspect drugs
- Urgent hepatology referral and consideration of liver transplant centre notification
- Serial monitoring of INR, bilirubin, and hepatic encephalopathy grade
Chronological Classification
| Type | Latency | Course After Withdrawal |
|---|---|---|
| Acute | 1–8 weeks | Resolution in days–weeks (most common) |
| Sub-acute | 8–26 weeks | Slower resolution; may mimic autoimmune hepatitis |
| Chronic | >26 weeks | Persistent abnormality; vanishing bile duct syndrome, autoimmune-like (e.g., nitrofurantoin, minocycline) |
Common Culprits & Diagnosis
Commonly Implicated Agents in Australia
The following agents account for the majority of DILI notifications to Australian hepatology registries:
Diagnostic Approach
DILI is a diagnosis of exclusion. No single test is diagnostic. The systematic approach involves:
RUCAM Causality Assessment
The Roussel Uclaf Causality Assessment Method (RUCAM) is the internationally validated scoring system for DILI causality. It incorporates seven domains scored to yield a total of −4 to +14 points:
| Domain | Score Range | Key Considerations |
|---|---|---|
| Time to onset | +1 to +2 | First exposure; latency consistent with known drug |
| Course after cessation | 0 to +3 | Decrease in ALT/ALP by ≥50% within 8 days = highly suggestive |
| Risk factors | 0 to +2 | Age ≥55, alcohol, pregnancy |
| Concomitant drugs | 0 to +3 | No other cause = +3; time suggestive = +2 |
| Non-drug causes | −3 to +2 | Exclusion of viral, biliary, autoimmune, ischaemic causes |
| Previous information | 0 to +2 | Published DILI for this drug; labelled reaction |
| Rechallenge | 0 to +3 | Positive rechallenge +3 (NOT recommended deliberately) |
| Total Score | Causality |
|---|---|
| ≤0 | Excluded |
| 1–2 | Unlikely |
| 3–5 | Possible |
| 6–8 | Probable |
| ≥9 | Highly probable |
Baseline Investigations
Management
Immediate Management Principles
N-Acetylcysteine (NAC) in Non-Paracetamol DILI
- Indicated in DILI with evidence of ALF: coagulopathy (INR ≥1.5), any grade of encephalopathy, or rapidly rising bilirubin
- Greatest benefit in early-stage ALF (Grade I–II hepatic encephalopathy)
- No established benefit in mild–moderate DILI without ALF features
Transplant Centre Referral
- INR ≥6.5 (regardless of encephalopathy grade)
- Any three of: age <10 or >40; non-paracetamol aetiology; jaundice-to-encephalopathy interval >7 days; INR ≥3.5; serum bilirubin ≥300 µmol/L
- Progressive hepatic encephalopathy (Grade II or above)
- Hy's Law criteria with worsening trajectory despite drug withdrawal
- Lactate >3.5 mmol/L after fluid resuscitation
Severity Grading & Disposition
Monitoring After Withdrawal
Serial LFT monitoring is essential to confirm improvement and exclude chronicity:
- Days 1–7: LFTs, INR, bilirubin daily or second-daily in severe cases
- Weeks 2–4: LFTs weekly; expect ≥50% decline in ALT by 8 days in most cases
- Months 1–6: LFTs monthly until normalised; if persistent elevation, investigate for chronic DILI, autoimmune hepatitis, or vanishing bile duct syndrome
- Document the causative drug in the patient's allergy/adverse drug reaction list and My Health Record
Special Populations
Aboriginal and Torres Strait Islander peoples experience a disproportionate burden of liver disease and face unique challenges in the recognition and management of DILI. Cultural safety, proactive screening, and accessible specialist referral are essential.
📚 References
- 1. Björnsson ES, Bergmann OM, Björnsson HK, et al. Incidence, presentation, and outcomes in patients with drug-induced liver injury in the general population of Iceland. Gastroenterology. 2013;144(7):1419–1425.
- 2. Danan G, Teschke R. RUCAM in Drug and Herb Induced Liver Injury: The Update. Int J Mol Sci. 2016;17(1):14.
- 3. Lee WM, Hynan LS, Rossaro L, et al. Intravenous N-acetylcysteine improves transplant-free survival in early stage non-acetaminophen acute liver failure. Gastroenterology. 2009;137(3):856–864.
- 4. Chalasani N, Bonkovsky HL, Fontana R, et al. Features and outcomes of 899 patients with drug-induced liver injury: The DILIN Prospective Study. Gastroenterology. 2015;148(7):1340–1352.
- 5. Lucena MI, Molokhia M, Shen Y, et al. Susceptibility to amoxicillin-clavulanate-induced liver injury is influenced by multiple HLA class I and II alleles. Gastroenterology. 2011;141(1):338–347.
- 6. Daly AK, Donaldson PT, Bhatnagar P, et al. HLA-B*5701 genotype is a major determinant of drug-induced liver injury due to flucloxacillin. Nat Genet. 2009;41(7):816–819.
- 7. Navarro VJ, Barnhart H, Bonkovsky HL, et al. Liver injury from herbals and dietary supplements in the U.S. Drug-Induced Liver Injury Network. Hepatology. 2014;60(4):1399–1408.
- 8. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2017.
- 9. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework 2020 summary report. Canberra: AIHW; 2020.
- 10. Fontana RJ, Hayashi PH, Gu J, et al. Idiosyncratic drug-induced liver injury is associated with substantial morbidity and mortality within 6 months from onset. Gastroenterology. 2014;147(1):96–108.
- 11. Craig DGN, Lee A, Hayes PC, Simpson KJ. Review article: The Royal College of Physicians' Biomarker in Liver Injury (BALI) consensus recommendations. Aliment Pharmacol Ther. 2010;31(8):844–856.
- 12. Lewis JH. The Art and Science of Diagnosing and Managing Drug-Induced Liver Injury in 2020 and Beyond. Clin Gastroenterol Hepatol. 2020;18(11):2441–2452.
- 13. Teschke R, Frenzel C, Schulze J, Eickhoff A. Herbal hepatotoxicity: challenges and pitfalls of causality assessment methods. World J Gastroenterol. 2013;19(19):2864–2882.