📋 Key Information Summary
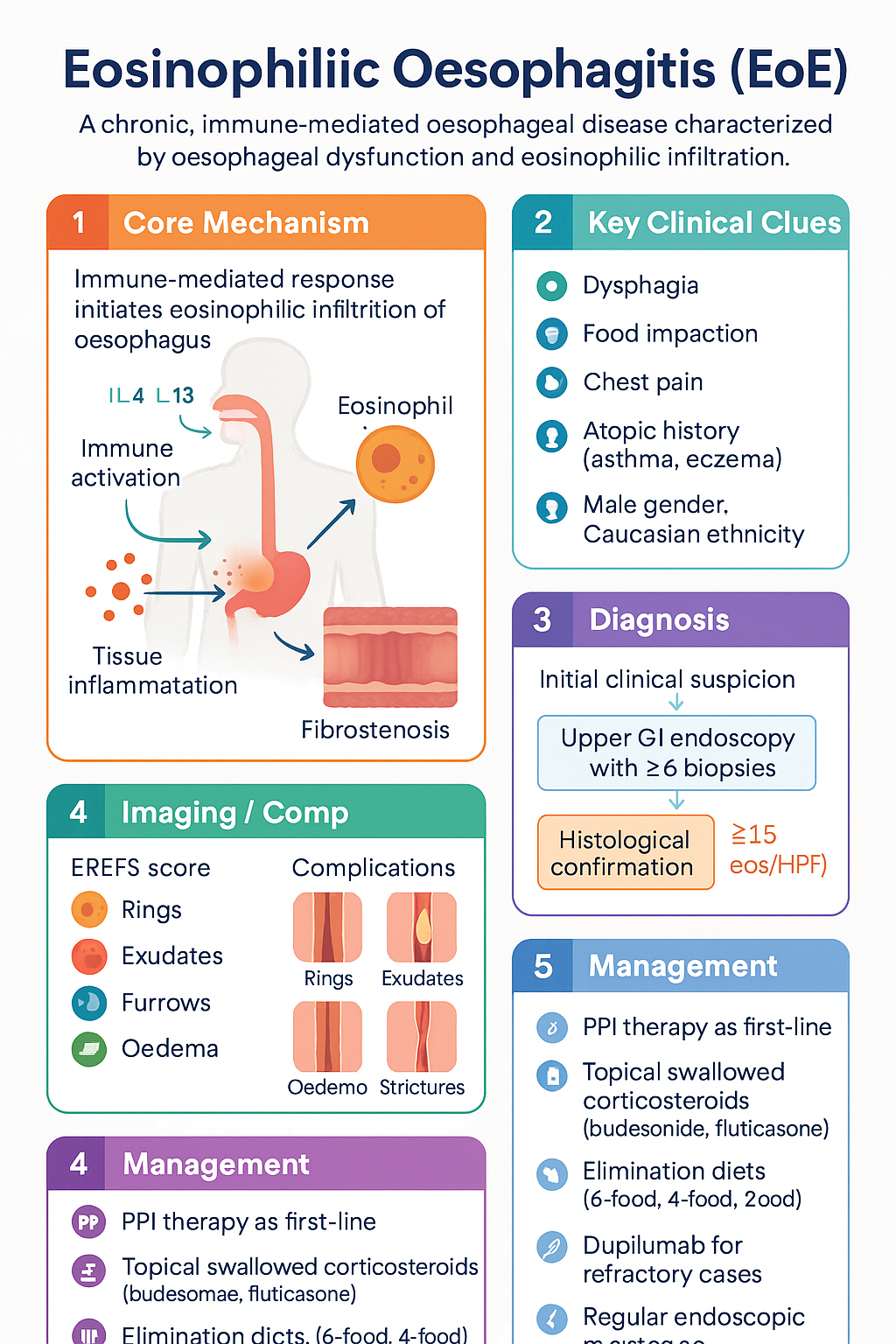
- Definition: Eosinophilic oesophagitis (EoE) is a chronic, immune-mediated oesophageal disease characterised by symptoms of oesophageal dysfunction and ≥15 eosinophils per high-power field (eos/HPF) on oesophageal biopsy, after exclusion of secondary causes.
- Epidemiology: Rising incidence in Australia (estimated 1 in 100–500 adults; peak prevalence in Caucasian males aged 30–50 years). Increasingly recognised in children and adolescents.
- Diagnosis requires: Upper GI endoscopy with ≥6 biopsies from both proximal and distal oesophagus showing ≥15 eos/HPF, plus exclusion of PPI-responsive oesophageal eosinophilia (PPI-REE) and other secondary causes of oesophageal eosinophilia.
- PPI therapy is now part of EoE treatment: PPIs are no longer solely a diagnostic exclusion criterion — they are considered first-line therapy for EoE in their own right, with up to 50% histological response rates.
- Topical swallowed corticosteroids (TSC): Budesonide orodispersible tablet (Jorveza®) or swallowed fluticasone propionate from an MDI are the cornerstone pharmacological treatments, with histological remission rates of 50–70%.
- Elimination diets: Empiric elimination diets (6-food, 4-food, or 2-food) are effective alternatives, with step-up or step-down approaches guided by endoscopic and histological response.
- Dupilumab: Now PBS-listed (Authority Required) for moderate-to-severe EoE in adults and adolescents ≥12 years refractory to at least one standard therapy.
- Treatment targets: The goal is histological remission (<15 eos/HPF, ideally <6 eos/HPF), symptomatic improvement, and endoscopic remission (normalised EREFS score).
- Monitoring: Repeat endoscopy with biopsies 8–12 weeks after initiating or changing therapy; then periodic surveillance for long-term maintenance patients.
- Complications: Progressive fibrostenosis leads to oesophageal strictures and food impaction. Endoscopic oesophageal dilation is required for symptomatic strictures unresponsive to medical therapy.
- Maintenance therapy: Most patients require long-term maintenance treatment to prevent relapse; abrupt cessation of therapy typically results in recurrence of eosinophilia and symptoms within weeks.
- ATSI considerations: EoE data in Aboriginal and Torres Strait Islander populations are limited; access to endoscopy and specialist gastroenterology services in remote and regional Australia remains a significant barrier.
🎧 Audio Brief
Diagnosis
The diagnosis of EoE is based on the presence of oesophageal symptoms accompanied by oesophageal mucosal eosinophilia, after exclusion of other causes. Updated 2024 guidelines from the International Gastrointestinal Eosinophil Research (TIGERS) consortium and AGREE consensus provide the current framework.
Histological Criteria
The hallmark of EoE is the presence of ≥15 eosinophils per high-power field (eos/HPF) in at least one oesophageal biopsy specimen, in the absence of secondary causes of oesophageal eosinophilia. This threshold has been validated in both adult and paediatric populations across multiple international studies.
Additional histological features that support the diagnosis include eosinophil microabscesses, surface layering of eosinophils, eosinophil degranulation, basal zone hyperplasia, and dilated intercellular spaces. These features should be reported by the pathologist even if the 15 eos/HPF threshold is not met in all specimens.
Endoscopic Features — EREFS Classification
The Endoscopic Reference Score (EREFS) system standardises the reporting of endoscopic findings in EoE. The following five features are each graded from 0 (absent) to 3 (severe):
| EREFS Feature | Description | Grade 0 | Grade 1 | Grade 2 | Grade 3 |
|---|---|---|---|---|---|
| R — Rings | Concentric mucosal rings | None | Mild (visible with insufflation) | Moderate (persistent) | Severe (non-traversable) |
| E — Exudates | White plaques or spots | None | Mild (<10% surface) | Moderate (10–30%) | Severe (>30%) |
| E — Furrows | Linear longitudinal grooves | None | Mild | Moderate | Severe |
| F — Oedema (Fr) | Mucosal oedema / loss of vascularity | None | Mild | Moderate | Severe |
| S — Strictures | Fixed luminal narrowing | None | Mild (≥14 mm) | Moderate (10–13 mm) | Severe (<10 mm) |
The EREFS score correlates with histological disease severity and can be used to track response to therapy. A total EREFS score ≤2 is considered endoscopic remission. Note that a normal-appearing oesophagus at endoscopy does not exclude EoE — up to 25% of patients with confirmed EoE have a macroscopically normal mucosa, underscoring the importance of systematic biopsies.
Exclusion of Secondary Oesophageal Eosinophilia
Before a diagnosis of EoE can be confirmed, secondary causes of oesophageal eosinophilia must be excluded. The following differential diagnoses should be considered and addressed:
| Secondary Cause | Key Differentiating Features |
|---|---|
| Gastro-oesophageal reflux disease (GORD) | Usually <15 eos/HPF; responds to PPI therapy; distal oesophagus predominant |
| PPI-responsive oesophageal eosinophilia (PPI-REE) | Now considered part of the EoE spectrum; PPIs are therapeutic, not just diagnostic |
| Hypereosinophilic syndrome | Peripheral eosinophilia >1500/μL; multi-organ involvement; cardiac risk |
| Achalasia | Oesophageal manometry shows failed peristalsis and incomplete LES relaxation |
| Crohn's disease | Usually colonic or ileal involvement; granulomas on biopsy |
| Connective tissue disorders | Scleroderma — oesophageal hypomotility; systemic features present |
| Drug hypersensitivity | Temporal relationship to drug exposure (e.g., azathioprine, tacrolimus) |
| Parasitic infection | Stool ova, cysts, and parasites; Strongyloides serology in at-risk patients |
Diagnostic Investigations
Treatment
The goals of EoE treatment are to achieve histological remission (<15 eos/HPF, ideally <6 eos/HPF), resolve symptoms, and prevent fibrostenotic complications. Treatment options include PPI therapy, topical swallowed corticosteroids, elimination diets, and biologic therapy. Choice of initial therapy depends on disease severity, patient preference, comorbidities, and access.
PPI Therapy — First-Line
PPIs are now considered a first-line treatment for EoE, not merely a diagnostic exclusion tool. Approximately 30–50% of patients with oesophageal eosinophilia achieve histological remission with PPI monotherapy. The mechanism involves both acid suppression and direct anti-eosinophilic effects (reduction of eotaxin-3, inhibition of IL-4/IL-13 signalling).
Topical Swallowed Corticosteroids (TSC)
If PPI therapy is insufficient, or as first-line in moderate-to-severe disease, topical swallowed corticosteroids are the mainstay of pharmacological treatment. These agents deliver corticosteroid directly to the oesophageal mucosa with minimal systemic absorption. Histological remission rates range from 50–70%.
Elimination Diets
Empiric elimination diets are an effective, drug-free alternative for EoE management, particularly in motivated patients and those wishing to avoid long-term corticosteroids. Histological remission rates vary by approach: 6-food elimination ~70%, 4-food ~60%, 2-food ~45%.
Protocol: Foods are eliminated for 6 weeks, followed by repeat endoscopy with biopsies. If histological remission is confirmed, foods are reintroduced sequentially (one food group every 6–8 weeks) with repeat endoscopy after each reintroduction to identify triggers. Dietitian involvement is essential to ensure nutritional adequacy, particularly in children.
Dupilumab — Biologic Therapy for Refractory EoE
Dupilumab (Dupixent®) is a fully human monoclonal antibody targeting IL-4Rα, thereby blocking both IL-4 and IL-13 signalling — key drivers of type 2 inflammation in EoE. It is approved by the TGA and listed on the PBS (Authority Required) for moderate-to-severe EoE in adults and adolescents ≥12 years who are refractory to, intolerant of, or have contraindications to at least one standard treatment (PPI, TSC, or elimination diet).
Treatment Algorithm — Step-Up Approach
Monitoring & Complications
Response Assessment — Repeat Endoscopy
All patients should undergo repeat upper GI endoscopy with oesophageal biopsies 8–12 weeks after initiating or changing therapy. This is the gold standard for assessing treatment response. Symptom assessment alone is unreliable — many patients have discordance between symptoms and histological activity, particularly adults who may have adapted to chronic dysphagia.
Treatment Targets
Updated consensus guidelines define three domains of remission, all of which should be assessed:
Long-Term Maintenance
EoE is a chronic, relapsing condition. Histological relapse occurs in the majority of patients within weeks to months of discontinuing therapy. Long-term maintenance therapy is therefore recommended for most patients, using the lowest effective dose of the treatment that induced remission.
Complications
Untreated or poorly controlled EoE can lead to progressive oesophageal remodelling and fibrosis, resulting in significant morbidity:
| Complication | Management |
|---|---|
| Food bolus impaction | Urgent endoscopic retrieval (MBS Item 30475). Emergent flexible endoscopy preferred over rigid oesophagoscopy in most centres. Consider general anaesthesia if prolonged impaction >24 hours. After resolution, schedule follow-up endoscopy + biopsies to confirm EoE diagnosis and initiate therapy. |
| Fibrostenotic strictures | Endoscopic oesophageal dilation (bougie or balloon). Serial dilations in increments of 1–2 mm to minimise perforation risk (perforation rate <1% when performed by experienced endoscopists). Always combine with medical therapy — dilation alone does not address the underlying inflammatory process. |
| Oesophageal perforation | Rare (<0.5% of dilations in experienced hands). Suspect if chest pain, crepitus, or haemodynamic instability post-dilation. Urgent CT thorax with oral contrast. Surgical consultation for contained perforation; emergency surgery for free perforation. |
| Subepithelial fibrosis | Often clinically silent in early stages. Detected by EREFS scoring (rings, strictures) and functional luminal imaging probe (EndoFLIP, specialist centres). Emphasises the importance of early, effective anti-inflammatory therapy to prevent irreversible remodelling. |
Oesophageal Dilation
Endoscopic oesophageal dilation is indicated for patients with symptomatic fibrostenotic strictures that fail to resolve with medical therapy alone. Key principles:
- Always combine with ongoing anti-inflammatory therapy (PPI, TSC, or dupilumab)
- Use bougie (Savary-Gilliard) or balloon dilation based on operator expertise and stricture characteristics
- Serial sessions preferred — dilate by 1–2 mm per session to minimise mucosal tears and perforation risk
- Target diameter of 15–17 mm is generally sufficient for symptom resolution
- Post-procedure: observe for 2–4 hours; soft diet for 24 hours; paracetamol for discomfort
Special Populations
📚 References
- 1. Hirano I, Chan ES, Rank MA, et al. AGA Institute and the Joint Task Force on Allergy-Immunology Practice Parameters Clinical Guidelines for the Management of Eosinophilic Esophagitis. Gastroenterology. 2020;158(6):1776–1786.
- 2. Lucendo AJ, Molina-Infante J, Arias Á, et al. Guidelines on eosinophilic esophagitis: evidence-based statements and recommendations for diagnosis and management in children and adults. United European Gastroenterol J. 2017;5(3):335–358.
- 3. Dellon ES, Liacouras CA, Molina-Infante J, et al. Updated International Consensus Diagnostic Criteria for Eosinophilic Esophagitis: Proceedings of the AGREE Conference. Gastroenterology. 2018;155(4):1022–1033.e10.
- 4. Molina-Infante J, Bredenoord AJ, Cheng E, et al. Proton pump inhibitor-responsive oesophageal eosinophilia: an entity challenging current diagnostic criteria for eosinophilic oesophagitis. Gut. 2016;65(3):524–531.
- 5. Hirano I, Moy N, Heckman MG, et al. Endoscopic assessment of the oesophageal features of eosinophilic oesophagitis: validation of a novel classification and grading system. Gut. 2013;62(4):489–495.
- 6. Miehlke S, Lucendo AJ, Straumann A, et al. Budesonide orodispersible tablets for induction and maintenance of remission in adult patients with eosinophilic esophagitis. Lancet Gastroenterol Hepatol. 2022;7(9):838–849.
- 7. Hirano I, Collins MH, Assouline-Dayan Y, et al. Dupilumab efficacy and safety in adults and adolescents with eosinophilic oesophagitis: a randomised, double-blind, placebo-controlled, phase 3 trial (Part A). Lancet. 2022;400(10363):1553–1565.
- 8. Molina-Infante J, Arias Á, Alcedo J, et al. Step-up approach for eosinophilic oesophagitis based on a randomised controlled trial. Gut. 2018;67(12):2130–2137.
- 9. Warners MJ, Vlieg-Boerstra BJ, Verheij J, et al. Elemental and elimination diet in adult eosinophilic oesophagitis. Aliment Pharmacol Ther. 2017;45(4):544–554.
- 10. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander health performance framework: Gastrointestinal diseases. Canberra: AIHW; 2023.
- 11. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.
- 12. Philpott H, Nandurkar S, Royce SG, et al. Allergic eosinophilic gastrointestinal disease in Australia: an update on prevalence, diagnosis, and management. Intern Med J. 2019;49(10):1240–1246.