📋 Key Information Summary
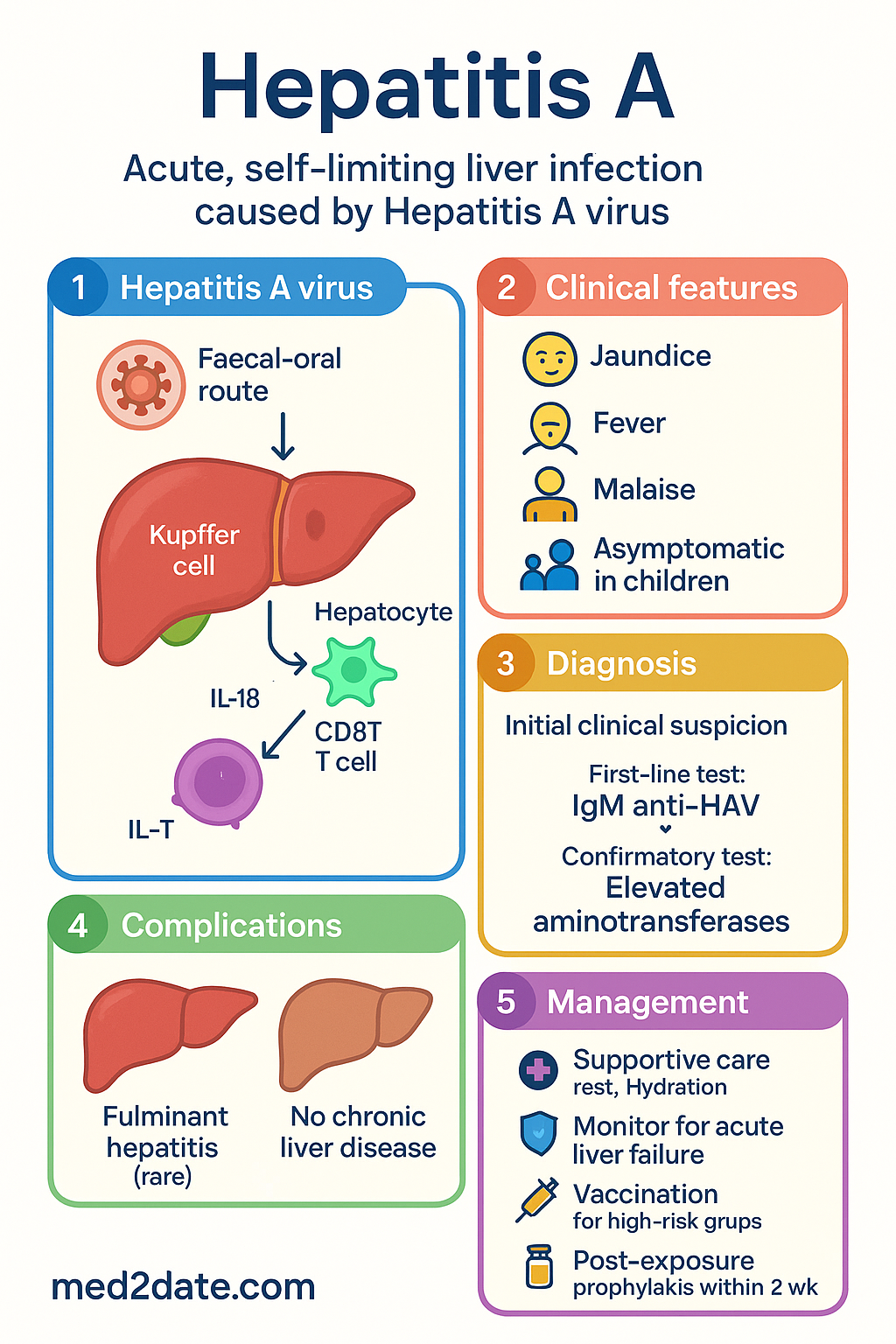
- Hepatitis A is an acute, self-limiting liver infection caused by the Hepatitis A virus (HAV), transmitted via the faecal-oral route.
- Key transmission routes include ingestion of contaminated food/water, person-to-person contact (especially in childcare), and sexual transmission among men who have sex with men (MSM).
- Australia has low endemicity; most cases are acquired overseas or linked to specific outbreaks.
- There is NO chronic carrier state or chronic liver disease following acute infection.
- Clinical presentation ranges from asymptomatic (common in children) to jaundice, fever, and malaise in adults.
- Diagnosis is confirmed by detecting IgM anti-HAV in serum during acute illness.
- Management is primarily supportive care; monitor for signs of acute liver failure (ALF), especially in patients with pre-existing chronic liver disease.
- Prevention is paramount: vaccination with inactivated HAV vaccine is recommended for high-risk groups (travellers, MSM, chronic liver disease, certain occupations).
- Post-exposure prophylaxis (PEP) with HAV vaccine (and/or immunoglobulin for specific groups) is effective if given within 2 weeks of exposure.
- The National Immunisation Program (NIP) funds HAV vaccine for Aboriginal and Torres Strait Islander children in high-risk areas and other specified risk groups.
- Good hygiene, safe food handling, and water treatment are critical public health measures to prevent outbreaks.
- Fulminant hepatitis is rare (<1%) but carries high mortality; risk is significantly increased in individuals with chronic hepatitis B or C.
Epidemiology & Transmission
Global and Australian Epidemiology
Hepatitis A has a global distribution, with incidence highest in regions with poor sanitation. Australia is a low-endemicity country. Notifications have declined significantly due to vaccination programmes and improved sanitation. Most cases in Australia are either imported (associated with travel to endemic regions) or linked to local outbreaks from a common source (e.g., contaminated food).
Transmission Routes
The Hepatitis A virus (HAV) is primarily transmitted via the faecal-oral route, person-to-person contact, or ingestion of contaminated food or water.
| Route | Details |
|---|---|
| Contaminated Food/Water | Consumption of raw or undercooked shellfish (filter feeders), uncooked produce washed with contaminated water, or food handled by an infectious person. |
| Person-to-Person | Close household contact, especially in settings with nappy-changing or poor hand hygiene (e.g., childcare centres). Outbreaks in long-term care facilities are also reported. |
| Sexual Transmission | Significant risk among men who have sex with men (MSM), particularly via oro-anal contact. |
| Travel | Travellers to high-endemicity regions (e.g., parts of Asia, Africa, Central/South America) are at risk. |
Key Epidemiological Features
- Incubation Period: Average 28 days (range 15–50 days).
- Infectious Period: Highest in the 2 weeks before jaundice onset; virus shedding in stool declines rapidly after.
- No Chronic Carrier State: Infection leads to complete recovery and lifelong immunity. There is no chronic infection or chronic liver disease.
- Fulminant Hepatitis: Rare (<1% of cases) but can be fatal. The risk is markedly higher in patients with pre-existing chronic liver disease (e.g., chronic hepatitis B or C).
Diagnosis & Management
Diagnostic Approach
Diagnosis is based on clinical suspicion in the setting of acute hepatitis (elevated aminotransferases, jaundice) confirmed by serology.
Key Investigations
Management of Acute Infection
There is no specific antiviral therapy. Management is supportive.
- Supportive Care: Rest, adequate hydration, and avoidance of hepatotoxins (e.g., alcohol, paracetamol).
- Monitor for Complications: Watch for signs of acute liver failure (ALF): coagulopathy (INR >1.5), encephalopathy, or worsening jaundice. Urgent specialist referral (gastroenterology/hepatology) is required.
- Hospital Admission: Consider for patients with severe symptoms, dehydration, coagulopathy, or significant comorbidities.
Prevention
1. Vaccination (Pre-exposure Prophylaxis)
The inactivated HAV vaccine is highly effective (>95% seroconversion).
Groups Recommended for Vaccination:
- Travellers to intermediate/high endemicity countries.
- Men who have sex with men (MSM).
- Individuals with chronic liver disease (any cause).
- Occupational risk: sewage workers, food handlers, staff of childcare centres and facilities for the intellectually disabled, healthcare workers in high-risk settings.
- Residents of institutions for the intellectually disabled.
- Recipients of clotting factor concentrates.
- Aboriginal and Torres Strait Islander children in high-risk communities (funded on NIP).
2. Post-Exposure Prophylaxis (PEP)
For susceptible (non-immune) individuals after close contact with a confirmed case. Must be given within 14 days of exposure.
ATSI Health Considerations
📚 References
- 1. Australian Government Department of Health and Aged Care. Australian Immunisation Handbook. Canberra: Australian Government; 2024. Available from: https://immunisationhandbook.health.gov.au
- 2. Communicable Diseases Network Australia (CDNA). Guidelines for the Public Health Management of Viral Hepatitis. Canberra: CDNA; 2023.
- 3. The Royal Australian College of General Practitioners (RACGP). Hepatitis B and C Screening and Management. (Contextual reference for general viral hepatitis). East Melbourne: RACGP; 2023.
- 4. World Health Organization (WHO). Hepatitis A Fact Sheet. Geneva: WHO; 2024. Available from: https://www.who.int/news-room/fact-sheets/detail/hepatitis-a
- 5. Heymann DL, editor. Control of Communicable Diseases Manual. 21st ed. Washington: American Public Health Association; 2022. (Sections on Hepatitis A).
- 6. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework. Canberra: AIHW; 2023. (Indicator 3.07 Vaccine-preventable diseases).
- 7. National Centre for Immunisation Research and Surveillance (NCIRS). Hepatitis A Vaccines: Information for Healthcare Professionals. Sydney: NCIRS; 2023.
- 8. The Australasian Society for HIV, Viral Hepatitis and Sexual Health Medicine (ASHM). Hepatitis A Management and Prevention in MSM. Sydney: ASHM; 2022.
- 9. Vento S, et al. Fulminant hepatitis associated with hepatitis A virus superinfection in patients with chronic liver disease. J Viral Hepat. 1998;5(1):9-14.
- 10. Victorian Government Department of Health. Post-Exposure Prophylaxis for Hepatitis A: Guidelines. Melbourne: Victorian Government; 2024.