📋 Key Information Summary
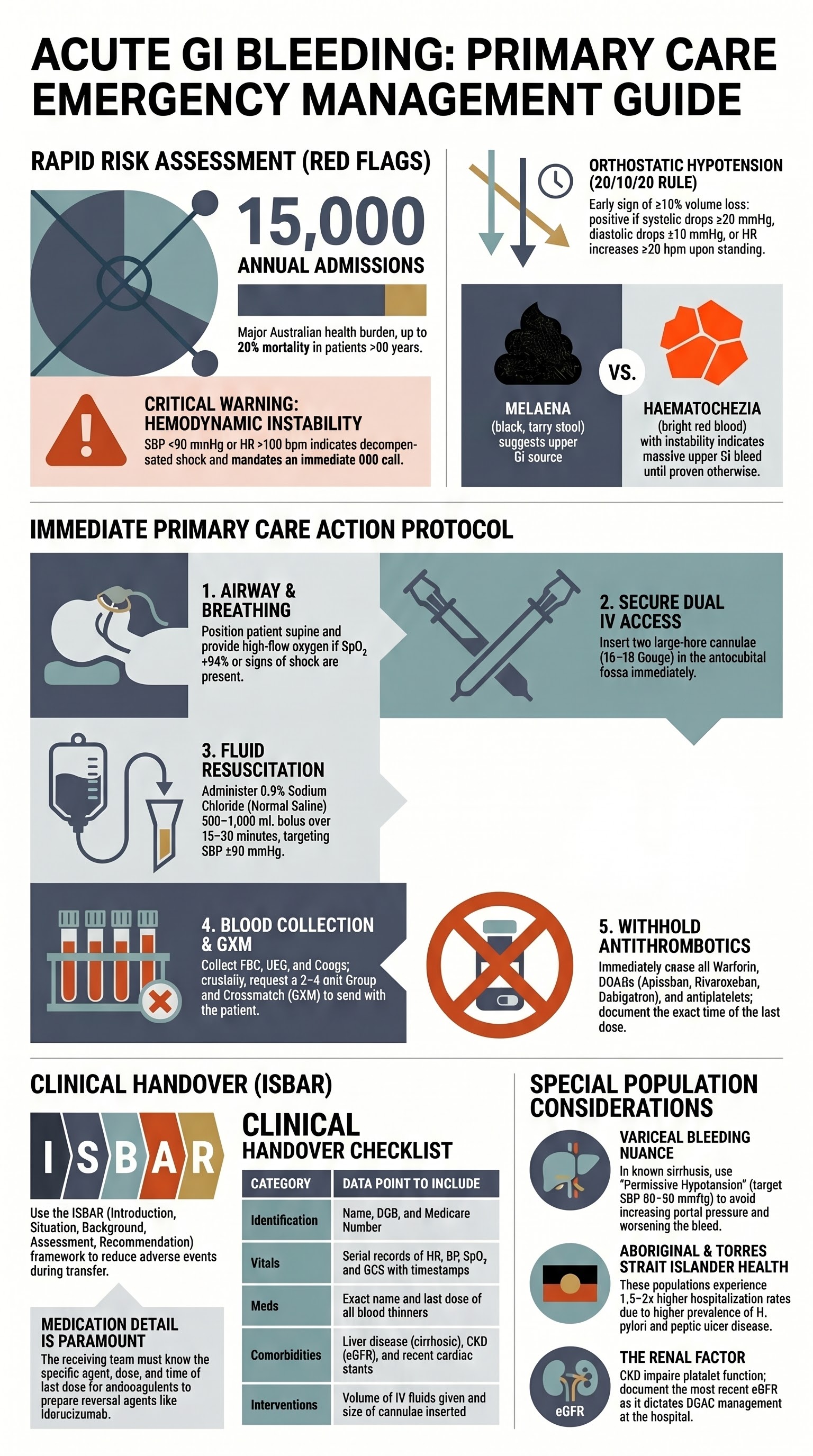
- Acute gastrointestinal (GI) bleeding is a common emergency presentation with significant mortality in patients aged ≥65 years; approximately 15,000 hospital admissions per year in Australia.
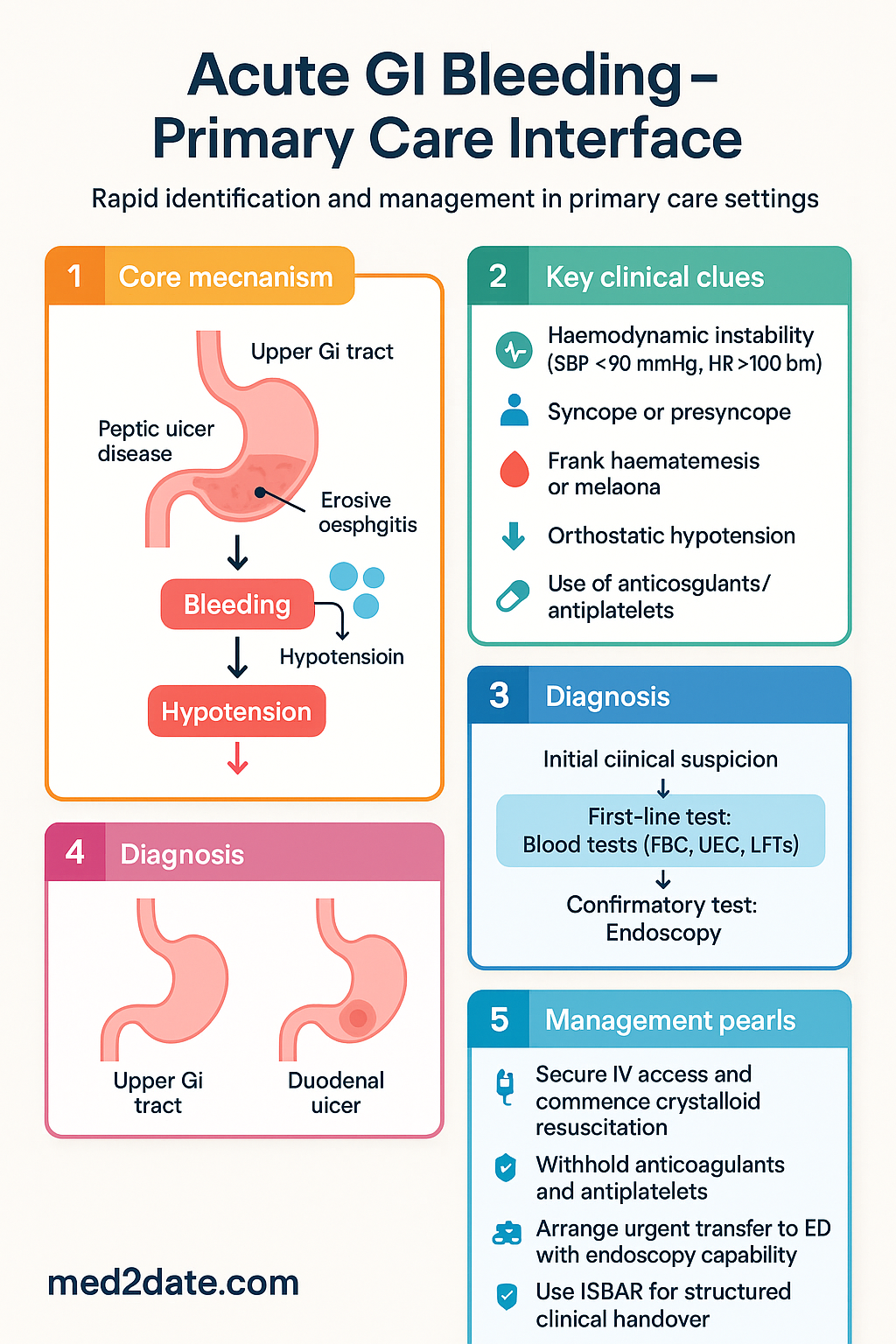
- Upper GI bleeding (above the ligament of Treitz) accounts for the majority of acute presentations, with peptic ulcer disease (40–50%), varices (10–15%), and erosive oesophagitis among the leading causes.
- Red flag features requiring emergent hospital transfer include haemodynamic instability (systolic BP <90 mmHg, HR >100 bpm), syncope, frank haematemesis, melaena, and brisk haematochezia.
- Orthostatic hypotension (systolic drop ≥20 mmHg or diastolic drop ≥10 mmHg on standing) is an early and sensitive sign of significant volume depletion — assess before supine vitals normalise.
- Immediate primary care actions: secure IV access (two large-bore cannulae, 16–18G), commence crystalloid resuscitation (0.9% sodium chloride), and arrange urgent transfer to the nearest ED with endoscopy capability.
- Assess and document all anticoagulant and antiplatelet agents (warfarin, DOACs, clopidogrel, aspirin, ticagrelor); these significantly increase bleeding severity and influence management timing.
- Patients on warfarin with active GI bleeding require urgent INR testing and may need prothrombin complex concentrate (PCC) and IV vitamin K at the receiving hospital.
- DOACs (apixaban, rivaroxaban, dabigatran) should be withheld immediately; specific reversal agents (idarucizumab for dabigatran, andexanet alfa for factor Xa inhibitors) are available at tertiary centres.
- A structured clinical handover using ISBAR (Introduction, Situation, Background, Assessment, Recommendation) improves communication with the receiving emergency team and reduces adverse events.
- Do not delay transfer for investigations beyond basic bloods — time to definitive haemostasis (endoscopy/interventional radiology) is the key determinant of patient outcomes.
- Aboriginal and Torres Strait Islander Australians experience higher rates of H. pylori infection and peptic ulcer disease; ensure culturally safe communication and involve Aboriginal health workers where possible.
- Elderly patients and those with significant comorbidities (cardiac, renal, hepatic disease) are at highest risk of adverse outcomes and require lower thresholds for transfer and aggressive resuscitation.
Introduction & Australian Epidemiology
Acute gastrointestinal (GI) bleeding encompasses any bleeding from the oesophagus to the anus that presents as an emergency requiring urgent assessment and management. In the Australian primary care setting, the general practitioner's role is to rapidly identify the severity of bleeding, initiate resuscitation, stabilise the patient, and facilitate timely transfer to a facility capable of definitive management — typically via endoscopy or interventional radiology.
GI bleeding is classified anatomically as upper GI (proximal to the ligament of Treitz) or lower GI (distal to the ligament of Treitz). Upper GI bleeding accounts for approximately 70–80% of acute presentations and carries a higher mortality rate (6–10%) compared with lower GI bleeding (2–4%). In Australia, acute upper GI bleeding results in an estimated 15,000 hospital admissions annually, with peptic ulcer disease remaining the single most common aetiology.
| Epidemiological Feature | Australian Data |
|---|---|
| Annual hospital admissions (acute GI bleed) | ~15,000 (AIHW data) |
| In-hospital mortality (upper GI bleed) | 6–10% overall; up to 20% in patients aged ≥80 years |
| Most common cause — upper GI | Peptic ulcer disease (40–50%) |
| Most common cause — lower GI | Diverticular disease (30–40%) |
| Median age at presentation | 65–70 years |
| Proportion on anticoagulants/antiplatelets | 30–40% of admissions |
| Re-bleeding rate (peptic ulcer) | 10–20% without definitive treatment |
| ATSI over-representation | 1.5–2× age-adjusted rate vs non-Indigenous Australians |
Key risk factors in the Australian population include increasing age, chronic NSAID or aspirin use, Helicobacter pylori infection (prevalence 15–30% in the general Australian population, higher in ATSI communities), cirrhosis with portal hypertension, and anticoagulant or antiplatelet therapy. The widespread use of direct oral anticoagulants (DOACs) for atrial fibrillation has contributed to an increasing proportion of GI bleeds related to anticoagulation.
Red Flag Features
Rapid identification of red flag features is the most critical step in primary care assessment of acute GI bleeding. These features indicate significant haemorrhage or haemodynamic compromise and mandate immediate resuscitation and emergency transfer. The absence of visible blood (melaena may be occult to the patient) does not exclude significant GI bleeding.
Hemodynamic Instability
Haemodynamic instability is the single most important red flag. In primary care, assess:
- Heart rate >100 bpm: Tachycardia is an early compensatory response to hypovolaemia and may precede hypotension by 30–60 minutes.
- Systolic blood pressure <90 mmHg: Indicates decompensated haemorrhagic shock; by this stage, estimated blood loss is typically >1,500 mL (Class III haemorrhage).
- Cool peripheries, pallor, diaphoresis: Clinical signs of poor peripheral perfusion consistent with Class II–III haemorrhage.
- Altered mental status: Agitation, confusion, or obtundation indicate cerebral hypoperfusion and Class III–IV haemorrhage — this is a medical emergency.
Syncope and Pre-Syncope
Syncope in the context of GI bleeding indicates significant volume loss (>1,000–1,500 mL) and is an independent predictor of severe haemorrhage. Even a single episode of presyncope (lightheadedness on standing, visual dimming) warrants urgent transfer. Patients who present after a syncopal episode — even if now haemodynamically stable — should be considered high risk, as they may re-bleed unpredictably.
Orthostatic Hypotension
Orthostatic (postural) hypotension is one of the earliest and most sensitive indicators of intravascular volume depletion. It may be detected before supine blood pressure falls below the normal range. Measure as follows:
Melaena
Melaena — black, tarry, foul-smelling stools — indicates upper GI bleeding (typically proximal to the ileum) with blood in transit for ≥14 hours. A single melaena stool may represent 100–200 mL of blood loss; copious or ongoing melaena indicates a significant and potentially ongoing bleed. Importantly, melaena may persist for 3–5 days after a self-limited bleed, so the clinical context (vital signs, haemoglobin trend) is more important than stool colour alone.
Haematemesis
Haematemesis (vomiting of blood) is the hallmark of upper GI bleeding. It may present as:
- Coffee-ground vomitus: Dark brown-black granular material indicating partially digested blood — suggests slower or intermittent upper GI bleeding.
- Frank haematemesis: Fresh red blood or blood clots — indicates rapid, high-volume upper GI bleeding and is a more urgent presentation.
The volume of haematemesis is a poor guide to total blood loss, as significant volumes may pool in the stomach before being vomited. Always assess haemodynamic status rather than relying on the volume of visible blood.
Brisk Haematochezia
Haematochezia — passage of bright red or maroon blood per rectum — is most commonly associated with lower GI bleeding (diverticular disease, angiodysplasia, colorectal neoplasm). However, brisk haematochezia (large-volume passage of red blood with clots) can occur with massive upper GI bleeding when rapid transit overwhelms the capacity for digestion. A rapid upper GI source must be excluded in any patient with brisk haematochezia and haemodynamic instability.
Summary of Red Flag Features
| Red Flag | Clinical Significance | Action |
|---|---|---|
| SBP <90 mmHg | Class III–IV haemorrhage (>1,500 mL loss) | Call 000, commence IV resuscitation |
| HR >100 bpm | Compensated to decompensated shock | Urgent transfer, IV access |
| Syncope / presyncope | Significant volume loss, high-risk feature | Urgent transfer irrespective of current vitals |
| Orthostatic hypotension | Early volume depletion (≥15% blood loss) | Transfer for observation, IV fluids |
| Frank haematemesis | Active upper GI haemorrhage | Urgent transfer, nil by mouth |
| Ongoing melaena | Continued upper GI blood loss | Transfer, monitor Hb trend |
| Brisk haematochezia | Potentially massive upper or lower GI bleed | Emergent transfer to tertiary centre |
| On anticoagulants/antiplatelets | Increased severity, delayed haemostasis | Withhold agents, transfer with medication list |
| Age ≥65 years | Higher mortality, reduced physiological reserve | Lower threshold for transfer |
| Known cirrhosis / liver disease | Variceal bleeding risk — highest mortality | Emergent transfer to tertiary centre with hepatology |
Immediate Actions in Primary Care
When a patient presents to a general practice with suspected acute GI bleeding, the GP has a narrow window of opportunity to stabilise the patient before transfer. The following actions should be undertaken in a structured, time-critical manner. Do not delay transfer for non-essential investigations.
Fluid Resuscitation — Detail
Crystalloid resuscitation with 0.9% sodium chloride is the first-line fluid in primary care for acute GI bleeding. The following guidance applies:
| Fluid | Volume | Rate | Notes |
|---|---|---|---|
| 0.9% sodium chloride (first-line) | 500–1,000 mL bolus | Over 15–30 min | Repeat ×1–2 as needed; target SBP ≥90 mmHg |
| Hartmann's solution (alternative) | 500–1,000 mL bolus | Over 15–30 min | Acceptable alternative if NS unavailable |
| Packed red blood cells | As per transfusion protocol | N/A in primary care | Commence at receiving hospital; GXM essential |
Medications That May Be Considered at Receiving Hospital
While the primary care role does not include administering definitive pharmacotherapy, awareness of the agents used at the receiving hospital helps with pre-transfer communication and anticipatory management.
Nil by Mouth (NBM) Status
All patients with active GI bleeding should be made nil by mouth from the point of assessment. This is essential for:
- Safety in case of emergency endoscopy or surgical intervention
- Prevention of aspiration if the patient deteriorates or requires sedation
- Reducing gastric acid production and potential re-bleeding stimulus
If the patient is on essential oral medications (e.g., antiepileptics), discuss with the receiving team regarding IV conversion.
Communication with the Receiving Team
Effective communication between primary care and the receiving emergency or gastroenterology team is a critical determinant of patient outcomes. A structured handover reduces information loss, prevents errors in medication management, and ensures the receiving team can initiate definitive management without delay.
ISBAR Framework for Clinical Handover
The ISBAR (Introduction, Situation, Background, Assessment, Recommendation) framework is endorsed by the Australian Commission on Safety and Quality in Health Care (ACSQHC) and should be used for all clinical handovers.
Critical Information to Provide
Medication List — Anticoagulants and Antiplatelets
The medication list is arguably the single most important piece of information for the receiving team. Provide precise details for all anticoagulant and antiplatelet agents:
| Medication Class | Common Agents in Australia | Critical Information to Communicate |
|---|---|---|
| Warfarin | Coumadin®, Marevan® | Last dose, most recent INR, indication (AF, VTE, mechanical valve) |
| DOACs — Factor Xa inhibitors | Rivaroxaban (Xarelto®), Apixaban (Eliquis®), Edoxaban (Lixiana®) | Last dose (hours ago), dose, renal function (eGFR), indication |
| DOACs — Direct thrombin inhibitor | Dabigatran (Pradaxa®) | Last dose, renal function — dabigatran is 80% renally cleared, reversal with idarucizumab available |
| Aspirin | Cartia®, aspirin 100 mg | Dose, indication (primary vs secondary prevention), last dose |
| Clopidogrel | Plavix®, Iscover® | Dose, last dose, recent PCI/stent (critical — may affect timing of cessation) |
| Ticagrelor | Brilinta® | Dose, last dose, recent ACS or stent — discuss with cardiology if <12 months post-ACS |
| Dual antiplatelet therapy (DAPT) | Aspirin + clopidogrel or ticagrelor | Duration remaining, date and type of stent/intervention |
| LMWH | Enoxaparin (Clexane®) | Dose, last dose, indication (treatment vs prophylaxis) |
Comorbidities
The following comorbidities significantly impact the management and prognosis of acute GI bleeding and should be communicated to the receiving team:
- Chronic liver disease / cirrhosis: High risk of variceal bleeding, coagulopathy, and hepatic decompensation. Communicate known Child-Pugh or MELD score if available.
- Chronic kidney disease (CKD): Impaired platelet function (uraemic bleeding diathesis), altered drug clearance, higher bleeding risk. Provide most recent eGFR and creatinine.
- Ischaemic heart disease / recent ACS: Affects decision-making regarding antiplatelet resumption and permissive hypotension targets.
- Atrial fibrillation: Explains anticoagulant use; risk of thromboembolism if anticoagulation withheld for prolonged period.
- Previous GI surgery: Altered anatomy may affect endoscopy approach or indicate afferent loop bleeding (Billroth II).
- Known GI malignancy or polyps: May indicate neoplastic source of bleeding.
- Diabetes mellitus: Increased infection risk, impaired wound healing, potential for HbA1c-related perioperative issues.
Prior GI History
- Previous episodes of GI bleeding — dates, cause, and management (endoscopic therapy, surgery)
- Known peptic ulcer disease, H. pylori status, eradication history
- Previous gastroscopy or colonoscopy findings and dates
- History of oesophageal varices or portal hypertensive gastropathy
- Inflammatory bowel disease (Crohn's disease, ulcerative colitis) and current flare status
- Known diverticular disease
Vitals and Estimated Blood Loss
Provide a serial record of vital signs with timestamps. This enables the receiving team to assess trajectory (improving vs deteriorating):
| Parameter | What to Record | Method |
|---|---|---|
| Heart rate | Rate, rhythm, regularity | Manual or automated BP cuff |
| Blood pressure | Supine + standing (at 1 min and 3 min) | Automated sphygmomanometer |
| Oxygen saturation | SpO₂ on room air (or O₂ if administered) | Pulse oximetry |
| Respiratory rate | Breaths per minute | Observed count over 30 seconds × 2 |
| Mental status | GCS (Eye + Verbal + Motor) | Standardised GCS assessment |
| Temperature | Core temperature | Tympanic or axillary |
| Estimated blood loss | Volume of haematemesis / melaena / haematochezia | Clinical estimation (pints, cups); photograph if possible |
| Urine output | Volume per hour (if catheterised) | Hourly measurement; oliguria (<0.5 mL/kg/hr) indicates inadequate perfusion |
Haemoglobin and Laboratory Results
If point-of-care or rapid pathology is available at the practice, include the following in your handover:
- Haemoglobin: Note that Hb may be normal in the first 1–2 hours of acute bleeding (haemodilution has not yet occurred). A normal Hb does not exclude significant haemorrhage.
- INR / APTT: Critical if the patient is on anticoagulants. An INR >4.0 in a warfarinised patient with active bleeding warrants urgent reversal.
- Urea: Elevated urea with normal creatinine may suggest upper GI bleeding (digested blood protein absorption).
- Crossmatch status: Advise whether GXM has been collected and sent, or if it needs to be done at the receiving hospital.
Handover Checklist
| Item | Provided? |
|---|---|
| Patient identification (name, DOB, address, Medicare number) | ☐ |
| Presenting complaint and onset / duration | ☐ |
| Type of bleeding (haematemesis / melaena / haematochezia) | ☐ |
| Estimated volume and duration of bleeding | ☐ |
| Vital signs with timestamps (including orthostatic measurements) | ☐ |
| Full medication list — especially anticoagulants and antiplatelets with last dose | ☐ |
| Relevant comorbidities (liver disease, CKD, IHD, AF) | ☐ |
| Prior GI history (previous bleeds, endoscopy findings, H. pylori status) | ☐ |
| Allergies | ☐ |
| Interventions commenced (IV access size, fluids given, medications ceased) | ☐ |
| Blood results (Hb, INR, UEC if available) | ☐ |
| GXM collected and sent? Yes / No | ☐ |
| Specialist notification (hepatologist if cirrhosis, cardiologist if recent stent) | ☐ |
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Investigations in Primary Care
Investigations in primary care should be limited to those that are immediately available and will not delay transfer. The primary care role is to initiate, not complete, the diagnostic workup.
Quick Reference — Primary Care Action Summary
📚 References
- 1. Lanas A, García-Rodríguez LA, Polo-Tomás M, et al. Time trends and impact of upper and lower gastrointestinal bleeding and perforation in clinical practice. Am J Gastroenterol. 2009;104(7):1633–1641.
- 2. Australian Institute of Health and Welfare (AIHW). Hospitalisations due to gastrointestinal conditions in Australia. Canberra: AIHW; 2023.
- 3. Stanley AJ, Laine L, Dalton HR, et al. Comparison of risk scoring systems for patients presenting with upper gastrointestinal bleeding: international multicentre prospective study. BMJ. 2017;356:i6432.
- 4. National Blood Authority (NBA). Australian Patient Blood Management Guidelines — Module 2: Perioperative. Canberra: NBA; 2012 (updated 2023).
- 5. HALT-IT Trial Collaborators. Effects of a high-dose 24-h infusion of tranexamic acid on death and thromboembolic events in patients with acute gastrointestinal bleeding (HALT-IT): an international randomised, double-blind, placebo-controlled trial. Lancet. 2020;395(10241):1927–1936.
- 6. Royal Australian College of General Practitioners (RACGP). Standards for General Practices. 5th ed. Melbourne: RACGP; 2020.
- 7. Australian Commission on Safety and Quality in Health Care (ACSQHC). Communicating for Safety Standard — Clinical Handover. Sydney: ACSQHC; 2019.
- 8. Gralnek IM, Dumonceau JM, Kuipers EJ, et al. Diagnosis and management of nonvariceal upper gastrointestinal hemorrhage: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy. 2015;47(1):a1–a46.
- 9. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework: Details of data quality and gaps. Canberra: AIHW; 2023.
- 10. Sung JJ, Chiu PW, Chan FKL, et al. Asia-Pacific working group consensus on non-variceal upper gastrointestinal bleeding: an update 2018. Gut. 2018;67(10):1757–1768.
- 11. Royal Australian and New Zealand College of Radiologists (RANZCR). Interventional Radiology Guidelines — Gastrointestinal Haemorrhage Embolisation. Sydney: RANZCR; 2021.
- 12. Strate LL, Gralnek IM. ACG Clinical Guideline: Management of patients with acute lower gastrointestinal bleeding. Am J Gastroenterol. 2016;111(5):683–699.
- 13. Lim W, Dentali F, Eikelboom JW, Crowther MA. Meta-analysis: low-molecular-weight heparin and bleeding in patients with severe renal insufficiency. Ann Intern Med. 2006;144(9):673–684.
- 14. Potter BJ, Larrivée B, Bhatt DL. Anticoagulation in patients with gastrointestinal bleeding: when and how to restart. J Am Coll Cardiol. 2021;77(15):1910–1923.
- 15. Mejia R, Schulz T, Ewald B, et al. Helicobacter pylori infection in Aboriginal Australians: prevalence and associated factors. Aust N Z J Public Health. 2020;44(3):223–228.