📋 Key Information Summary
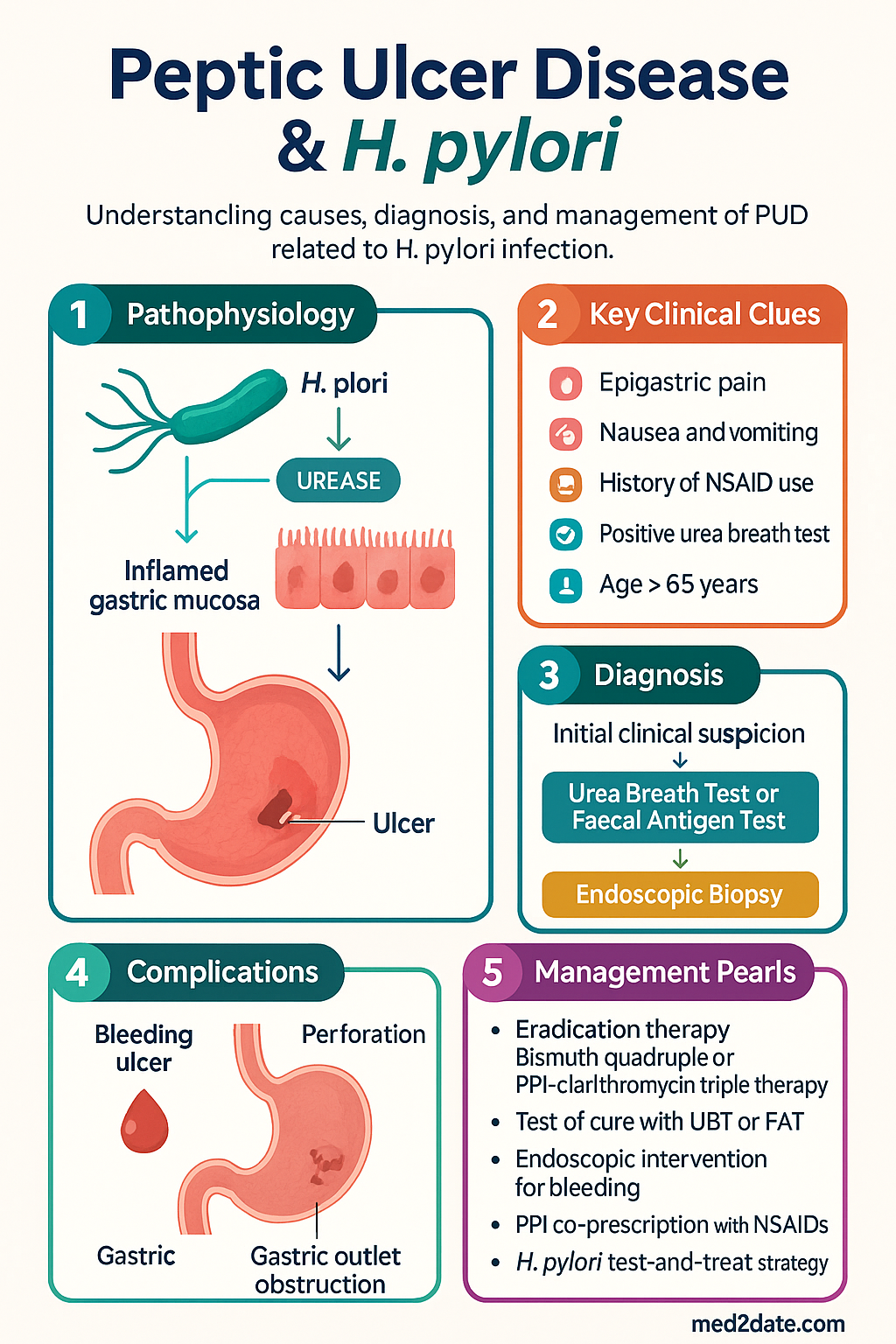
- Peptic ulcer disease (PUD) encompasses gastric and duodenal ulcers, primarily caused by H. pylori infection or NSAID use.
- Non-serological tests for H. pylori (urea breath test, faecal antigen, biopsy-based) require PPIs withheld for ≥2 weeks and antibiotics for ≥4 weeks prior.
- Serology is not used for test of cure due to inability to distinguish active from past infection.
- First-line eradication: Bismuth quadruple therapy (PPI + bismuth subsalicylate/subcitrate + tetracycline + metronidazole) for 14 days is a key empiric option in Australia.
- PPI-clarithromycin triple therapy (PPI + amoxicillin + clarithromycin) is first-line only where clarithromycin resistance is confirmed <15%.
- Second-line or rescue therapies include levofloxacin-based or rifabutin-based regimens after treatment failure.
- Test of cure (urea breath test or faecal antigen) is mandatory at least 4 weeks after completing eradication therapy.
- Acute upper GI bleeding from ulcers: Endoscopic therapy with dual modality (e.g., clipping + injection) is standard, followed by IV PPI infusion.
- Forrest classification (Ia, Ib, IIa, IIb, IIc, III) guides endoscopic intervention and re-bleeding risk.
- All gastric ulcers require endoscopic biopsy to exclude malignancy, even if benign in appearance.
- NSAID-related ulcer risk stratification guides gastroprotection: age >65, prior PUD, anticoagulant/steroid use, high-dose NSAID are major risk factors.
- High-risk patients on NSAIDs require a PPI co-prescription or a COX-2 selective inhibitor with PPI.
- Test-and-treat for H. pylori is recommended before starting long-term NSAID therapy.
🎧 Audio Brief
H. pylori Diagnosis
Accurate diagnosis of Helicobacter pylori infection is fundamental to PUD management. Choice of test depends on clinical context, prior therapy, and local availability.
Non-Invasive Tests
Invasive (Biopsy-Based) Tests – Require Endoscopy
A "test-and-treat" strategy (using UBT or FAT) is appropriate for young patients (<50 years) with uncomplicated dyspepsia and no alarm features. Endoscopy is indicated for patients >50 years, with alarm features (dysphagia, weight loss, vomiting, anaemia), or treatment failure.
Eradication Therapy
Successful eradication cures H. pylori-related ulcers and prevents recurrence. Regimen choice is based on local resistance patterns, prior exposure, and allergies. All courses are 14 days unless specified.
First-Line Therapy
Second-Line / Rescue Therapies (After First-Line Failure)
High-Dose Dual Therapy
PUD Complications
Complications of peptic ulcer disease include bleeding, perforation, gastric outlet obstruction, and, for gastric ulcers, potential malignancy. Management requires urgent intervention.
Bleeding Ulcer
Acute upper GI bleeding is a medical emergency. Risk stratification and endoscopic therapy are cornerstone.
| Forrest Class | Appearance | Re-bleed Risk | Management |
|---|---|---|---|
| Ia | Spurting haemorrhage | Very High (~90%) | Immediate endoscopic therapy + IV PPI infusion |
| Ib | Oozing haemorrhage | High (~50-60%) | Endoscopic therapy + IV PPI infusion |
| IIa | Non-bleeding visible vessel | High (~40-50%) | Endoscopic therapy + IV PPI infusion |
| IIb | Adherent clot | Moderate (~20-30%) | Consider clot removal → treat underlying lesion (IIa). IV PPI. |
| IIc | Flat pigmented spot | Low (~5-10%) | No endoscopic therapy. Oral PPI. |
| III | Clean base ulcer | Very Low (~2-5%) | No endoscopic therapy. Oral PPI. |
Endoscopic & Pharmacological Therapy
Dual modality endoscopic therapy (e.g., injection of adrenaline + mechanical therapy with haemoclips or thermal coagulation) is superior to monotherapy for high-risk stigmata. Newer options include Over-The-Scope Clips (OTSC) and haemospray for refractory bleeding.
IV PPI Therapy: Following endoscopic haemostasis, high-dose IV PPI infusion (e.g., esomeprazole 80 mg bolus then 8 mg/hr for 72 hrs) is standard. Intermittent IV PPI (e.g., 40 mg BD) may be non-inferior in lower-risk patients (Forrest IIb).
Perforation
Sudden onset severe abdominal pain. Presents with peritonitis and free air on imaging. Requires urgent surgical consultation for laparoscopic or open repair, often with an omental patch. Concurrent H. pylori testing and eradication post-operatively is essential.
Gastric Outlet Obstruction
Caused by chronic inflammation and scarring from duodenal or pyloric channel ulcers. Presents with vomiting, early satiety, and weight loss. Initial management is gastric decompression with NG tube, IV PPI, and fluid/electrolyte correction. Endoscopic balloon dilation may be attempted; surgery is reserved for refractory cases.
Malignancy Exclusion in Gastric Ulcers
All gastric ulcers identified at endoscopy must be biopsied (multiple samples from ulcer edge and base) to exclude adenocarcinoma. Even with benign histology, repeat endoscopy with biopsy in 6-8 weeks is mandatory to confirm complete healing and non-malignant aetiology.
Special Populations
PUD and H. pylori prevalence are higher in Aboriginal and Torres Strait Islander peoples, contributing to significant morbidity. Management must consider unique barriers.
Engagement with local Aboriginal Community Controlled Health Organisations (ACCHOs) is crucial for culturally safe care, holistic management, and improving long-term outcomes.
📚 References
- 1. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.
- 2. Malfertheiner P, et al. Helicobacter pylori infection. Nat Rev Dis Primers. 2023;9(1):19.
- 3. Fallone CA, et al. The Toronto Consensus for the Treatment of Helicobacter pylori Infection in Adults. Gastroenterology. 2016;151(1):51-69.e14.
- 4. Laine L, et al. Management of Patients with Ulcer Bleeding. Am J Gastroenterol. 2012;107(3):345-360.
- 5. The Royal Australian College of General Practitioners (RACGP). Management of dyspepsia and heartburn in general practice. East Melbourne: RACGP; 2020.
- 6. Medicines Australia. Australian Medicines Handbook. Adelaide: AMH; 2024.
- 7. Australian Government Department of Health. Pharmaceutical Benefits Scheme (PBS). Available at: pbs.gov.au.
- 8. National Health and Medical Research Council (NHMRC). Australian guidelines to reduce health risks from drinking alcohol. Canberra: NHMRC; 2020. [Relevance: alcohol as PUD risk factor].
- 9. Lanas A, Chan FKL. Peptic ulcer disease. Lancet. 2017;390(10094):613-624.
- 10. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander health performance framework. Canberra: AIHW; 2023.
- 11. RHDAustralia (The Australian Government Department of Health). Recognising and managing acute rheumatic fever and rheumatic heart disease. [Relevance: penicillin prophylaxis and PUD].
- 12. Chey WD, et al. ACG Clinical Guideline: Treatment of Helicobacter pylori Infection. Am J Gastroenterol. 2017;112(2):212-239.