📋 Key Information Summary
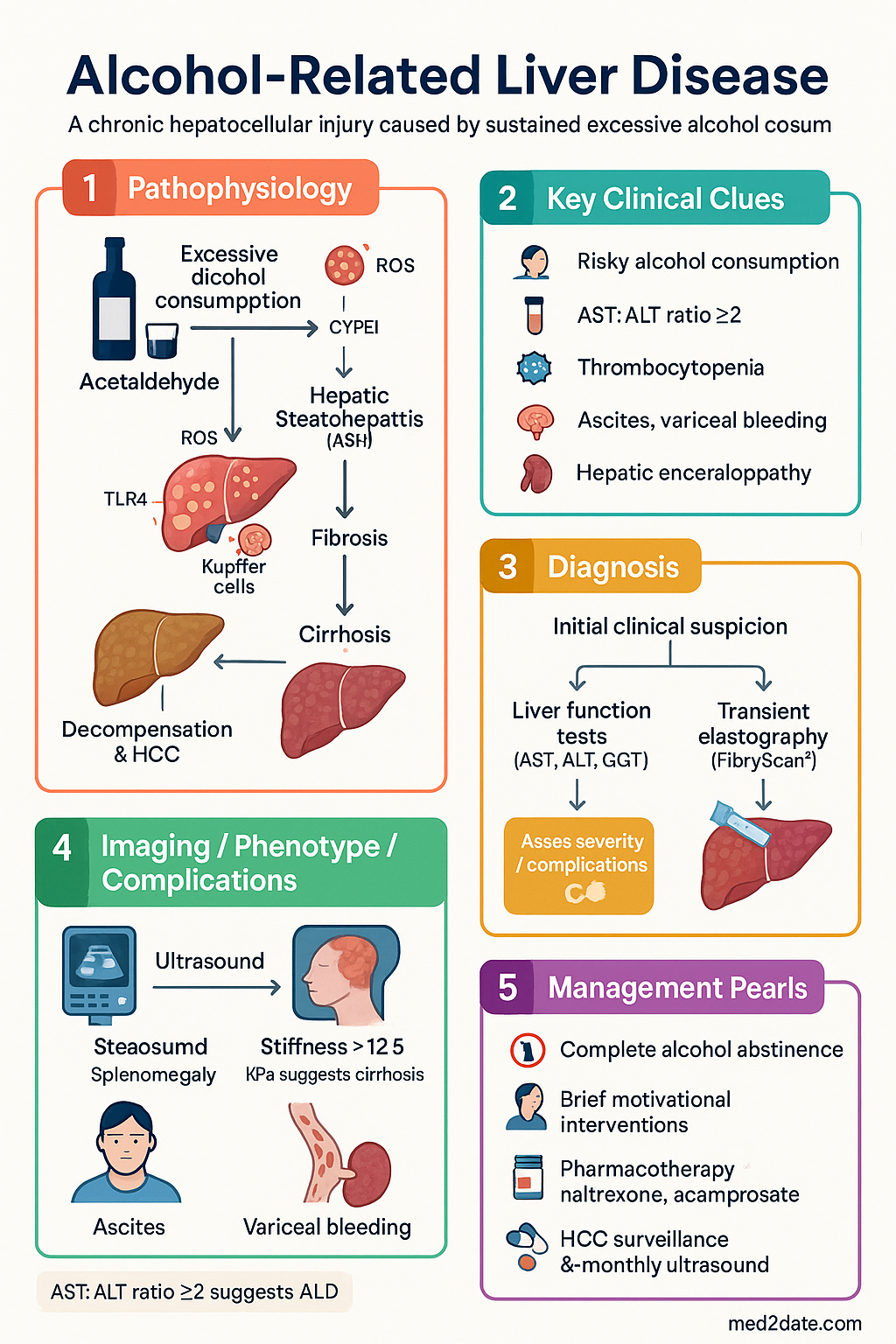
- Alcohol-related liver disease (ALD) encompasses a spectrum from hepatic steatosis through steatohepatitis (ASH), fibrosis, cirrhosis, and hepatocellular carcinoma (HCC); it remains one of the leading causes of liver-related morbidity and mortality in Australia.
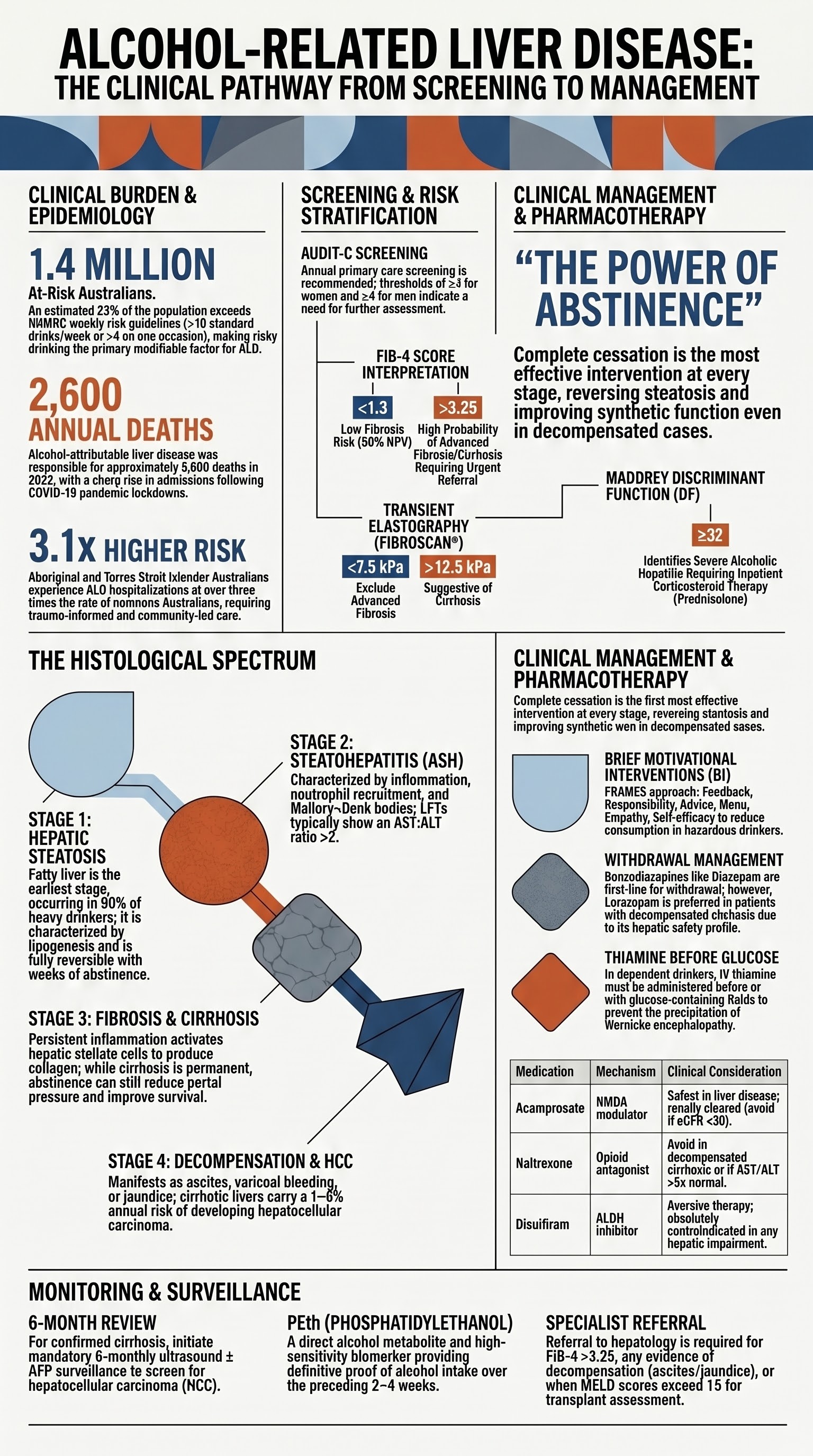
- An estimated 1.4 million Australians exceed NHMRC guideline limits for alcohol intake (>10 standard drinks/week or >4 on any single occasion); risky drinking is the strongest modifiable risk factor for ALD.
- Screening with the AUDIT-C (≥3 women, ≥4 men) or full AUDIT questionnaire should be performed annually in primary care; the AUDIT-C can be embedded in routine electronic health record templates.
- Brief motivational interventions (BI) — typically 1–3 sessions of 10–30 minutes — reduce alcohol consumption and are cost-effective in Australian general practice settings.
- Evaluate for liver damage with LFTs (AST, ALT, GGT), platelet count, INR, FIB-4 score, and liver ultrasound; an AST:ALT ratio >2 is highly suggestive of ALD.
- Transient elastography (FibroScan®) is available at most major Australian hospitals (MBS item 13020 or 55063) and is the preferred non-invasive test for staging fibrosis.
- Complete alcohol abstinence is the single most effective intervention — it can reverse steatosis, halt fibrosis progression, and improve survival even in decompensated cirrhosis.
- Alcohol withdrawal syndrome (AWS) should be assessed with the Clinical Institute Withdrawal Assessment for Alcohol–Revised (CIWA-Ar); benzodiazepines (diazepam or chlordiazepoxide) are first-line for moderate–severe withdrawal, preferably in a supervised medical setting.
- Patients with decompensated cirrhosis (ascites, variceal bleeding, hepatic encephalopathy) or severe alcoholic hepatitis (Maddrey DF ≥32) require urgent hepatology referral and consideration of corticosteroids (prednisolone 40 mg/day for 28 days).
- Pharmacotherapy for alcohol use disorder includes naltrexone (oral or extended-release IM injection), acamprosate, and disulfiram — all PBS-listed; choice depends on comorbidities, hepatic function, and patient preference.
- HCC surveillance with 6-monthly ultrasound ± AFP is mandatory for all patients with ALD-related cirrhosis, and liver transplant assessment should be considered early in eligible patients.
- Aboriginal and Torres Strait Islander Australians experience ALD at 3–5× the rate of non-Indigenous Australians; culturally safe, trauma-informed, and community-led approaches are essential to closing the gap.
Introduction & Australian Epidemiology
Alcohol-related liver disease (ALD) is a chronic hepatocellular injury caused by sustained excessive alcohol consumption. It encompasses a histological continuum — hepatic steatosis (fatty liver), alcoholic steatohepatitis (ASH), progressive fibrosis, cirrhosis, and hepatocellular carcinoma (HCC). ALD is a leading cause of liver transplantation in Australia and accounts for approximately 25–30% of all liver-related hospital admissions nationally.
In the 2022–2023 National Drug Strategy Household Survey, 16.8% of Australians aged 14 and over exceeded the NHMRC single-occasion risk guideline (≥5 standard drinks on one occasion) at least monthly, and 23% exceeded the lifetime risk guideline (>10 standard drinks per week). The annual economic burden of alcohol-related harm in Australia has been estimated at over billion (including healthcare, lost productivity, and social costs).
ALD disproportionately affects Aboriginal and Torres Strait Islander peoples, people experiencing socioeconomic disadvantage, rural and remote populations, and middle-aged men (40–65 years). However, ALD in women is increasing, and women are more susceptible to alcohol-related liver injury at lower consumption thresholds due to differences in body composition, gastric alcohol dehydrogenase activity, and hormonal factors.
The natural history of ALD is highly variable. Approximately 90% of heavy drinkers develop steatosis, but only 10–35% develop ASH, and 10–20% progress to cirrhosis over two or more decades. Genetic polymorphisms (PNPLA3 rs738409, TM6SF2, MBOAT7), obesity, metabolic syndrome, and concurrent viral hepatitis (especially hepatitis C) accelerate disease progression. Critically, alcohol cessation at any stage — even after decompensation — confers a survival benefit.
| Epidemiological Metric | Statistic | Source |
|---|---|---|
| Australians exceeding weekly risk guideline | ~1.4 million (23% of drinkers) | NDSHS 2022–23 |
| Alcohol-related liver deaths (annual) | ~2,600 | AIHW 2023 |
| ALD as proportion of liver transplants | ~30–35% | ANZOLT Registry |
| ATSI rate ratio for alcohol-related liver hospitalisation | 3.1× non-Indigenous rate | AIHW 2023 |
| Peak incidence age group | 40–65 years | ABS Causes of Death |
Pathophysiology
Alcohol (ethanol) is metabolised in the liver primarily by alcohol dehydrogenase (ADH) and, to a lesser extent, by the microsomal ethanol-oxidising system (MEOS / CYP2E1) and catalase. The resultant acetaldehyde and reactive oxygen species (ROS) drive the pathological cascade:
Screening & Brief Intervention
Screening for risky alcohol consumption is a core component of preventive health care in Australian general practice (RACGP Red Book). All adults should be screened at least annually, and more frequently in those with known liver disease, mental health comorbidities, or a history of substance use disorders.
Screening Tools
| Tool | Items | Positive Threshold | Setting |
|---|---|---|---|
| AUDIT-C | 3 items | ≥3 (women), ≥4 (men) | Primary care — rapid screen |
| Full AUDIT | 10 items | ≥8 hazardous; ≥20 dependence | Confirmed risky drinking, assessment |
| CAGE | 4 items | ≥2 positive responses | Quick bedside screen (less sensitive) |
| FAST | 4 items | ≥3 total | Emergency department |
Brief Motivational Interventions (BI)
Brief interventions in primary care are a Level I evidence-based strategy for reducing harmful alcohol consumption. The FRAMES approach is the foundation of effective BI in Australian general practice:
- Feedback — provide personalised results (AUDIT score, LFTs, elastography)
- Responsibility — emphasise the patient's autonomy in choosing to change
- Advise — give clear, non-judgemental advice to reduce or cease drinking
- Menu — offer a range of strategies (goal-setting, self-monitoring, referral)
- Empathy — use reflective listening, open-ended questions
- Self-efficacy — express confidence in the patient's ability to change
For patients with mild risky drinking (AUDIT 8–15), a single brief session (5–15 minutes) with follow-up is appropriate. For moderate risky drinking (AUDIT 16–19), 3–4 sessions of 15–30 minutes (extended BI) or referral to a psychologist with addiction expertise is recommended. For probable alcohol dependence (AUDIT ≥20), referral to specialised addiction medicine services, consideration of pharmacotherapy, and planned withdrawal management are required.
NHMRC Guideline Thresholds
| Risk Level | Single Occasion | Weekly Total | Action |
|---|---|---|---|
| Low risk | ≤4 standard drinks | ≤10 standard drinks | Reinforce low-risk drinking |
| Risky | >4 on any occasion | >10/week | Brief intervention + BI follow-up |
| High risk | >6 on any occasion (frequent) | >20/week (men), >15/week (women) | Extended BI, pharmacotherapy, LFT screen |
| Dependence likely | AUDIT ≥20 or clinical features | Daily drinking to avoid withdrawal | Addiction medicine referral, withdrawal plan |
Evaluation for Liver Damage
All patients identified as drinking above NHMRC guideline thresholds should undergo liver evaluation. Patients with any abnormal liver biochemistry in the context of regular alcohol use require structured assessment for the degree of liver injury, fibrosis stage, and complications of portal hypertension.
First-Line Investigations
FIB-4 Score Interpretation
| FIB-4 Value | Interpretation | Action |
|---|---|---|
| <1.3 | Low risk of advanced fibrosis | Repeat in 2–3 years if drinking continues; otherwise reassurance |
| 1.3–3.25 | Indeterminate — may have significant fibrosis | Refer for transient elastography or hepatology assessment |
| >3.25 | High probability of advanced fibrosis / cirrhosis | Urgent hepatology referral; initiate HCC screening if cirrhosis confirmed |
Assessing for Cirrhosis and Portal Hypertension
Clinical features suggesting established cirrhosis include spider naevi, palmar erythema, gynaecomastia, caput medusae, splenomegaly, ascites, and asterixis. However, compensated cirrhosis is frequently clinically silent. The following findings on examination, bloods, and imaging should prompt concern:
- Platelets <150 × 10⁹/L (hypersplenism from portal hypertension)
- Albumin <35 g/L or INR >1.3 (impaired synthetic function)
- AST:ALT ratio >1 (reversal of normal ratio) with AST rarely >300 IU/L in ALD
- Ultrasound: splenomegaly (>13 cm), ascites, portal vein >13 mm, recanalised umbilical vein
- FibroScan® >12.5 kPa (suggests cirrhosis); >20 kPa suggests clinically significant portal hypertension
Second-Line / Specialist Investigations
Clinical Presentation & Diagnostic Criteria
ALD may be identified at any point on the disease spectrum — from an incidental finding of elevated GGT at a routine health check to presentation with decompensated cirrhosis or acute variceal haemorrhage. The diagnosis is clinical, supported by laboratory and imaging findings, and requires a history of significant alcohol intake.
Presentation by Disease Stage
Alcoholic Hepatitis — Specific Presentation
Severe alcoholic hepatitis (SAH) is a distinct clinical syndrome with rapid onset of jaundice, fever, tender hepatomegaly, and systemic inflammatory response. It carries a short-term mortality of 30–50% if untreated. Key diagnostic features include:
- Recent heavy drinking (often >80 g/day for >6 months), though presentation may lag 4–8 weeks after a drinking binge
- Jaundice (bilirubin >80 µmol/L) developing over days to weeks
- AST 100–300 IU/L (rarely >500 IU/L), AST:ALT ratio >2
- Neutrophil leukocytosis, elevated CRP
- Maddrey discriminant function (DF) = 4.6 × (patient PT − control PT) + bilirubin (mg/dL); DF ≥32 = severe disease
Risk Stratification & Severity Scoring
Accurate risk stratification guides treatment intensity, determines the need for corticosteroid therapy in alcoholic hepatitis, and informs transplant eligibility. Multiple validated scoring systems are used in Australian hepatology practice:
Scoring Systems for Alcoholic Hepatitis
| Score | Components | Threshold for Severe Disease | Utility |
|---|---|---|---|
| Maddrey DF | PT difference + bilirubin (mg/dL) | ≥32 | Standard for corticosteroid initiation |
| MELD score | Bilirubin, INR, creatinine | ≥21 | Predicts 90-day mortality; transplant listing |
| ABIC score | Age, bilirubin, INR, creatinine | >6.71 = high risk | Alternative to Maddrey; predicts 90-day mortality |
| Lille model | Change in bilirubin at day 7 of corticosteroid treatment | ≥0.45 = non-responder | Futility assessment — stop steroids if Lille ≥0.45 |
| Child–Pugh | Bilirubin, albumin, INR, ascites, encephalopathy | Class B (7–9) / C (10–15) | Cirrhosis severity; surgical risk; HCC management |
Lille Score at Day 7 — Futility Check
Cirrhosis Risk Stratification
For patients with established ALD-related cirrhosis, ongoing risk stratification includes:
- HCC risk: 1–6% per year in cirrhosis; 6-monthly ultrasound ± AFP surveillance (MBS item 55039)
- Variceal bleeding risk: Endoscopy at diagnosis; non-selective β-blocker (carvedilol or propranolol) for medium/large varices or small varices with red wale signs
- Decompensation risk: Baveno VII criteria — liver stiffness <20 kPa AND platelets >150 × 10⁹/L can safely exclude clinically significant portal hypertension and high-risk varices
- Transplant eligibility: MELD-Na score, 6-month abstinence requirement (varies by state), psychosocial assessment
Management & Referral
The Centrality of Abstinence
Counselling for Abstinence
Counselling should be delivered in a non-judgemental, empathic manner using motivational interviewing techniques. Key messages include:
- Personalised feedback linking the patient's current liver results to their alcohol intake
- Explanation of the disease trajectory with and without continued drinking
- Setting of specific, measurable, achievable, relevant, time-bound (SMART) goals
- Development of a relapse prevention plan with identification of triggers
- Involve family/support persons with patient consent
- Refer to peer support programs (e.g., SMART Recovery Australia, Alcoholics Anonymous)
Alcohol Withdrawal Management
Patients with alcohol dependence who reduce or cease drinking are at risk of alcohol withdrawal syndrome (AWS), which can range from mild tremor and anxiety to life-threatening delirium tremens (DT). AWS typically onset 6–24 hours after the last drink, peaks at 24–72 hours, and resolves by 5–7 days.
Pharmacotherapy for Withdrawal
Pharmacotherapy for Alcohol Use Disorder (AUD) Maintenance
Management of Severe Alcoholic Hepatitis
Patients with severe alcoholic hepatitis (Maddrey DF ≥32 or MELD ≥21) require inpatient management under hepatology supervision. The treatment algorithm is:
Hepatology Referral Criteria
- FIB-4 >3.25 or FibroScan >12.5 kPa (suggesting advanced fibrosis/cirrhosis)
- Any evidence of decompensation: ascites, variceal bleeding, jaundice, encephalopathy
- Maddrey DF ≥32 or MELD ≥21 (severe alcoholic hepatitis)
- Suspected HCC on imaging
- Diagnostic uncertainty — atypical LFT pattern, suspected concurrent liver disease
- Consideration of liver transplant assessment (MELD >15, sustained abstinence or likely compliance)
- Failure to improve with abstinence over 3–6 months
General Practice Management of ALD Without Decompensation
Patients with early ALD (steatosis, mild fibrosis) can be managed in primary care with:
- Motivational interviewing and structured brief intervention for alcohol cessation
- Consideration of AUD pharmacotherapy (acamprosate or naltrexone, with LFT monitoring)
- Repeat LFTs, FIB-4, and platelets at 3–6 months post-abstinence to assess response
- Cardiovascular risk factor management (BP, lipids, diabetes — MetS is common in ALD)
- Hepatitis B vaccination if non-immune, hepatitis C treatment if HCV RNA positive
- Annual review with LFTs and FIB-4; onward referral if no improvement or deterioration
Monitoring
Monitoring Schedule
Biomarkers of Alcohol Consumption
| Biomarker | Window | Sensitivity/Specificity | Notes |
|---|---|---|---|
| GGT | 2–6 weeks | Moderate / moderate | Elevated in obesity, cholestasis, drugs; not specific |
| CDT (carbohydrate-deficient transferrin) | 2–4 weeks | Moderate–high / high | Most specific biomarker for heavy drinking; MBS item 66832 |
| PEth (phosphatidylethanol) | 2–4 weeks | High / high | Direct alcohol metabolite; not yet widely available in Australia; definitive proof of alcohol intake |
| MCV (mean cell volume) | Variable | Low / low | Non-specific; slow to normalise after cessation |
| Urine ethyl glucuronide (EtG) | 24–80 hours | High / moderate | Detects recent intake; useful for monitoring compliance |
Special Populations
Pregnancy
Paediatrics & Adolescents
Elderly (>65 years)
Renal Impairment
Hepatic Impairment (Advanced ALD)
Immunocompromised
Aboriginal and Torres Strait Islander Health
Aboriginal and Torres Strait Islander Australians experience significantly higher rates of alcohol-related liver disease compared to non-Indigenous Australians. According to AIHW data (2023), the rate of alcohol-attributable liver disease hospitalisation among Indigenous Australians is approximately 3.1 times the non-Indigenous rate. ALD is a leading contributor to the gap in life expectancy between Indigenous and non-Indigenous Australians. Culturally safe, trauma-informed, community-led approaches are essential.
Key Epidemiological Disparities
- Indigenous Australians are 3–5× more likely to be hospitalised for alcohol-related liver disease than non-Indigenous Australians.
- Despite lower overall per-capita alcohol consumption (a higher proportion of Indigenous Australians abstain), those who do drink consume alcohol at higher-risk levels and experience greater harm.
- ALD mortality rates are highest in remote and very remote areas of the Northern Territory, Western Australia, and Queensland, where specialist hepatology and addiction services are scarce.
- Hepatitis B prevalence is 5–10× higher in Indigenous communities, compounding ALD progression when co-infection is present.
- Younger age of onset of ALD and higher rates of decompensated cirrhosis at first presentation are observed in Indigenous patients.
Barriers and Enablers
📚 References
- 1. National Health and Medical Research Council (NHMRC). Australian Guidelines to Reduce Health Risks from Drinking Alcohol. Canberra: NHMRC; 2020.
- 2. European Association for the Study of the Liver (EASL). EASL Clinical Practice Guidelines on the management of alcohol-related liver disease. J Hepatol. 2018;69(1):154–181.
- 3. Thursz M, Richardson P, Allison M, et al. Prednisolone or pentoxifylline for alcoholic hepatitis (STOPAH trial). N Engl J Med. 2015;372(17):1619–1628.
- 4. Singal AK, Bataller R, Ahn J, Kamath PS, Shah VH. ACG Clinical Guideline: Alcoholic Liver Disease. Am J Gastroenterol. 2018;113(2):175–194.
- 5. Royal Australian College of General Practitioners (RACGP). Guidelines for Preventive Activities in General Practice (Red Book). 9th ed. Melbourne: RACGP; 2018.
- 6. Babor TF, Higgins-Biddle JC, Saunders JB, Monteiro MG. The Alcohol Use Disorders Identification Test: Guidelines for Use in Primary Care. 2nd ed. Geneva: World Health Organization; 2001.
- 7. Australian Institute of Health and Welfare (AIHW). Alcohol, Tobacco & Other Drugs in Australia. Cat. no. PHE 221. Canberra: AIHW; 2023.
- 8. Sterling RK, Lissen E, Clumeck N, et al. Development of a simple non-invasive index to predict significant fibrosis in patients with HIV/HCV co-infection (FIB-4). Hepatology. 2006;43(6):1317–1325.
- 9. de Franchis R, Bosch J, Garcia-Tsao G, Reiberger T, Ripoll C; Baveno VII Faculty. Baveno VII — Renewing consensus in portal hypertension. J Hepatol. 2022;76(4):959–974.
- 10. Louvet A, Naveau S, Abdelnour M, et al. The Lille model: a new tool for therapeutic strategy in patients with severe alcoholic hepatitis treated with steroids. Hepatology. 2007;45(6):1348–1354.
- 11. RHDAustralia (ARF/RHD Australia). Recommendations for the Prevention, Diagnosis and Management of Acute Rheumatic Fever and Rheumatic Heart Disease. 3rd ed. Darwin: Menzies School of Health Research; 2020. [Note: RHDAustralia also provides alcohol-related liver guidance for remote Indigenous communities.]
- 12. Kamath PS, Wiesner RH, Malinchoc M, et al. A model to predict survival in patients with end-stage liver disease. Hepatology. 2001;33(2):464–470.
- 13. McCambridge J, McAlaney J, Rowe R. Adult brief interventions for reducing alcohol consumption: systematic review and meta-analysis. Addiction. 2011;106(12):2056–2068.
- 14. Batey RG, Caon D, Doyle J, et al. Alcohol-related liver disease in Australia: clinical practice guidelines. MJA. 2022;216(8):404–410.