📋 Key Information Summary
- Drug-induced cholestasis is a significant cause of acute liver injury in Australia, accounting for an estimated 2–5% of jaundice presentations to gastroenterology services.
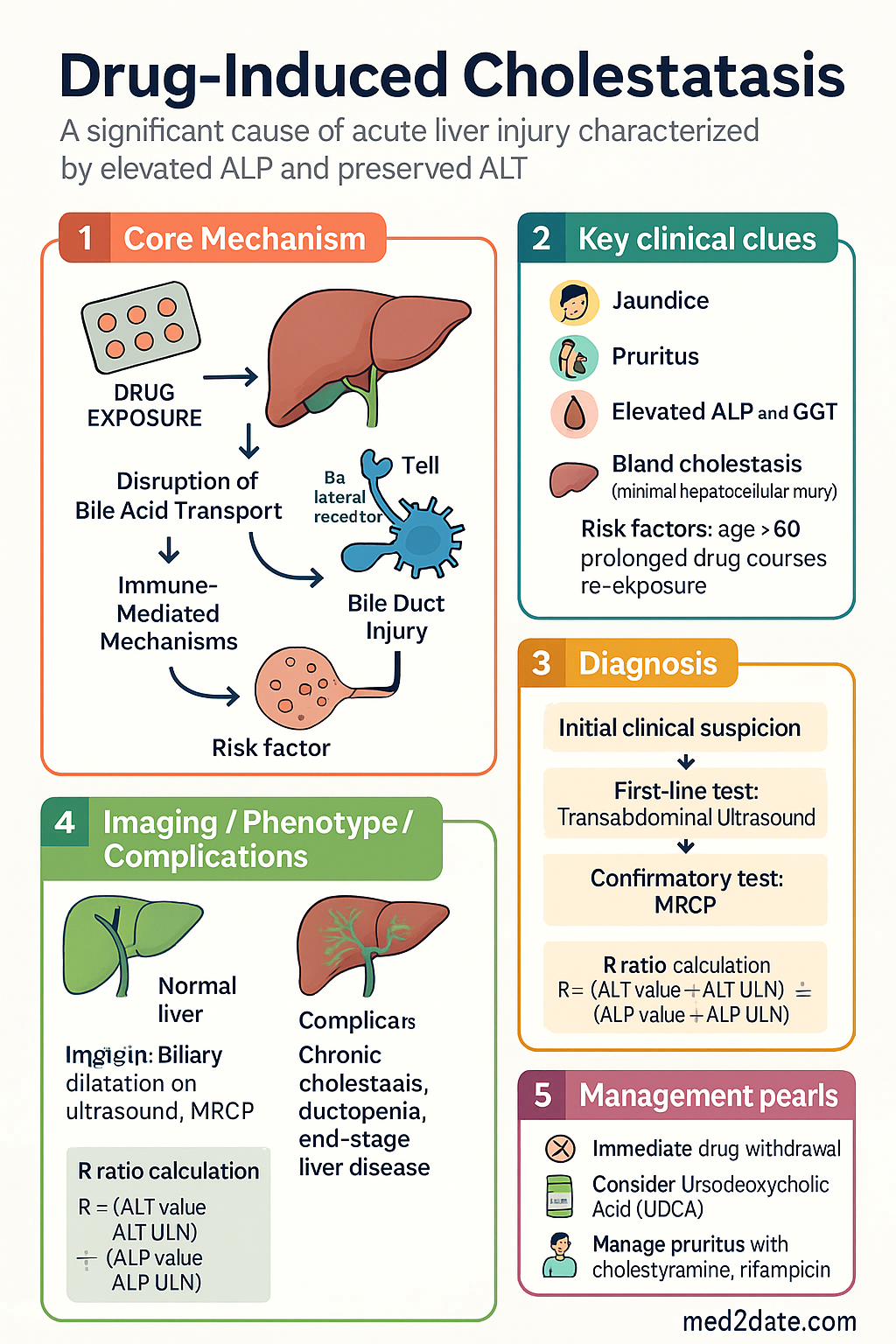
- The cholestatic biochemical pattern is defined by a predominantly elevated alkaline phosphatase (ALP) with a relatively preserved alanine aminotransferase (ALT); the R ratio (ALT/ULN ÷ ALP/ULN) is <2.
- Amoxicillin-clavulanate is the most frequently implicated drug in Australia, often presenting 1–2 weeks after cessation of therapy; prolonged courses and re-exposure increase risk.
- Flucloxacillin cholestasis may present weeks to months after the drug has been stopped, making temporal association difficult; HLA-B*5701 testing may identify at-risk individuals.
- Oestrogens, combined oral contraceptives, and anabolic-androgenic steroids cause bland cholestasis without significant hepatocellular necrosis; genetic susceptibility (e.g., ABCB4 variants) may predispose.
- Chlorpromazine and erythromycin estolate are classical cholestatic agents; onset is typically 1–4 weeks after initiation.
- Azathioprine can cause cholestatic hepatitis and nodular regenerative hyperplasia, particularly in transplant and inflammatory bowel disease populations.
- Immune checkpoint inhibitors (nivolumab, pembrolizumab, ipilimumab) are increasingly recognised causes of immune-mediated cholestatic hepatitis (immune-mediated cholangitis) in oncology patients.
- Biliary obstruction must be excluded with transabdominal ultrasound and, if inconclusive, MRCP before attributing cholestasis to a drug.
- Liver biopsy is indicated when cholestasis persists beyond 3–6 months after drug withdrawal or when diagnostic doubt exists (e.g., to detect ductopenia or vanishing bile duct syndrome).
- The cornerstone of management is immediate withdrawal of the offending drug; ursodeoxycholic acid (UDCA) may provide benefit but evidence is limited.
- Pruritus associated with cholestasis can be severe; management includes cholestyramine, rifampicin, and specialist referral for refractory cases.
- A small proportion of patients develop prolonged or chronic cholestasis with ductopenia; some may progress to end-stage liver disease requiring liver transplantation.
- Timely recognition, cessation of the causative agent, and specialist hepatology involvement are essential to minimise morbidity and mortality.
Common Drugs Causing Cholestasis
Drug-induced cholestasis results from disruption of bile acid transport, bile duct injury, or immune-mediated mechanisms. The following agents are the most clinically relevant causes encountered in Australian practice.
Amoxicillin–Clavulanate
Amoxicillin–clavulanate is the single most common cause of drug-induced liver injury (DILI) worldwide and in Australia. Cholestatic or mixed hepatocellular-cholestatic patterns predominate. Onset typically occurs during or 1–2 weeks after cessation of therapy, although delayed presentations up to 6 weeks have been reported. The clavulanic acid component is thought to be primarily responsible. Risk factors include increasing age, repeated courses, and underlying liver disease.
Flucloxacillin
Flucloxacillin cholestasis may present weeks to months after the drug has been discontinued, making the temporal relationship difficult to establish. This delayed onset is a well-recognised pitfall in clinical practice. The HLA-B*5701 genotype confers a marked increase in risk (up to 80-fold in some studies). Although HLA typing is not yet routine for flucloxacillin prescribing, clinicians should consider this association when encountering unexplained cholestasis with a history of flucloxacillin use.
Oestrogens and Combined Oral Contraceptives
Oestrogens, particularly ethinyloestradiol in combined oral contraceptive pills (COCPs), cause a bland cholestasis characterised by pruritus and elevated ALP with minimal hepatocellular injury. The mechanism involves inhibition of the bile salt export pump (BSEP/ABCB11) and multidrug resistance-associated protein 2 (MRP2). Women with mutations in the ABCB4 gene (encoding MDR3/MDR P-glycoprotein 3) are at increased risk. Pregnancy-related cholestasis (intrahepatic cholestasis of pregnancy) shares a similar pathophysiology. Cholestasis is typically reversible within weeks of oestrogen withdrawal.
Anabolic-Androgenic Steroids
Anabolic-androgenic steroids (AAS), including testosterone analogues and 17α-alkylated steroids used in bodybuilding and sports, produce a pure bland cholestasis with profound pruritus and jaundice. Biochemically, ALP may be only mildly elevated while bilirubin rises markedly. Histologically, bile plugs are seen within dilated canaliculi with minimal inflammation—a pattern termed "bland cholestasis." Cholestasis may persist for weeks to months after cessation. 17α-alkylated agents (e.g., stanozolol, methyltestosterone) are particularly hepatotoxic.
Chlorpromazine
Chlorpromazine is a classical cause of drug-induced cholestasis. Jaundice develops in approximately 1–2% of patients within 2–4 weeks of commencing therapy, although subclinical ALP elevation occurs in up to 40%. Histological features include bile stasis, portal inflammation with eosinophils, and bile duct injury. Most cases resolve within weeks of drug withdrawal, but chronic cholestasis with ductopenia may occasionally develop.
Erythromycin Estolate
Erythromycin estolate is associated with a hypersensitivity-type cholestatic hepatitis characterised by fever, right upper quadrant pain, and eosinophilia. The estolate salt is more hepatotoxic than other erythromycin formulations. Cholestasis usually resolves within days to weeks of cessation. This reaction is idiosyncratic and not dose-related. In Australia, erythromycin stearate and ethylsuccinate are more commonly used and have a lower hepatotoxicity risk.
Azathioprine
Azathioprine causes cholestatic hepatitis in approximately 2–3% of patients, typically within the first 3–6 months of therapy. It is also associated with nodular regenerative hyperplasia (NRH) and sinusoidal obstruction syndrome with long-term use. TPMT (thiopurine methyltransferase) and NUDT15 genotyping should be performed prior to initiation to guide dosing and reduce hepatotoxicity risk. Australian guidelines recommend baseline and serial LFT monitoring in the first 3 months. Cholestasis generally resolves with dose reduction or drug withdrawal.
Immune Checkpoint Inhibitors
Immune checkpoint inhibitors (ICIs) including nivolumab, pembrolizumab, ipilimumab, and atezolizumab are increasingly used in Australian oncology practice. Immune-mediated cholangitis (IMC) is a recognised but relatively rare hepatobiliary adverse event, distinct from classical immune-mediated hepatitis (which is hepatocellular). IMC presents with a cholestatic biochemical pattern (elevated ALP and GGT) ± biliary dilatation on imaging, without mechanical obstruction. Management involves corticosteroids ± mycophenolate mofetil as per ASCO/NCCN toxicity management guidelines. Severe cases may require permanent ICI discontinuation and specialist hepatology and oncology review.
Diagnosis & Management
Cholestatic LFT Pattern
Drug-induced cholestasis is identified by a characteristic biochemical pattern on liver function tests:
- Elevated alkaline phosphatase (ALP): Predominant abnormality; values typically >2× upper limit of normal (ULN).
- Elevated gamma-glutamyl transferase (GGT): Confirms hepatobiliary origin of ALP elevation.
- Elevated conjugated (direct) bilirubin: Indicates impaired bile excretion.
- Relatively preserved ALT: ALT is elevated but less than ALP elevation.
- R ratio <2: Calculated as (ALT/ULN) ÷ (ALP/ULN). An R ratio <2 defines a cholestatic pattern; 2–5 defines mixed; >5 defines hepatocellular.
Exclude Biliary Obstruction
Before attributing cholestasis to a drug, mechanical biliary obstruction must be excluded:
Causality Assessment
Drug causality in cholestasis is assessed using the Roussel Uclaf Causality Assessment Method (RUCAM) score, which evaluates temporal relationship, course after drug withdrawal, risk factors, concomitant drugs, exclusion of other causes, and previous information on the drug. A RUCAM score ≥6 indicates a "probable" drug reaction; ≥8 is "highly probable." In clinical practice, the diagnosis is often one of exclusion.
Liver Biopsy
Liver biopsy is not required in all cases but is indicated in the following circumstances:
- Cholestasis persists beyond 3–6 months after drug withdrawal.
- Diagnostic uncertainty — to exclude primary biliary cholangitis (PBC), primary sclerosing cholangitis (PSC), autoimmune hepatitis, infiltrative disease, or granulomatous hepatitis.
- Suspected vanishing bile duct syndrome (progressive loss of interlobular bile ducts).
- Need to assess severity of bile duct injury or fibrosis.
Key histological findings:
- Bland cholestasis: Bile plugs in dilated canaliculi with minimal inflammation (oestrogens, AAS).
- Cholestatic hepatitis: Cholestasis with portal/lobular inflammation and eosinophilic infiltrate (chlorpromazine, erythromycin).
- Ductopenia: Loss of interlobular bile ducts in >50% of portal tracts — indicates vanishing bile duct syndrome; poor prognosis.
- Nodular regenerative hyperplasia: Diffuse nodularity without fibrosis (azathioprine).
Management
1. Drug Withdrawal
Immediate cessation of the offending drug is the most important intervention. In most cases, cholestasis resolves within weeks to months. The drug should be documented in the patient's allergy/adverse drug reaction record in My Health Record and the hospital EMR.
2. Ursodeoxycholic Acid (UDCA)
UDCA has cytoprotective, anti-apoptotic, and choleretic properties. It is established therapy for primary biliary cholangitis and is used off-label in drug-induced cholestasis. Evidence for efficacy in drug-induced cholestasis is limited to case series and observational data; randomised controlled trials are lacking. Despite this, UDCA is commonly prescribed in Australian hepatology practice for persistent cholestasis after drug withdrawal. It is generally well tolerated; diarrhoea is the most common side effect.
3. Symptomatic Pruritus Management
Cholestatic pruritus can be debilitating and significantly impair quality of life. A stepwise approach is recommended:
4. Monitoring & Follow-Up
- Repeat LFTs every 2–4 weeks after drug withdrawal to assess trajectory.
- Resolution is expected within 1–3 months for most agents.
- Persistent elevation beyond 3–6 months warrants liver biopsy to evaluate for vanishing bile duct syndrome, underlying PBC, or PSC.
- Chronic cholestasis may progress to secondary biliary cirrhosis and portal hypertension.
5. Liver Transplantation
A small subset of patients with drug-induced cholestasis develop irreversible bile duct loss (vanishing bile duct syndrome) or progressive hepatic failure. Referral to a liver transplant centre is indicated for:
- Chronic cholestasis with ductopenia unresponsive to medical therapy.
- Progressive hepatic synthetic failure (declining albumin, rising INR).
- Development of complications of portal hypertension (varices, ascites).
- Intractable pruritus refractory to all pharmacological measures.
Liver transplantation outcomes in drug-induced cholestasis are generally favourable if performed before irreversible complications develop. Australia's liver transplant centres are located at Royal Prince Alfred Hospital (Sydney), Austin Hospital (Melbourne), Princess Alexandra Hospital (Brisbane), Sir Charles Gairdner Hospital (Perth), and Flinders Medical Centre (Adelaide).
Special Populations
Aboriginal and Torres Strait Islander Health
📚 References
- 1. Björnsson ES, Bergmann OM, Björnsson HK, et al. Incidence, presentation, and outcomes in patients with drug-induced liver injury in the general population of Iceland. Gastroenterology. 2013;144(7):1419-1425.
- 2. Daly AK, Donaldson PT, Bhatnagar P, et al. HLA-B*5701 genotype is a major determinant of drug-induced liver injury due to flucloxacillin. Nat Genet. 2009;41(7):816-819.
- 3. Chalasani N, Bonkovsky HL, Fontana R, et al. Features and outcomes of 899 patients with drug-induced liver injury: the DILIN prospective study. Gastroenterology. 2015;148(7):1340-1352.
- 4. Lucena MI, Molokhia M, Shen Y, et al. Susceptibility to amoxicillin-clavulanate-induced liver injury is influenced by multiple HLA class I and II alleles. Gastroenterology. 2011;141(1):338-347.
- 5. De Valle MB, Av Klinteberg V, Alem N, et al. Drug-induced liver injury in a Swedish university hospital out-patient hepatology clinic. Aliment Pharmacol Ther. 2006;24(8):1187-1195.
- 6. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander health performance framework 2020 summary report. Canberra: AIHW; 2020.
- 7. Danan G, Benichou C. Causality assessment of adverse reactions to drugs—I. A novel method based on the conclusions of international consensus meetings: application to drug-induced liver injuries. J Clin Epidemiol. 1993;46(11):1323-1330.
- 8. Kubisa S, Niewiński G, Kubisa MJ. Immune-mediated cholangitis and cholangiopathy induced by immune checkpoint inhibitors — a systematic review. Cancers (Basel). 2023;15(5):1508.
- 9. Poupon R, Chazouillères O, Balkau B, et al. Clinical and biochemical features of ursodeoxycholic acid responsive primary biliary cholangitis. Hepatology. 2019;70(4):1207-1217.
- 10. Bolier AR, Elferink RPO, Beuers U. Advances in pathogenesis and treatment of pruritus. Clin Liver Dis. 2013;17(2):319-329.
- 11. Brahmania M, Lombardero M, Hansen BE, et al. Post-transplant hepatotoxicity: azathioprine-related cholestasis and nodular regenerative hyperplasia. Transplantation. 2015;99(1):e1-e5.
- 12. Remote Area Health Corps (RAHC). CARPA Remote Primary Health Care Manuals. 7th ed. Alice Springs: Central Australian Rural Practitioners Association; 2020.